Page 1 of 34
PE26.1 | Approach to Anaemia — SDL Guide
Learning Objectives
- Define anaemia and apply age-specific haemoglobin cut-offs to identify it in children
- Classify anaemia using MCV into microcytic, normocytic, and macrocytic categories with their common paediatric causes
- Take a focused history and perform a clinical examination to assess a child with anaemia
- Use RBC indices, peripheral smear findings, and the Mentzer index to narrow the differential diagnosis
- Outline initial management and indications for packed-cell transfusion in paediatric anaemia
INSTRUCTIONS
Anaemia is the most common haematological problem in children worldwide, and India carries a disproportionately high burden — over 50% of children under five are anaemic by National Family Health Survey data. A systematic, MCV-based approach prevents diagnostic error, avoids unnecessary investigations, and ensures that common causes like iron deficiency and haemolytic conditions are neither missed nor conflated. This module builds the foundational framework you will apply in every subsequent SDL on specific anaemia types.
References
- Ghai Essential Pediatrics, 9th ed, Ch 17 (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 482 (textbook)
- IAP Guidelines on Management of Childhood Anaemia, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old girl is brought to the outpatient department by her mother, who says the child has been 'looking pale and tired' for the past three months. The child attends a government-run anganwadi and eats mainly rice, dal, and vegetables — rarely meat or eggs. On examination, you note severe conjunctival pallor, mild tachycardia, and a systolic flow murmur at the left sternal border. You request a complete blood count: Hb 6.8 g/dL, MCV 62 fL, MCH 18 pg, RDW 19%. Where do you begin? What does each number tell you, and how does knowing the MCV immediately restructure your differential diagnosis?
WHY THIS MATTERS
Anaemia affects over 1.2 billion people globally, with children under five and school-age children in low-income countries bearing the greatest burden. In India, the National Family Health Survey-5 (2019–21) reports that 67% of children aged 6–59 months are anaemic. Unrecognised or inadequately treated anaemia in childhood impairs cognitive development, physical growth, school performance, and immune function. As a clinician, you will encounter anaemic children in every setting — outpatient clinics, emergency departments, nutrition rehabilitation centres, and inpatient wards. A structured, MCV-based approach is the single most powerful tool to arrive at the correct aetiology quickly, minimise investigations, and direct treatment before complications develop.
RECALL
Before proceeding, recall the following from Biochemistry and Pathology:
• Haemoglobin structure: adult Hb (HbA) consists of two alpha (α) and two beta (β) globin chains, each carrying a haem group that binds oxygen reversibly; fetal Hb (HbF) has gamma chains instead of beta chains and has higher oxygen affinity.
• RBC indices from Pathology: MCV (mean corpuscular volume, fL) measures average RBC size; MCH (mean corpuscular haemoglobin, pg) measures average Hb per RBC; MCHC (mean corpuscular haemoglobin concentration, g/dL) measures Hb concentration per RBC volume; RDW (red cell distribution width, %) measures variation in RBC size — elevated in deficiency states.
• Iron cycle: dietary iron is absorbed in the duodenum and proximal jejunum, transported as transferrin, stored as ferritin, and incorporated into haem during erythropoiesis in the bone marrow. Hepcidin is the liver-derived master regulator — it reduces iron export from enterocytes and macrophages in inflammation.
Definition and Classification of Anaemia
Anaemia is defined as a reduction in haemoglobin concentration, haematocrit, or red cell count below the normal reference range for age, sex, and physiological state. In clinical paediatrics, haemoglobin is the most practical measure. The World Health Organization and Indian Academy of Pediatrics define anaemia using the following age-specific cut-offs: Hb <11 g/dL in children under 5 years; Hb <11.5 g/dL in children aged 5–11 years; Hb <12 g/dL in adolescent girls (12–14 years) and non-pregnant adult women; Hb <13 g/dL in adolescent boys and adult men. These cut-offs reflect the normal physiological rise in Hb with age and the male-female divergence at puberty. In practical assessment, severity is graded as mild (Hb from the cut-off down to 10 g/dL), moderate (7–10 g/dL), and severe (<7 g/dL) — severity directly guides transfusion decisions.
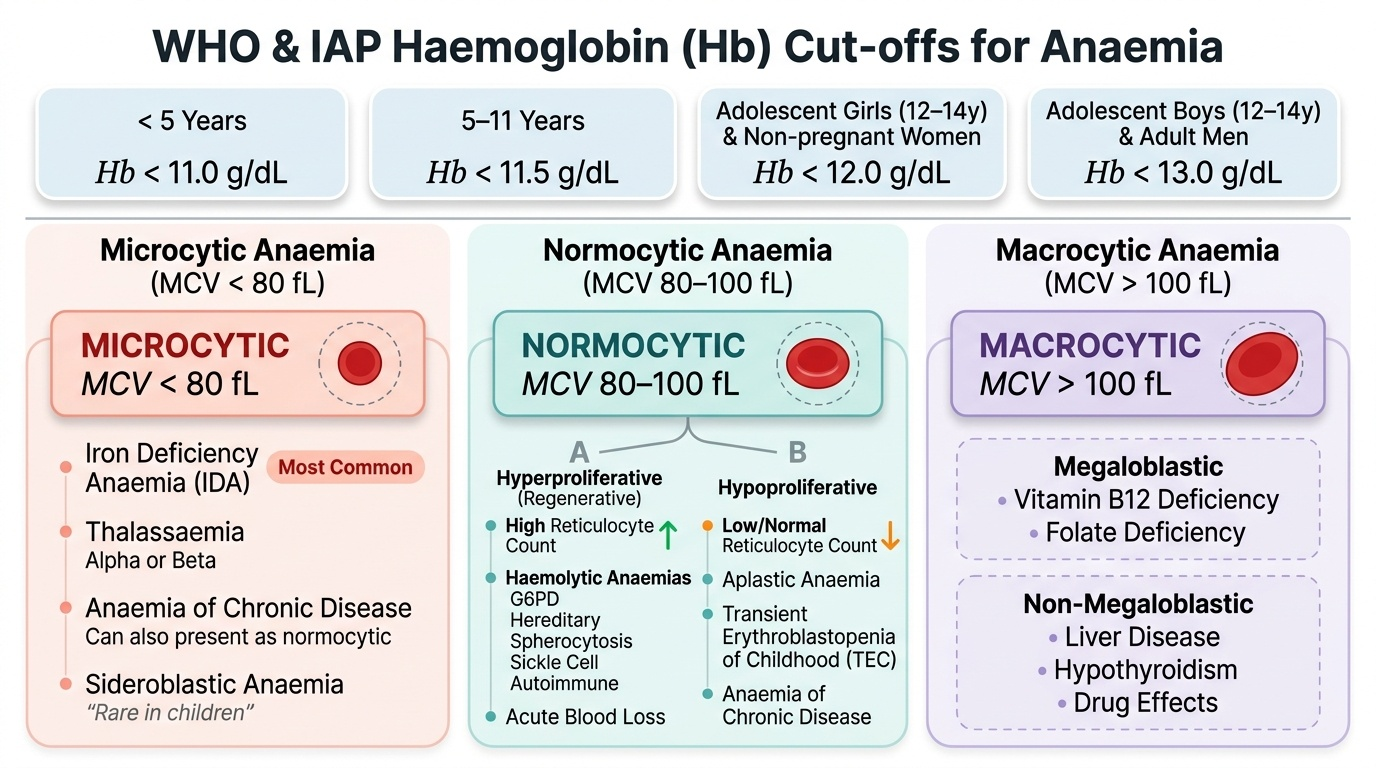
Provided image
The most useful initial classification of anaemia uses MCV (mean corpuscular volume): microcytic if MCV <80 fL, normocytic if 80–100 fL, and macrocytic if >100 fL. This immediately partitions the differential into three distinct pathological mechanisms and narrows the investigation pathway considerably. A second dimension is the reticulocyte count, which separates hyperproliferative (regenerative — blood loss, haemolysis) from hypoproliferative (bone marrow failure, nutritional deficiency) causes of normocytic anaemia.
Common causes by MCV category in paediatric practice:
• Microcytic: Iron deficiency anaemia (IDA — most common overall), thalassaemia (alpha or beta), anaemia of chronic disease (usually normocytic but can be microcytic), sideroblastic anaemia (rare in children)
• Normocytic: Haemolytic anaemias (G6PD, hereditary spherocytosis, sickle cell, autoimmune), aplastic anaemia, acute blood loss, anaemia of chronic disease, transient erythroblastopenia of childhood (TEC)
• Macrocytic: Megaloblastic anaemia due to vitamin B12 or folate deficiency; non-megaloblastic causes include liver disease, hypothyroidism, and drug effects
Pathophysiology and Aetiology
Anaemia arises from one or more of three fundamental mechanisms, and understanding them prevents diagnostic anchoring. The three mechanisms are: (1) decreased RBC production (hypoproliferative), (2) increased RBC destruction (haemolytic), and (3) blood loss (acute or chronic). In children, nutritional deficiency is the dominant cause of decreased production, while congenital haemolytic conditions predominate among causes of increased destruction.
Decreased production occurs when erythropoiesis is impaired by: nutritional deficiency (iron, B12, or folate — substrate shortage); bone marrow suppression (aplastic anaemia, infiltration by leukaemia, drugs, radiation); or chronic inflammation (anaemia of chronic disease — the hepcidin-mediated mechanism sequesters iron in macrophages and reduces EPO responsiveness). In iron deficiency, the bone marrow runs out of substrate for haem synthesis, producing small hypochromic red cells.
Increased destruction (haemolysis) can be intravascular (complement-mediated, e.g. transfusion reactions, paroxysmal nocturnal haemoglobinuria) or extravascular (splenic — hereditary spherocytosis, G6PD deficiency, sickle cell, thalassaemia major). Laboratory markers of haemolysis include elevated unconjugated bilirubin, elevated LDH, reduced haptoglobin, and reticulocytosis.
Blood loss is less common in young children but occurs with hookworm infestation, Meckel's diverticulum, and gastrointestinal bleeding; in adolescent girls, heavy menstrual flow is a significant contributor. Chronic occult blood loss (especially hookworm) produces the same CBC picture as IDA because it depletes iron stores.
Aetiologically, the predominant paediatric causes by age group are:
• Neonates: haemolytic disease of the newborn (Rh/ABO), G6PD haemolysis, physiological nadir
• Infants 6–24 months: IDA (rapid growth + inadequate dietary iron + late introduction of iron-rich foods)
• School-age children: IDA, hookworm-related blood loss, thalassaemia minor
• Adolescents: IDA (girls — menstruation; boys — growth spurt), haemolytic conditions
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
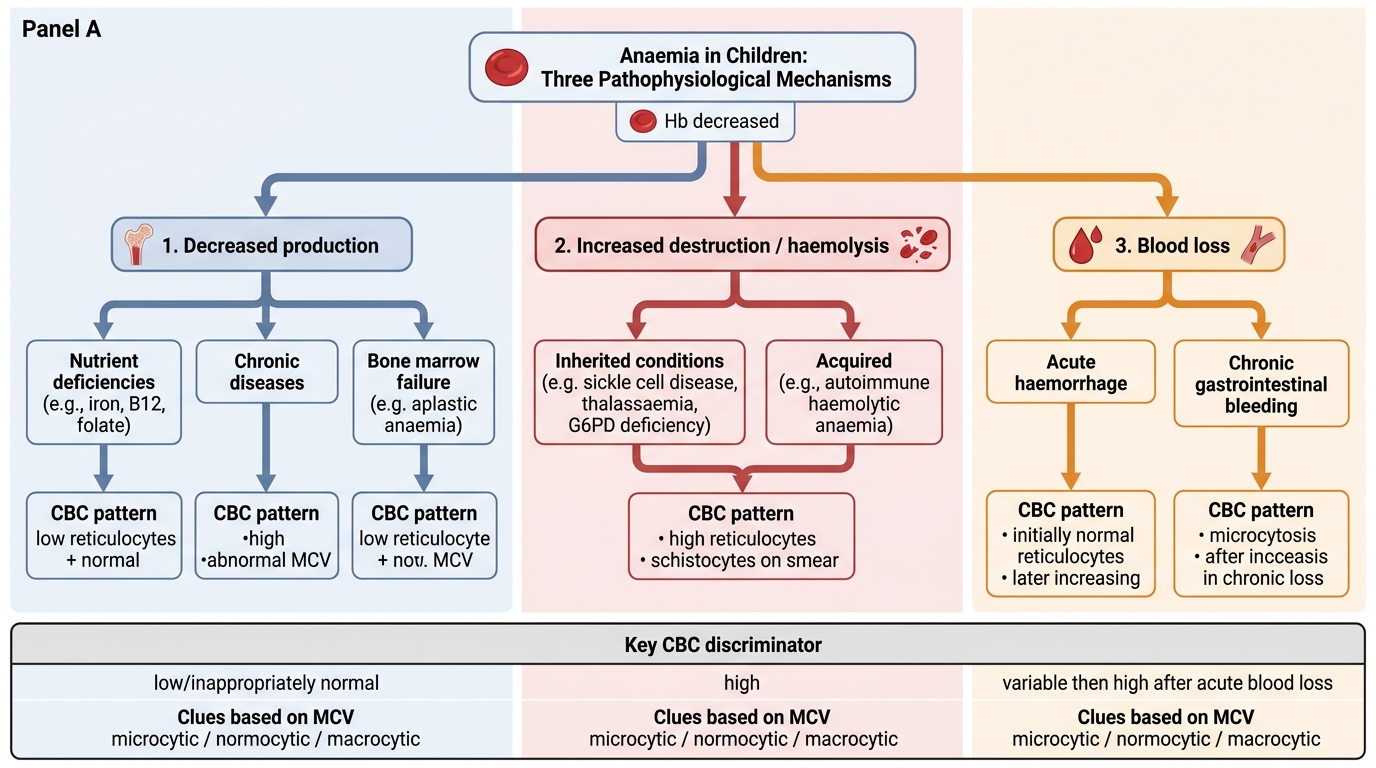
Pathophysiological Mechanisms of Anaemia in Children
Clinical Features
The clinical features of anaemia in children result from two overlapping processes: oxygen-delivery failure to tissues and the compensatory cardiovascular response to maintain tissue oxygenation. Understanding these mechanisms makes the physical signs predictable and interpretable rather than a rote list to memorise.
Symptoms reflect reduced oxygen supply to the brain and muscles: fatigue and reduced exercise tolerance, irritability and poor concentration (particularly important in school-age children as cognitive impairment), headache, and in severe or rapidly developing anaemia, dyspnoea on exertion. In infants, poor feeding and failure to thrive may be the presenting complaint. Pica — a craving to eat non-food substances such as soil, clay, or ice — is a specific though not universal feature of iron deficiency in children.
General signs include pallor, which is best assessed at the conjunctiva (the single most reliable site — a pale conjunctiva with Hb <7 g/dL has good sensitivity), palmar creases, nail beds, and buccal mucosa. Pallor of the palms is a specific sign in darker-skinned individuals. In chronic iron deficiency, additional signs include koilonychia (spoon-shaped nails), angular stomatitis, glossitis, and brittle hair.
Cardiovascular compensation produces tachycardia, a systolic flow murmur (due to turbulent flow from reduced blood viscosity and increased cardiac output), and in severe cases (Hb <5 g/dL), signs of high-output cardiac failure: cardiomegaly, elevated JVP, hepatomegaly, and in extreme cases, oedema. This is a medical emergency requiring urgent intervention.
Haemolysis-specific signs include jaundice (indirect hyperbilirubinaemia), splenomegaly (extravascular haemolysis), and in thalassaemia major, the characteristic facies — frontal bossing and maxillary prominence from expanded erythroid marrow in untransfused or under-transfused cases.
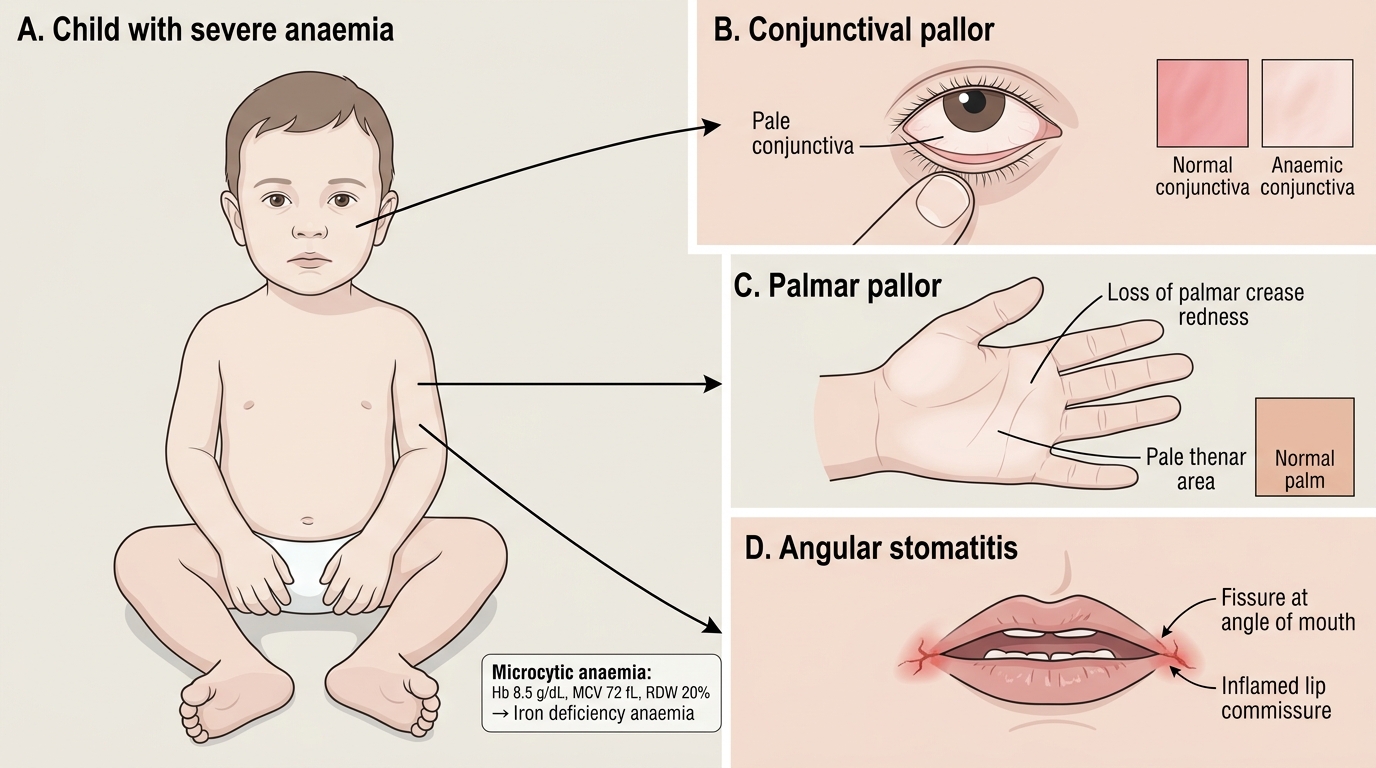
Clinical Signs of Severe Iron Deficiency Anaemia in a Child
SELF-CHECK
A 2-year-old child has Hb 8.5 g/dL, MCV 72 fL, and RDW 20%. Which of the following is the most likely diagnosis?
A. Vitamin B12 deficiency
B. Iron deficiency anaemia
C. Hereditary spherocytosis
D. Aplastic anaemia
Reveal Answer
Answer: B. Iron deficiency anaemia
MCV 72 fL is microcytic (<80 fL) and RDW 20% is elevated (normal 11.5–14.5%), pointing to marked anisocytosis — the hallmark of iron deficiency anaemia. B12 deficiency produces macrocytosis (MCV >100). Hereditary spherocytosis causes normocytic haemolytic anaemia. Aplastic anaemia results in normocytic or slightly macrocytic anaemia.