Page 2 of 34
PE26.1 | Approach to Anaemia — SDL Guide (Part 2)
Systematic Approach and Investigation Strategy
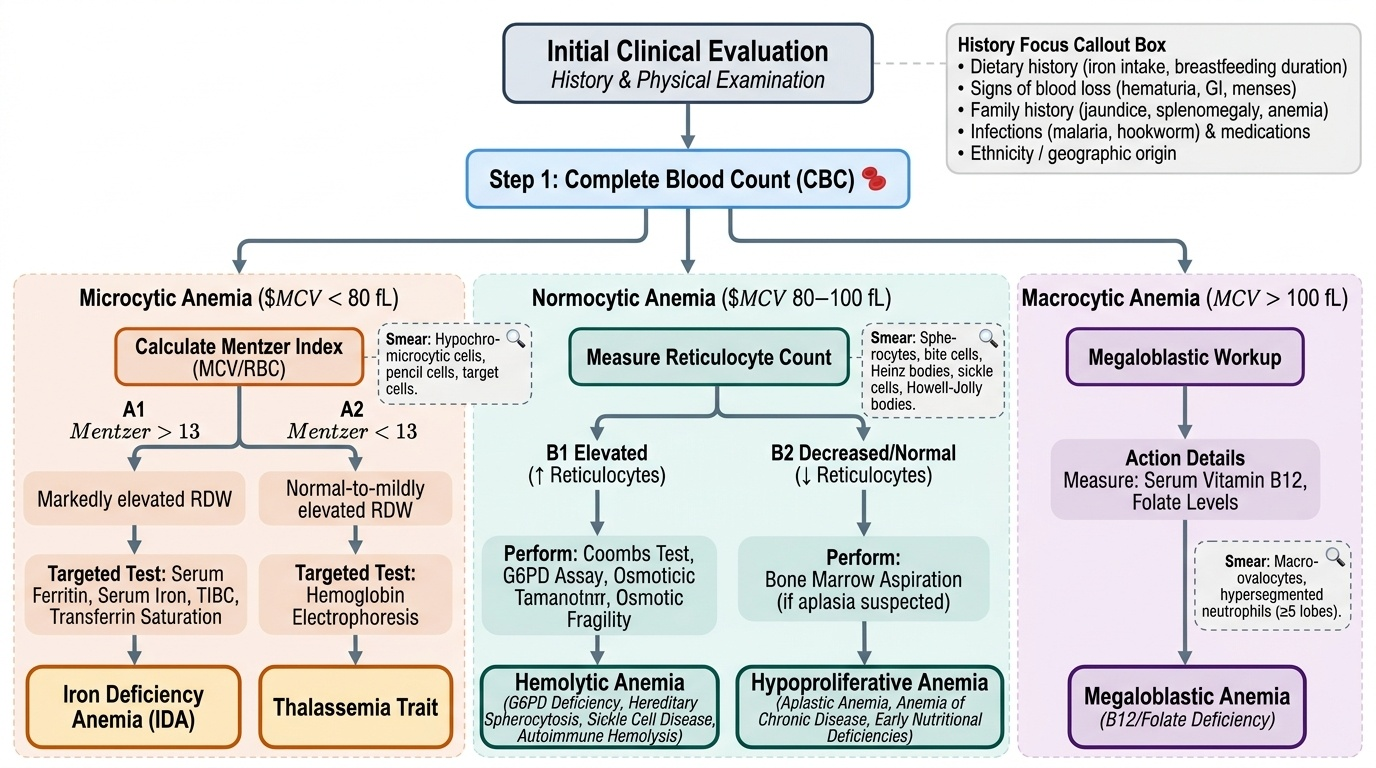
A systematic, stepwise approach to the child with anaemia prevents both under-investigation (missing a haemolytic condition) and over-investigation (ordering expensive tests before the cheap CBC is fully interpreted). The approach begins with history and examination, then uses the CBC as the primary decision tool.
Provided image
History focus: dietary history (iron-rich foods, breastfeeding duration, complementary feeding), symptoms of blood loss (haematuria, rectal bleeding, menstruation), family history of anaemia, jaundice, or splenomegaly (suggesting hereditary haemolytic conditions), history of infections (malaria in endemic areas, hookworm), medication history (drug-induced haemolysis or marrow suppression), ethnicity (thalassaemia common in Mediterranean, South-East Asian, and Indian populations).
Step 1 — CBC with indices: The MCV immediately classifies the anaemia into microcytic, normocytic, or macrocytic. The Mentzer index (MCV/RBC count) is a useful discriminator in the microcytic group: a value <13 suggests thalassaemia trait (normal or high RBC count with small cells), while >13 suggests IDA (low RBC count with small cells). The RDW reflects anisocytosis: markedly elevated in IDA (cells vary widely in size as iron runs out), normal-to-mildly elevated in thalassaemia trait.
Step 2 — Peripheral blood smear: This is the most informative single investigation after the CBC. Key findings:
• IDA: hypochromic microcytic cells, pencil cells (elliptocytes), target cells in severe disease
• Thalassaemia: target cells, nucleated RBCs, polychromasia
• Megaloblastic anaemia: macro-ovalocytes, hypersegmented neutrophils (≥5 lobes or ≥1 cell with 6 lobes)
• Hereditary spherocytosis: small dense spherocytes, absent central pallor
• G6PD deficiency (during crisis): Heinz bodies (supravital stain), bite cells
• Sickle cell: sickle-shaped cells, Howell-Jolly bodies (asplenia)
Step 3 — Targeted investigation by MCV branch:
• Microcytic: serum ferritin (most sensitive/specific for iron stores), serum iron, TIBC, transferrin saturation; haemoglobin electrophoresis if Mentzer index <13 or ferritin normal
• Normocytic: reticulocyte count separates haemolytic (↑ reticulocytes) from hypoproliferative (↓ reticulocytes); if haemolytic: Coombs test, G6PD assay, osmotic fragility; if hypoproliferative: bone marrow aspiration if aplasia suspected
• Macrocytic: serum B12, serum folate, peripheral smear for hypersegmented neutrophils; bone marrow if non-megaloblastic
| Index | IDA | Thalassaemia Trait | Megaloblastic |
|---|---|---|---|
| MCV | ↓↓ | ↓ | ↑↑ |
| RDW | ↑↑ | Normal or mildly ↑ | ↑ |
| Mentzer index | >13 | <13 | N/A |
| Ferritin | ↓↓ | Normal | Normal |
| Smear | Hypochromic, pencil cells | Target cells, microcytes | Macro-ovalocytes, hyperseg. neutrophils |
CLINICAL PEARL
The Mentzer index (MCV ÷ RBC count) is a quick bedside calculation: if MCV = 68 fL and RBC = 6.2 × 10¹²/L, Mentzer = 68 ÷ 6.2 = 10.97 (<13) — thalassaemia trait more likely. If MCV = 65 and RBC = 3.8 × 10¹²/L, Mentzer = 65 ÷ 3.8 = 17.1 (>13) — IDA more likely. It is a screening tool, not a diagnostic test, but it saves time and money before ordering haemoglobin electrophoresis.
Approach by Diagnosis and Management Principles
Once the aetiology is identified or strongly suspected, management is directed at the underlying cause while simultaneously addressing the degree of anaemia and any complications. A general framework applies to all types regardless of aetiology, with condition-specific management details covered in subsequent SDLs on IDA, B12/folate deficiency, and haemolytic anaemias. The guiding principle in paediatric anaemia management is that transfusion is a bridge, not a cure: it corrects the haemoglobin temporarily but does nothing about the underlying cause, which will reproduce the anaemia unless directly treated. Simply transfusing a child with IDA without prescribing iron and addressing dietary deficiency leads to recurrence within weeks. Similarly, transfusing a child with thalassaemia major without initiating chelation leads to progressive iron overload affecting the heart and liver. Cause-directed treatment, concurrent attention to nutritional status, treatment of co-morbid infections, and careful monitoring of haematological response are the four pillars of effective management.
General principles for all anaemias:
1. Treat the underlying cause (iron supplementation for IDA, B12/folate replacement for megaloblastic, transfusion and chelation for thalassaemia major, management of haemolysis triggers for G6PD).
2. Correct dietary deficiencies and counsel caregivers on iron-rich foods (especially for IDA).
3. Treat concurrent infections (malaria, hookworm) which perpetuate anaemia.
4. Monitor response: reticulocyte response within 7–10 days of starting haematinics indicates adequate treatment; haemoglobin should rise ~1–2 g/dL per week with effective iron therapy.
Packed red cell transfusion (PRCT) indications in children:
• Hb <7 g/dL with haemodynamic compromise or active bleeding
• Hb <7 g/dL with signs of cardiac failure, severe tachycardia, or respiratory distress
• Symptomatic anaemia despite haemoglobin in the 7–10 range (clinical judgement)
• Pre-operative correction when surgery is urgently needed
• Transfusion is NOT routinely indicated for compensated anaemia with Hb ≥7 g/dL in a nutritional deficiency; the clinical and haematological response to specific treatment should be awaited
Dose of PRCT: 10–15 mL/kg, administered over 3–4 hours; for severe anaemia with cardiac failure, give 5 mL/kg slowly with a concurrent diuretic to prevent fluid overload.
When to refer to a paediatric haematologist:
• Suspected thalassaemia major or sickle cell disease
• Non-response to iron therapy after 4 weeks
• Features suggesting aplastic anaemia or haematological malignancy
• Recurrent haemolytic episodes
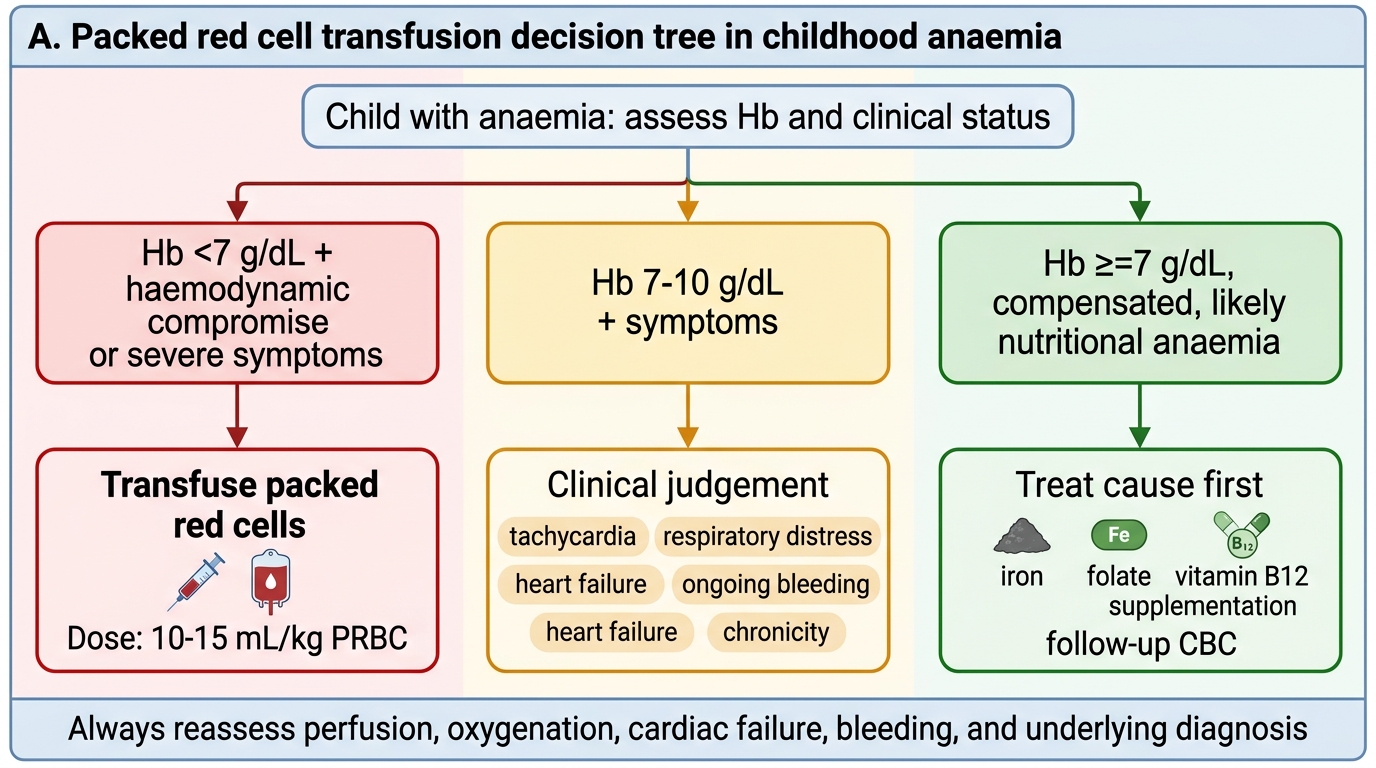
Packed Red Cell Transfusion Decision Tree in Childhood Anaemia
SELF-CHECK
A 5-year-old boy has Hb 9.2 g/dL, MCV 85 fL, reticulocyte count 8% (elevated), and indirect bilirubin 3.1 mg/dL. What is the most appropriate next investigation?
A. Serum ferritin
B. Serum B12 level
C. Direct Coombs test
D. Bone marrow aspiration
Reveal Answer
Answer: C. Direct Coombs test
The picture is normocytic anaemia with elevated reticulocyte count and indirect hyperbilirubinaemia — a classic haemolytic pattern. The appropriate next investigation is the Direct Coombs test (direct antiglobulin test) to determine whether haemolysis is immune-mediated (autoimmune haemolytic anaemia, alloantibodies) or not. Serum ferritin is for iron deficiency (microcytic). Serum B12 is for macrocytic anaemia. Bone marrow aspiration is indicated in hypoproliferative (low reticulocyte) normocytic anaemia.
Self-Assessment
Self-assessment consolidates the MCV-based diagnostic framework you have built throughout this module. Rather than reciting facts in isolation, the goal is to apply them in an integrated clinical scenario — the same cognitive operation you will perform at the bedside. Work through the case below independently, calculating indices and choosing investigations before reading the analysis. This kind of deliberate retrieval practice strengthens diagnostic reasoning far more effectively than re-reading alone, and exposes any gaps in your understanding of the Mentzer index, RDW interpretation, and transfusion thresholds before you encounter these decisions in a clinical context.
Case: A 3-year-old girl is brought with pallor for 2 months. She is predominantly breastfed and has had minimal complementary feeding. CBC shows Hb 7.5 g/dL, MCV 62 fL, MCH 16 pg, RDW 18.5%, RBC count 5.8 × 10¹²/L. Peripheral smear shows hypochromic microcytic cells with occasional target cells.
Questions:
1. Calculate the Mentzer index and interpret it.
2. Does the RDW and smear support IDA or thalassaemia trait?
3. What single investigation would best confirm your diagnosis?
4. What is your immediate management, and what dietary counselling would you provide?
Analysis:
1. Mentzer index = 62 ÷ 5.8 = 10.7 — this is <13, suggesting thalassaemia trait; however, the clinical context (poor diet, late complementary feeding) strongly suggests IDA.
2. RDW 18.5% is markedly elevated, which favours IDA (anisocytosis); in thalassaemia trait, RDW is typically normal or only mildly elevated. The smear shows hypochromic microcytic cells; target cells appear in both conditions.
3. Serum ferritin is the investigation of choice. A low ferritin (<12 µg/L) confirms IDA. If ferritin is normal, haemoglobin electrophoresis would be ordered to exclude thalassaemia trait.
4. Prescribe elemental iron 3–6 mg/kg/day (ferrous sulphate or ferrous gluconate) for at least 3 months (1 month to correct Hb + 2 months to replenish stores). Dietary counselling: iron-rich foods (meat, fish, poultry, dark leafy vegetables, legumes), vitamin C (enhances absorption), limit cow's milk (inhibits iron absorption). Introduce iron-fortified complementary feeds. Expected response: reticulocytosis within 7–10 days; Hb rise ~1 g/dL/week.
This case illustrates that the Mentzer index is a screening tool — the full picture (RDW, clinical history, ferritin) drives the diagnosis.
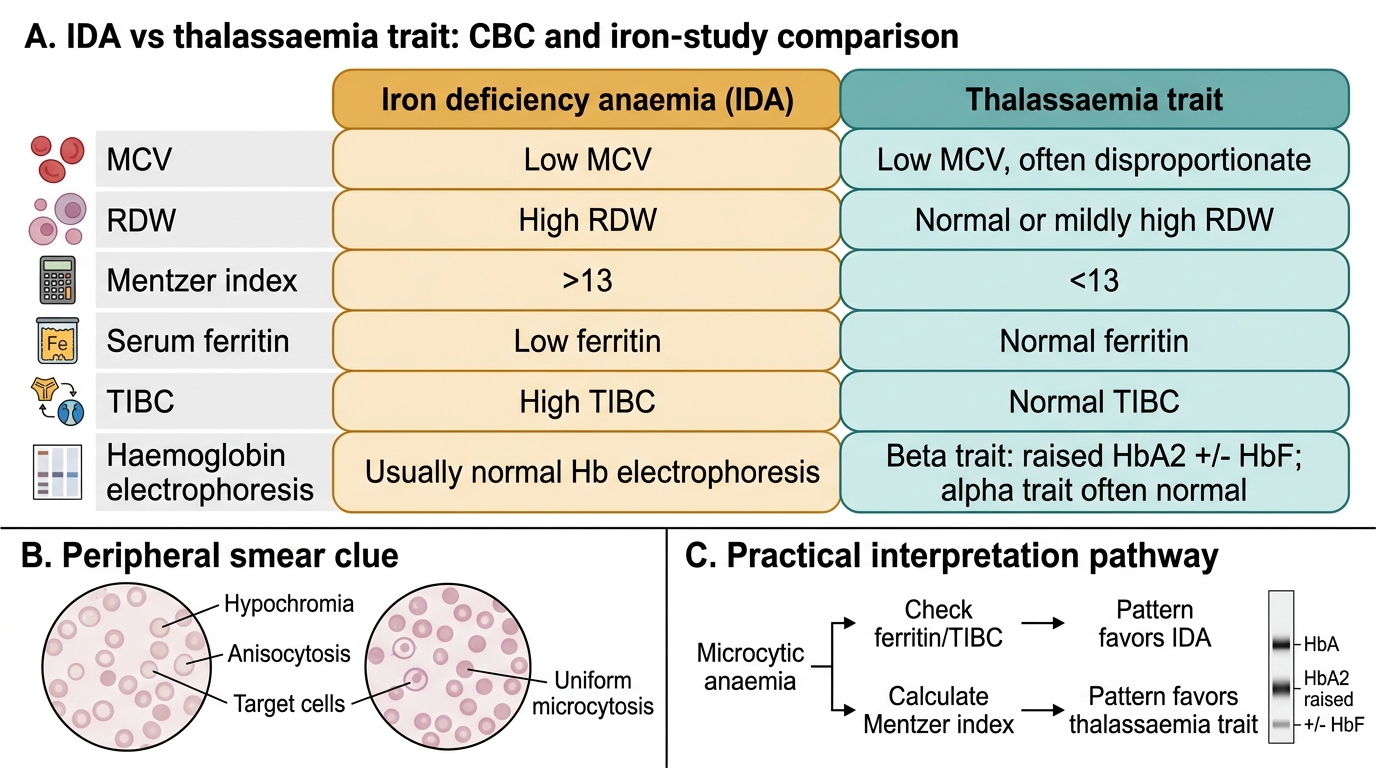
IDA vs Thalassaemia Trait: Key Laboratory Differences