Page 17 of 34
PE26.7 | Hemophilia — SDL Guide (Part 2)
Management of Hemophilia
Management of hemophilia is centred on factor replacement therapy — supplying the missing coagulation factor to restore haemostatic function. The approach has evolved from purely on-demand (reactive) treatment to prophylactic (preventive) infusions in severe hemophilia, which is now the global standard of care because it prevents haemarthrosis and preserves joint function over decades.
Provided image
Dosing of factor replacement — the most examinable calculation:
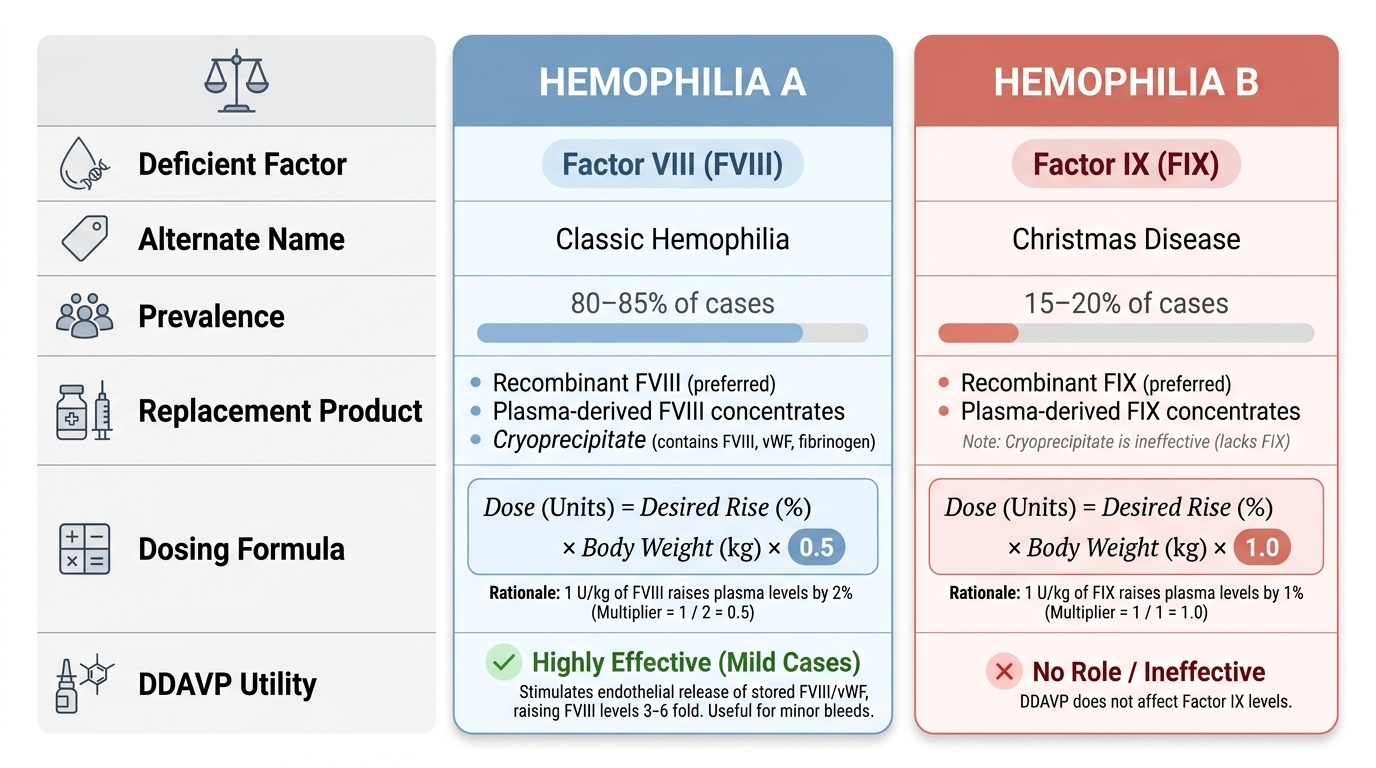
For Hemophilia A (factor VIII):
> Factor VIII dose (units) = Desired rise in factor level (%) × Body weight (kg) × 0.5
Rationale: infusing 1 unit/kg of factor VIII raises the plasma level by approximately 2%, so the multiplier is 1/2 = 0.5.
For Hemophilia B (factor IX):
> Factor IX dose (units) = Desired rise in factor level (%) × Body weight (kg) × 1.0
Rationale: infusing 1 unit/kg of factor IX raises the plasma level by approximately 1% (a smaller volume-of-distribution correction for FIX), so the multiplier is 1.
Example: A 40 kg boy with hemophilia A has a haemarthrosis and baseline factor VIII of 2%. The target level for joint bleed is 50%. Dose = (50 − 2) × 40 × 0.5 = 48 × 40 × 0.5 = 960 units given as an IV infusion.
Indications and target levels: Minor bleeds (haemarthrosis, muscle haematoma) → target 30–50%; major bleeds (surgery, iliopsoas, head injury, life-threatening) → target 80–100%; prophylaxis in severe hemophilia → maintain trough >1% (usually achieved by thrice-weekly or alternate-day infusions).
Products available:
• Plasma-derived factor concentrates (virus-inactivated) — available in Indian haemophilia treatment centres.
• Recombinant factor concentrates (rFVIII, rFIX) — preferred in resource-adequate settings (no viral transmission risk).
• Cryoprecipitate — contains factor VIII, fibrinogen, von Willebrand factor; used when concentrates are unavailable.
• Fresh Frozen Plasma (FFP) — contains all coagulation factors but in low concentrations; volume-limited; inferior to concentrates for specific factor deficiency.
DDAVP (Desmopressin, 1-deamino-8-D-arginine vasopressin): Stimulates endothelial release of stored vWF and factor VIII, raising FVIII levels 3–6-fold within 30–60 minutes. Useful only in mild hemophilia A (patients with baseline FVIII 5–40%) for minor bleeds or pre-procedural cover — it has no role in hemophilia B (which involves FIX, not FVIII).
Adjuncts and general principles:
• Tranexamic acid (antifibrinolytic) — useful for oral mucosal bleeds, epistaxis, and dental procedures.
• Haemarthrosis management (RICE): Rest, Ice pack (cold compression), Compression bandage, Elevation of the affected limb — plus factor replacement.
• Physiotherapy between episodes: regular supervised exercise preserves joint strength and prevents contractures.
• Avoid aspirin and all NSAIDs — these impair platelet function and compound the haemostatic defect.
• Inhibitor management: Patients who develop inhibitors require either high-dose factor to overwhelm the antibody, bypassing agents (activated prothrombin complex concentrate, recombinant factor VIIa), or immune tolerance induction.
• Genetic counselling: All carrier females and their families should receive structured counselling regarding inheritance, carrier testing, and prenatal diagnosis options.
SELF-CHECK
A 40 kg boy with severe hemophilia A (baseline factor VIII <1%) presents with a knee haemarthrosis. You decide to raise his factor VIII level to 50%. How many units of factor VIII concentrate should you administer?
A. 500 units
B. 1000 units
C. 1500 units
D. 2000 units
Reveal Answer
Answer: B. 1000 units
Using the formula: Factor VIII dose = desired rise (%) × weight (kg) × 0.5. Desired rise = 50 − 0 (baseline ~0%) = 50%. Dose = 50 × 40 × 0.5 = 1000 units. The 0.5 multiplier reflects the pharmacokinetic fact that 1 unit/kg of factor VIII raises plasma FVIII by approximately 2 IU/dL (2%). The factor IX formula uses a multiplier of 1.0 (1 unit/kg raises FIX by ~1%).
Self-Assessment
Consolidate your understanding with the following case and questions.
Case: A 10-year-old boy presents with right knee swelling and pain for three days following a minor fall. He reports that his maternal uncle had a 'bleeding disorder' requiring factor infusions. Examination: warm, swollen right knee with limited flexion; no petechiae or purpura; no lymphadenopathy; no hepatosplenomegaly. Investigations: Hb 10.8 g/dL (mild anaemia, likely from bleeding), WBC 9,200/µL (normal), platelets 280,000/µL, PT 13 s (normal), aPTT 82 s (reference <35 s), bleeding time normal. Factor VIII activity: 2%.
Q1: What is the diagnosis?
Answer: Hemophilia A — factor VIII deficiency confirmed at 2% (moderate-to-severe), X-linked recessive, with haemarthrosis of the knee.
Q2: Calculate the factor VIII dose to raise the level to 50% in this 35 kg boy.
Answer: Dose = (50 − 2) × 35 × 0.5 = 48 × 35 × 0.5 = 840 units IV.
Q3: The junior resident wants to give him paracetamol IM for the pain. What is your response?
Answer: Strictly contraindicated — IM injections must never be given in hemophilia. Prescribe oral/IV paracetamol only. Aspirin and NSAIDs must also be avoided.
Q4: What additional investigation would you order to look for a complication of repeated factor replacement?
Answer: Factor VIII inhibitor assay (Bethesda assay) — repeated FVIII infusions lead to inhibitor development in ~25–30% of severe hemophilia A patients. This should be checked if the aPTT fails to correct with factor replacement or if the mixing test shows non-correction.
SELF-CHECK
DDAVP (desmopressin) is effective for raising factor levels in which specific clinical scenario?
A. Severe hemophilia A (baseline FVIII <1%) with haemarthrosis
B. Mild hemophilia A (baseline FVIII 5–40%) for minor bleeds or pre-procedural cover
C. Hemophilia B (factor IX deficiency) for any severity
D. Hemophilia A with inhibitors
Reveal Answer
Answer: B. Mild hemophilia A (baseline FVIII 5–40%) for minor bleeds or pre-procedural cover
DDAVP stimulates endothelial release of stored von Willebrand factor (vWF) and factor VIII, raising plasma FVIII levels 3–6-fold. This works only if the patient has some endogenous FVIII to release — hence it is useful only in MILD hemophilia A (baseline FVIII 5–40%) for minor bleeds or pre-procedural prophylaxis. In severe hemophilia A (baseline <1%), there is no stored FVIII to release, so DDAVP is ineffective. DDAVP does NOT affect FIX levels and is ineffective in hemophilia B.