Page 1 of 48
PE27.1 | Acute Bacterial Meningitis — SDL Guide
Learning Objectives
- Explain the age-specific aetiology of acute bacterial meningitis in neonates, infants, and older children
- Describe the pathophysiology of bacterial invasion of the meninges and resultant inflammation
- Interpret CSF findings to distinguish bacterial meningitis from other causes
- Outline the empirical antibiotic regimen, adjunctive dexamethasone, and supportive care
- Identify early and late complications and describe preventive strategies including vaccination
INSTRUCTIONS
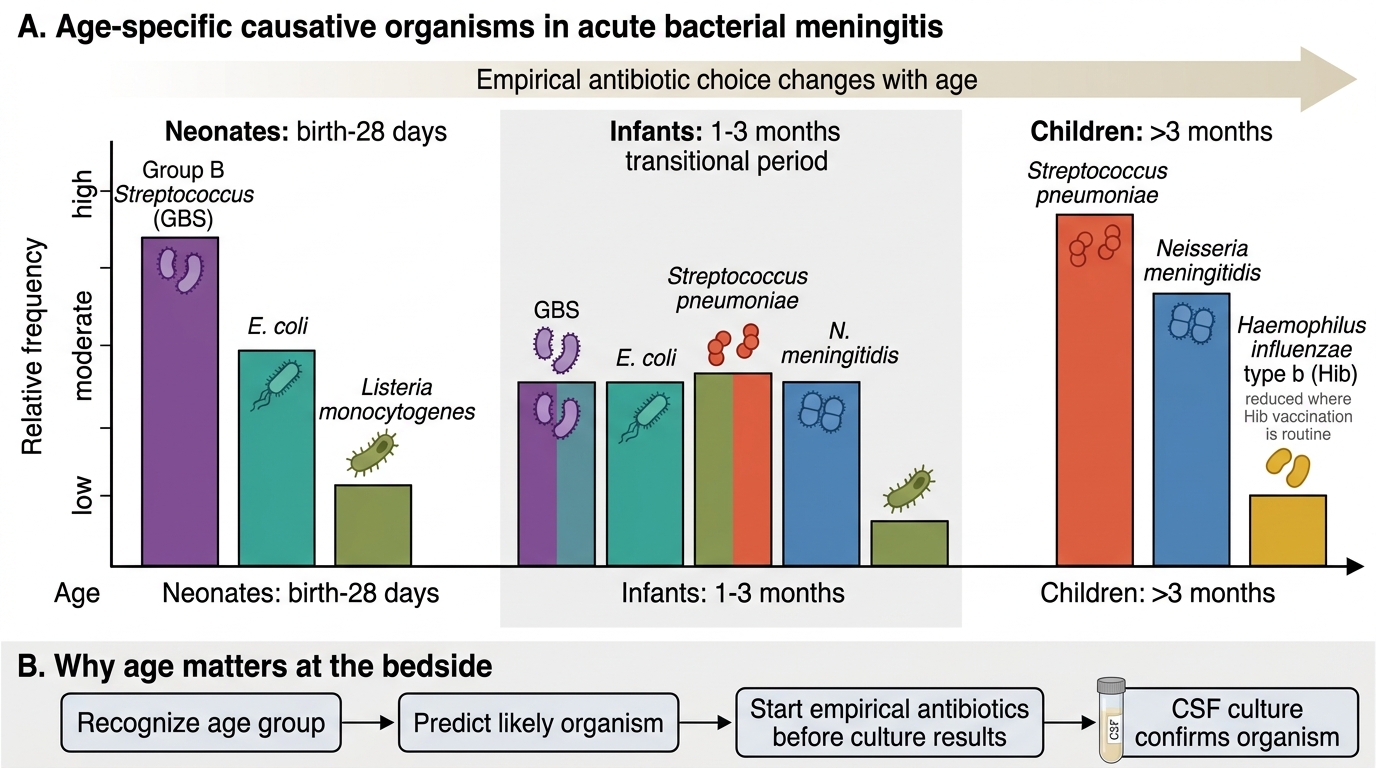
Bacterial meningitis is a paediatric emergency carrying a mortality rate of 5–30% even with treatment, and leaving neurological sequelae in up to 30% of survivors. The causative organism shifts predictably with age, a fact that directly determines your empirical antibiotic choice before culture results are available. This module builds your systematic approach: recognise the age-appropriate organism, understand the inflammatory cascade that drives pathology, interpret the lumbar puncture correctly, and institute life-saving treatment within the critical early window.
References
- Ghai Essential Pediatrics, 9th ed., Ch 17 (CNS Infections) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 616 (Bacterial Meningitis beyond the Neonatal Period) (textbook)
- IAP Guidelines on Management of Acute Bacterial Meningitis (current edition) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-month-old boy is brought to the emergency department with a 2-day history of high fever, irritability, and poor feeding. On examination he is febrile at 39.5°C, has a tense, bulging anterior fontanelle, and neck stiffness. He had received his 6-week and 10-week vaccines but his parents moved states and the 14-week dose was missed. A lumbar puncture is performed immediately. The CSF is turbid, with WBC 1,800/mm³ (90% neutrophils), protein 180 mg/dL, and glucose 18 mg/dL (simultaneous serum glucose 95 mg/dL). What organism is most likely, and what treatment must be started right now — before culture results return?
WHY THIS MATTERS
Acute bacterial meningitis is one of the true paediatric emergencies where a delay of even a few hours in diagnosis or treatment measurably worsens outcome. India continues to carry a high burden of meningitis, particularly from Haemophilus influenzae type b (Hib) in unimmunised children and Streptococcus pneumoniae year-round. As a final-year student and future intern, you will be among the first to assess a child presenting with fever and altered behaviour; your ability to suspect meningitis, perform or request a lumbar puncture safely, and initiate empirical treatment while awaiting results is genuinely life-saving knowledge. Understanding the age-stratified organism spectrum is not rote memorisation — it is the rational basis for the antibiotic choice you must make before microbiology is available.
RECALL
Before proceeding, recall the following from earlier modules:
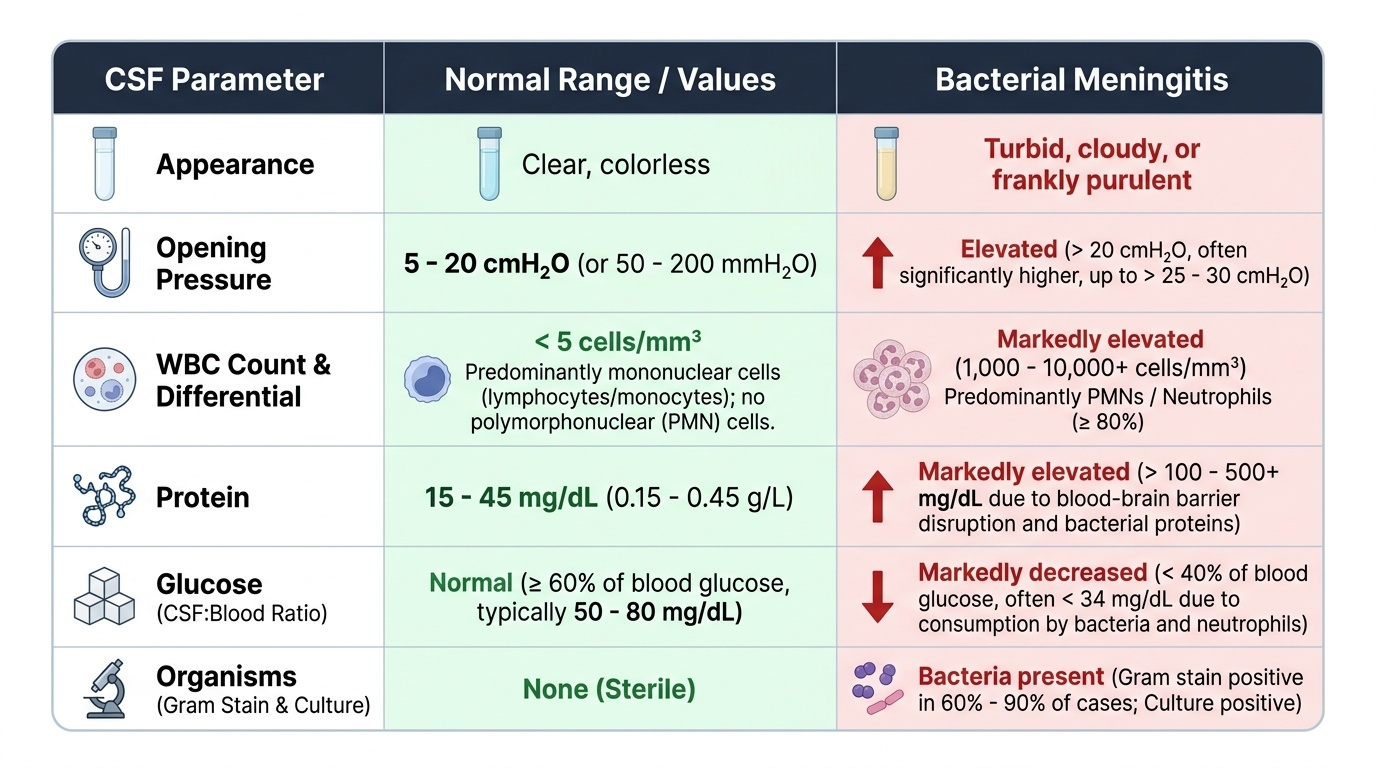
• Cerebrospinal fluid (from PY): produced by the choroid plexus at ~0.35 mL/min; circulates in the subarachnoid space; normal composition in older children — clear, colourless, WBC <5/mm³ (lymphocytes), protein 15–45 mg/dL, glucose 50–80 mg/dL (or 60–70% of simultaneous serum glucose).
• Blood-brain barrier (from AN/PY): tight junctions of cerebral capillary endothelium restrict most molecules; bacterial toxins and cytokines disrupt this barrier, allowing oedema.
• Gram stain morphology (from MI): Group B Streptococcus = gram-positive cocci in chains; E. coli = gram-negative rods; N. meningitidis = gram-negative diplococci (intracellular); S. pneumoniae = gram-positive diplococci (lancet-shaped).
• Complement system: the alternative pathway is critical for opsonisation of encapsulated bacteria; neonates and asplenic patients lack this protection, explaining increased susceptibility.
Clinical Presentation of Acute Bacterial Meningitis
The clinical presentation of bacterial meningitis varies dramatically with age, making age the single most important variable in your initial assessment. Neonates (0–28 days) rarely present with the classic meningeal signs seen in older children; instead, the signs are non-specific and easy to overlook: poor feeding and lethargy, temperature instability (may be hypothermic, not necessarily febrile), high-pitched cry, a bulging anterior fontanelle, seizures, and apnoea. The absence of neck stiffness in a neonate does NOT exclude meningitis — the fontanelle is the most reliable clinical window in this age group.
Infants and older children (beyond 3 months) progressively develop more classic features as the meninges are better developed. The classic triad — fever, neck stiffness, and altered consciousness — is present in only about 44% of children with bacterial meningitis at presentation; absence of all three makes the diagnosis less likely but does not exclude it. Photophobia and headache are present in verbal children. Kernig's sign (inability to extend the knee with the hip flexed at 90°) and Brudzinski's sign (involuntary flexion of the knees when the neck is passively flexed) reflect meningeal irritation; both have moderate sensitivity.
Meningococcal disease may present with a distinctive petechial or purpuric rash, which in the context of fever and unwell appearance must be treated as meningococcaemia until proven otherwise — do not wait for lumbar puncture results. The rash does not blanch on pressure (non-blanching), distinguishing it from viral exanthems.
Raised intracranial pressure (ICP) signs — bradycardia, hypertension, and irregular respirations (Cushing's triad) — indicate herniation risk; if present, defer LP and obtain urgent CT.
Key warning signs by age:
• Neonate: bulging fontanelle, high-pitched cry, apnoea, hypothermia
• 3–18 months: bulging fontanelle, seizures, irritability, fever
• >18 months: headache, photophobia, neck stiffness, Kernig's/Brudzinski's signs
IMPORTANT: a febrile convulsion with rapid recovery is NOT bacterial meningitis; however, any child with a prolonged or focal seizure, post-ictal altered consciousness, or meningeal signs requires LP.
Age-Specific Causes of Acute Bacterial Meningitis
Pathophysiology and Aetiology by Age Group
The age-stratified organism spectrum of bacterial meningitis is not arbitrary — it reflects the interaction between the child's immunological maturity, the organisms colonising the maternal genital tract, and the bacteria circulating in the community at each developmental stage. A neonate's immune system is profoundly different from that of a 5-year-old: neonates lack maternal IgM (which does not cross the placenta), have immature complement activation, and rely heavily on transplacental IgG — a defence that is effective only against organisms the mother has encountered. This is why neonates are uniquely susceptible to organisms acquired during delivery from maternal genital colonisation. By contrast, children beyond 3 months are most vulnerable to encapsulated community-acquired pathogens against which their still-maturing adaptive immunity provides incomplete protection before vaccination. Understanding the mechanism of invasion explains why treatment must simultaneously target the organism, the host inflammatory response, and the haemodynamic consequences.
Organism spectrum by age:
Neonates (0–28 days): These three organisms dominate because they are acquired during delivery from maternal colonisation or are environmental gram-negatives.
• Group B Streptococcus (GBS, Streptococcus agalactiae) — most common cause of neonatal meningitis; acquired from maternal vaginal flora; early-onset (0–7 days) from intrapartum transmission; late-onset (7–90 days) from horizontal spread.
• Escherichia coli (K1 strain) — second most common neonatal pathogen; K1 capsular polysaccharide impairs complement-mediated killing.
• Listeria monocytogenes — less common but important; acquired through contaminated food; affects neonates AND immunocompromised/pregnant adults; gram-positive bacillus uniquely resistant to cephalosporins — this mandates adding ampicillin to the neonatal regimen.
Children >3 months:
• Streptococcus pneumoniae (pneumococcus) — most common cause of bacterial meningitis in India in children beyond 3 months of age; serotype 6B, 14, 19F common pre-vaccine; carries the highest risk of serious neurological sequelae.
• Neisseria meningitidis (meningococcus) — serogroups A, B, C, W135, Y; causes outbreaks; associated with petechial/purpuric rash and septicaemia; has a characteristic Waterhouse-Friderichsen syndrome (bilateral adrenal haemorrhage in fulminant disease).
• Haemophilus influenzae type b (Hib) — dramatically reduced in countries with high Hib vaccine coverage; still significant in unimmunised children.
Pathogenesis — how bacteria enter and damage the CNS:
Bacteria first colonise the nasopharynx, then invade the bloodstream (bacteraemia). Encapsulated organisms resist complement-mediated killing and reach the choroid plexus, where they cross into the subarachnoid space. Once in the CSF, the near-absent local immune defences (low immunoglobulin, complement) allow rapid bacterial multiplication. Bacterial cell-wall products (lipopolysaccharide, lipoteichoic acid) trigger the release of cytokines (TNF-α, IL-1β, IL-6) by microglia and arachnoid cells, producing a massive inflammatory cascade:
• Breakdown of the blood-brain barrier → vasogenic oedema
• Loss of cerebrovascular autoregulation → ischaemia
• Obstruction of CSF flow → hydrocephalus
• Direct cortical toxicity and vasculitis → neuronal death
• Exudate in cochlear aqueduct → sensorineural hearing loss (especially with pneumococcal meningitis)
SELF-CHECK
A neonate presents at day 5 of life with temperature instability, poor feeding, and a bulging anterior fontanelle. CSF grows a gram-positive coccus in chains. The organism is most likely:
A. Streptococcus pneumoniae
B. Group B Streptococcus (GBS)
C. Neisseria meningitidis
D. Haemophilus influenzae type b
Reveal Answer
Answer: B. Group B Streptococcus (GBS)
GBS (Group B Streptococcus, S. agalactiae) is the most common cause of neonatal meningitis in the first month of life, acquired from maternal genital colonisation. It appears as gram-positive cocci in chains. S. pneumoniae is the leading organism in children beyond 3 months. N. meningitidis is gram-negative. Hib rarely causes neonatal meningitis.
Diagnosis and CSF Interpretation
Lumbar puncture (LP) is the cornerstone diagnostic procedure for suspected meningitis and must not be unduly delayed, because every hour of diagnostic uncertainty prolongs the window before targeted therapy can begin. However, LP carries a real risk of precipitating cerebral herniation when intracranial pressure is already elevated; performing LP in that setting can cause fatal brainstem compression. You must therefore always make a clinical assessment for raised ICP before proceeding. The relevant contraindications are: papilloedema on fundoscopy, focal neurological deficit (suggesting a space-occupying process), reduced or rapidly declining level of consciousness (GCS <13), seizures within the preceding hour, or clinical Cushing's triad (bradycardia, hypertension, irregular respirations). If any of these are present, obtain a CT scan first and simultaneously give empirical antibiotics without waiting — delaying antibiotics for CT is a preventable cause of death. When none of these features is present, LP may be performed immediately without prior imaging. Always record the opening pressure at the time of LP using a manometer, as this is part of the diagnostic information.
Provided image
CSF analysis in bacterial meningitis:
The key parameters and their interpretation are best remembered as a coordinated picture rather than isolated numbers:
• Appearance: typically turbid or frankly purulent (cf. clear in viral; xanthochromic in subarachnoid haemorrhage)
• Opening pressure: elevated (>20 cmH₂O)
• Cell count: markedly elevated, typically 1,000–10,000 cells/mm³, predominantly neutrophils (polymorphonuclear leucocytes >80% of cells) — this neutrophilic pleocytosis is the hallmark of bacterial meningitis
• Protein: elevated, usually >100 mg/dL (normal <45 mg/dL), due to BBB breakdown and cellular debris
• Glucose: reduced — the gold standard expression is CSF glucose <40% of simultaneous serum glucose (CSF:serum ratio <0.4); if serum glucose is not measured simultaneously, a CSF glucose <40 mg/dL is a reasonable threshold. Bacteria and leucocytes consume glucose, driving it to very low levels in established bacterial meningitis.
• Gram stain: positive in 60–80% of untreated cases; sends the broadest information fastest — identifies gram-positive vs gram-negative and guides antibiotic narrowing.
• Culture: definitive, but takes 24–48 hours; sensitivity ~80–85% before antibiotics; reduced after antibiotic administration — always draw blood cultures before the first antibiotic dose (they remain positive longer than CSF cultures after antibiotic initiation).
Additional investigations:
• Serum CRP (markedly elevated in bacterial, usually normal in viral meningitis)
• Serum procalcitonin — useful discriminator (>0.5 ng/mL suggests bacterial aetiology)
• Full blood count (leucocytosis with neutrophilia)
• Serum electrolytes (detect SIADH — hyponatraemia)
• Blood glucose (for CSF:serum ratio)