Page 2 of 48
PE27.1 | Acute Bacterial Meningitis — SDL Guide (Part 2)
Complications of Bacterial Meningitis
Bacterial meningitis exerts its damage through two overlapping mechanisms: the direct toxic effects of bacterial products and the self-amplifying inflammatory response the host mounts in reply. Both mechanisms continue to cause harm even after antibiotics have sterilised the CSF, which is why early recognition and active management of complications are inseparable from antibiotic therapy. Approximately 5–30% of children with bacterial meningitis die despite optimal treatment, and up to 30% of survivors are left with one or more permanent neurological sequelae. These are not random outcomes — most complications follow predictable pathophysiological pathways from the core processes of raised intracranial pressure, disrupted vascular autoregulation, and direct cochlear and cortical injury. Knowing the mechanism of each complication tells you both when to look for it and how to intervene before it becomes irreversible.
Acute complications:
- Raised intracranial pressure (ICP): The most immediately life-threatening complication. Brain oedema, obstructive hydrocephalus, and loss of vascular autoregulation all raise ICP. Signs include declining level of consciousness, Cushing's triad (bradycardia, hypertension, irregular breathing), and papilloedema. Management: elevate head 30°, restrict fluids to two-thirds maintenance if SIADH is present, consider mannitol or hypertonic saline, avoid hypotension.
- Syndrome of inappropriate antidiuretic hormone secretion (SIADH): Inflammatory mediators stimulate ADH release, causing water retention, hyponatraemia, and worsening cerebral oedema. Presents as falling serum sodium with concentrated urine despite hypo-osmolar plasma. Fluid restriction (two-thirds maintenance) is the cornerstone; avoid hypotonic fluids.
- Subdural effusion/empyema: Collections in the subdural space, more common with H. influenzae and pneumococcal meningitis. Suspect if fever persists beyond 72 hours or if there are focal neurological signs. Diagnosed on CT. Empyema requires drainage; sterile effusions often resolve with continued antibiotic therapy.
- Brain herniation: Transtentorial or tonsillar herniation from uncontrolled ICP. Prevents LP; requires aggressive ICP management.
- Septicaemia and shock: Particularly with meningococcaemia; manage as septic shock with fluid resuscitation and vasopressors.
- Seizures: Occur in up to 30% during the acute illness; treat with benzodiazepines acutely; control is important as seizure activity worsens cerebral oxygen demand.
Long-term sequelae (occur in up to 30% of survivors):
- Sensorineural hearing loss (SNHL): Most common neurological sequela (~20% after pneumococcal, ~5–10% after Hib meningitis); results from labyrinthitis via the cochlear aqueduct. All survivors of bacterial meningitis require formal audiological assessment before discharge or within 4–6 weeks.
- Cognitive and learning disabilities: Impaired school performance, attention deficit, memory problems.
- Cerebral palsy: Caused by cortical infarction, vasculitis, and white-matter damage.
- Hydrocephalus (communicating): From arachnoid fibrosis impairing CSF resorption; may require ventriculoperitoneal (VP) shunt.
- Blindness and cranial nerve palsies: CN VI (abducens), CN III, CN VII palsies from basilar meningitis.
CLINICAL PEARL
The 'golden hour' rule for bacterial meningitis: Mortality increases measurably for every hour antibiotics are delayed after presentation. If there is any clinical suspicion of bacterial meningitis and LP is contraindicated or delayed for CT, give empirical antibiotics IMMEDIATELY. A blood culture takes 2 minutes to draw and will remain positive for up to 2 hours after antibiotic initiation — do not let the desire for a 'clean' CSF result delay treatment. The LP can follow once the patient is stabilised and CT is done. Starting antibiotics before LP does NOT make the diagnosis impossible; it makes death less likely.
Management: Antibiotics, Adjunctive Therapy and Supportive Care
The management of acute bacterial meningitis is genuinely time-critical: every hour of delayed antibiotic therapy is associated with measurable increases in mortality and morbidity, and the adjunctive corticosteroid loses much of its benefit if given after the first antibiotic dose. Effective management therefore requires you to act on three simultaneous streams from the moment the diagnosis is suspected — empirical antibiotics calibrated to the patient's age-group organism spectrum, adjunctive dexamethasone administered immediately before or with the first antibiotic dose to blunt the inflammatory cascade, and careful supportive care targeting the acute complications of raised ICP, SIADH, seizures, and haemodynamic instability. Treatment is not sequential; it is parallel. The specific drug choices below follow directly from the pathophysiology and organism-spectrum framework established earlier in this module.
Empirical antibiotic regimen (before culture results):
The critical rule is that the antibiotic choice in the empirical window is driven entirely by the age-stratified organism spectrum:
Neonates (0–28 days):
• Ampicillin (50–100 mg/kg/dose, divided doses) + Cefotaxime (50 mg/kg/dose every 6–8 h) OR Ampicillin + Gentamicin (3–5 mg/kg/day once daily)
• Rationale: Ampicillin covers GBS and Listeria (cephalosporins have no activity against Listeria); cefotaxime or gentamicin covers gram-negative rods (E. coli).
• Ceftriaxone is AVOIDED in neonates <28 days (displaces bilirubin, risk of kernicterus; incompatible with calcium-containing IV fluids).
Infants and children >3 months:
• Ceftriaxone (100 mg/kg/day IV divided every 12 h, max 4 g/day) + Vancomycin (15 mg/kg/dose every 6 h)
• Rationale: Ceftriaxone covers S. pneumoniae, N. meningitidis, and Hib; vancomycin is added because of the rising prevalence of penicillin/cephalosporin-resistant pneumococci. Once cultures confirm a susceptible organism, vancomycin can be discontinued.
Adjunctive dexamethasone:
• Dose: 0.15 mg/kg IV every 6 hours for 4 days
• Timing: must be given before or with the very first antibiotic dose — administering it after antibiotics have already lysed bacterial cell walls provides minimal benefit
• Mechanism: suppresses TNF-α and IL-1β release, reducing BBB breakdown and cochlear inflammation
• Benefit: clearest and best-established for Hib meningitis (significantly reduces incidence of hearing loss); benefit for pneumococcal and other organisms is debated but the standard of care is to give it regardless of confirmed organism, especially where Hib has not been excluded
Supportive care:
• Fluids: In well-perfused patients without shock, restrict to two-thirds maintenance (Holliday-Segar base) to limit SIADH-driven cerebral oedema; switch to full maintenance once eunatraemia is confirmed. In septic shock, volume resuscitate with 10–20 mL/kg normal saline boluses.
• Anti-seizure: Phenobarbitone (20 mg/kg loading dose) or levetiracetam for seizure prophylaxis in high-risk cases; benzodiazepines for active seizures.
• Monitoring: Neurological status every 2–4 hours; serial serum sodium; temperature; blood pressure
• Repeat LP is NOT routinely required unless the child fails to improve or shows clinical deterioration at 48–72 hours.
Duration of therapy (when culture is confirmed):
• GBS, S. pneumoniae: 10–14 days
• N. meningitidis: 5–7 days
• H. influenzae type b: 7–10 days
• Gram-negative bacilli (neonatal): 21 days
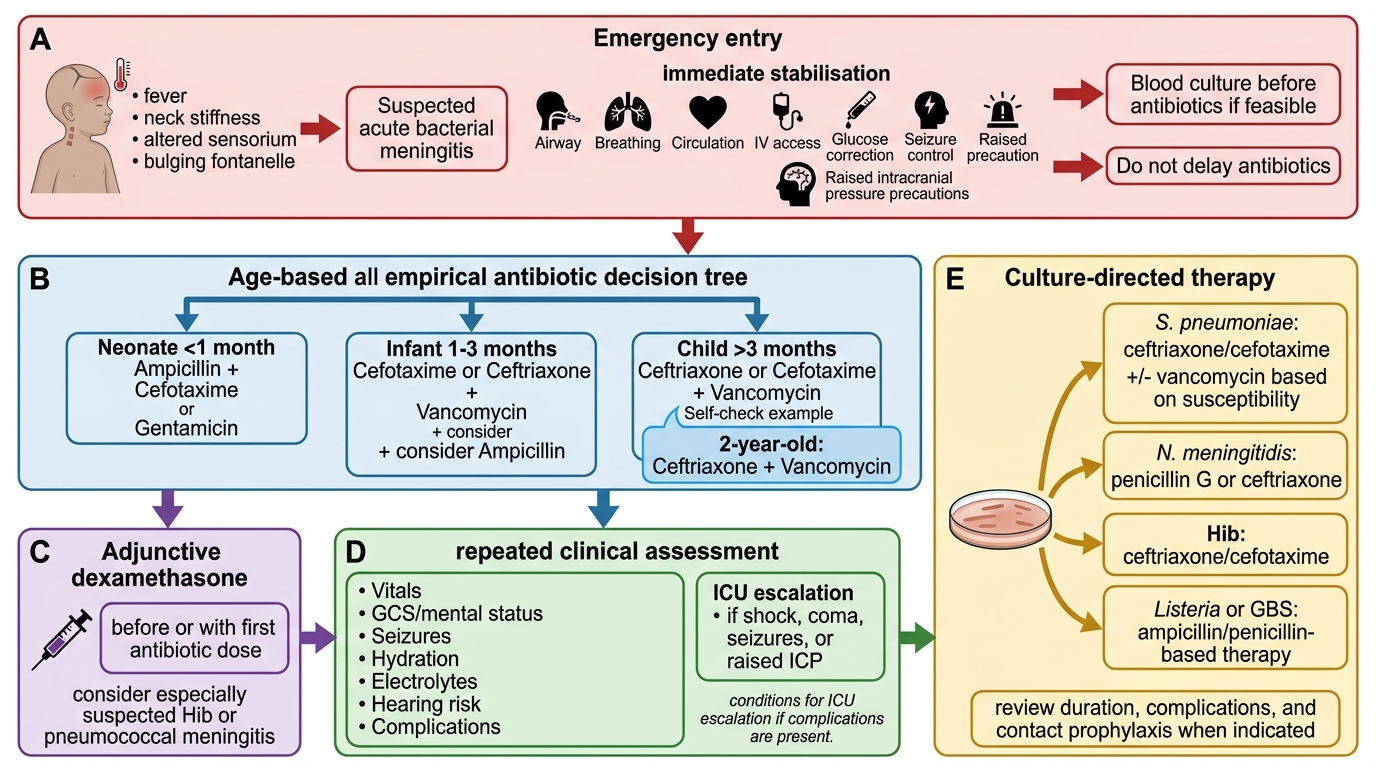
Acute Bacterial Meningitis in Children: Management Algorithm
SELF-CHECK
A 2-year-old child is diagnosed with acute bacterial meningitis. Before starting antibiotics, you draw blood cultures. Empirical therapy is started. Which of the following is the correct empirical antibiotic regimen?
A. Ampicillin + Gentamicin
B. Ceftriaxone alone
C. Ceftriaxone + Vancomycin
D. Ampicillin + Cefotaxime
Reveal Answer
Answer: C. Ceftriaxone + Vancomycin
In children >3 months, the empirical regimen is ceftriaxone (covers S. pneumoniae, N. meningitidis, Hib) PLUS vancomycin (added because of possible penicillin/cephalosporin-resistant S. pneumoniae). Ceftriaxone alone is inadequate if resistant pneumococcus is present. Ampicillin + gentamicin or ampicillin + cefotaxime is used for neonates (where Listeria must be covered by ampicillin and ceftriaxone is avoided due to bilirubin displacement).
Prevention: Vaccination and Chemoprophylaxis
Prevention of bacterial meningitis operates at two distinct levels: primary prevention through vaccination eliminates the risk of disease before it begins, while secondary prevention through chemoprophylaxis limits the spread of infection to close contacts after a case is identified. These are not theoretical measures — the introduction of the Hib conjugate vaccine into national immunisation schedules has resulted in a dramatic, near-complete elimination of Hib meningitis in countries with high coverage, providing direct proof that vaccine-preventable meningitis is a public health failure when it occurs in an immunised child. As a future physician, you will counsel families on vaccination schedules and be responsible for recognising index cases that trigger contact prophylaxis. Both functions depend on knowing exactly which vaccine prevents which organism and which antibiotic eradicates which carrier state.
Vaccination (NIS and IAP-recommended schedules):
- Haemophilus influenzae type b (Hib) vaccine: Included in the pentavalent vaccine (DTP-Hib-HepB) given at 6, 10, and 14 weeks under the national UIP. A booster is given at 16–18 months. The dramatic reduction in Hib meningitis in immunised populations is the strongest evidence for the vaccine's effectiveness in this disease.
- Pneumococcal Conjugate Vaccine (PCV13 or PCV10): Recommended by IAP at 6, 10, and 14 weeks + booster at 12–15 months. Protects against the most common S. pneumoniae serotypes causing meningitis. Not yet universally available under UIP nationwide, but provided in select states and recommended by IAP for all children.
- Meningococcal vaccine (MCV): Conjugate vaccines (MenACWY) recommended by IAP for high-risk groups (asplenia, complement deficiency, travellers to endemic areas), and during outbreaks. Not in routine NIS currently but should be offered where accessible.
- Maternal GBS screening (group B streptococcal disease prevention): IAP guidelines recommend vaginal-rectal swab at 35–37 weeks gestation and intrapartum antibiotic prophylaxis (IV penicillin or ampicillin) for GBS-positive mothers, significantly reducing early-onset neonatal GBS sepsis and meningitis.
Chemoprophylaxis for close contacts:
When a case of meningococcal (N. meningitidis) or Hib meningitis is diagnosed, close household and daycare contacts require antibiotic prophylaxis to eliminate nasopharyngeal colonisation:
- Rifampicin (drug of choice): 10 mg/kg/dose (max 600 mg) orally every 12 hours for 2 days for meningococcal disease; 20 mg/kg/day (max 600 mg) once daily for 4 days for Hib disease
- Ciprofloxacin (single dose, adults): alternative for meningococcal disease where rifampicin is unavailable
- Ceftriaxone (IM single dose) also eradicates meningococcal carriage in pregnancy
Note: Chemoprophylaxis is NOT required for pneumococcal meningitis contacts.