Page 41 of 48
PE27.13-14 | CSF Analysis and Lumbar Puncture — SDL Guide (Part 2)
Performing the Lumbar Puncture: Step-by-Step Technique
Lumbar puncture in children requires meticulous preparation, correct positioning, and a systematic procedural approach. Rushing any step increases the risk of a dry tap (no CSF), a traumatic tap, or patient distress. The following sequence is the standard technique taught in the Ghai and Nelson references and applicable to mannequin practice for PE27.14. A useful mental model is to divide the procedure into four sequential phases — preparation and consent, positioning, aseptic needle insertion and manometry, and specimen collection followed by safe withdrawal. Each phase has its own checklist of steps, and failure at any one phase propagates to the next: a poorly positioned child makes landmark identification unreliable, which leads to an off-midline needle, which produces a dry or traumatic tap. Investing time in correct positioning before touching the needle is the single intervention most likely to make the procedure succeed on the first pass.
Preparation:
- Confirm indication; ensure no contraindication is present
- Explain the procedure to the parents/caregiver and obtain informed consent
- Gather equipment: LP tray with spinal needle (22G for children, 20G for older children/adolescents), manometer, three-way stopcock, sterile drapes, betadine/chlorhexidine solution, sterile gloves, specimen tubes (3-4 numbered), bandage
- Premedicate with adequate analgesia/sedation as per unit protocol (e.g. topical EMLA cream 60 minutes earlier; intranasal midazolam or IV ketamine for anxious children)
Positioning — the single most important factor for success:
- Lateral decubitus (foetal/knee-chest) position: the child lies on their side at the edge of the examination table, with knees flexed toward the chest and neck flexed forward — this opens the interspinous spaces maximally. An assistant holds the child in this position, placing one arm behind the knees and the other behind the neck. This is the standard position for most paediatric LPs.
- Sitting position (used in neonates): the infant is held sitting upright, with neck and trunk slightly flexed. Caution — respiratory compromise can occur in premature infants in this position; monitor carefully.
Aseptic technique:
- Wash hands; apply sterile gloves
- Prepare the skin with betadine or 2% chlorhexidine solution over at least a 10 cm radius around the intended site; allow to dry
- Drape the area with sterile fenestrated drape
- Infiltrate local anaesthetic (1% lignocaine, 0.5-1 mL subcutaneously) at the intended needle site in children old enough to cooperate and not already sedated
Needle insertion:
1. Identify Tuffier's line (iliac crest line = L4) and the L3-L4 or L4-L5 interspace
2. Insert the spinal needle (with stylet in situ) in the midline, angled slightly cephalad (toward the umbilicus — approximately 10-15° in children, who have a less pronounced lumbar lordosis than adults)
3. Advance slowly, feeling for two subtle resistances: ligamentum flavum (first), then dura (second)
4. After the second "give" (dural puncture), stop advancing; withdraw the stylet partially to check for CSF return
5. If CSF is not seen, rotate the needle 90° (bevel direction may be important) or advance by 1-2 mm increments
Manometry:
- Once CSF flows freely, attach the manometer via three-way stopcock
- Record the opening pressure with the child relaxed and legs slightly extended (knee-chest flexion artificially raises pressure)
- Normal opening pressure: 70-180 mmH2O in children
Specimen collection:
- Collect CSF into sequentially numbered tubes (tubes 1, 2, 3, and 4 if available):
- Tube 1: biochemistry (protein, glucose) — collected first
- Tube 2: microbiology (Gram stain, culture, AFB if TB suspected, India ink/CrAg if fungal)
- Tube 3: cell count and differential — last tube to differentiate traumatic tap (tube 1 has more blood, tube 3 less)
- Tube 4 (if available): extra for PCR (HSV, enterovirus, pneumococcal antigen, MTB PCR) or cytology
- Simultaneously send a blood glucose sample to calculate the CSF:blood glucose ratio
Needle removal:
- Replace the stylet before withdrawing the needle (reduces post-LP headache incidence by preventing nerve root entrapment during withdrawal)
- Apply pressure with a sterile swab; apply adhesive dressing
- Lay the child supine; there is no evidence that strict bed rest prevents post-LP headache, but a brief rest period is customary
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
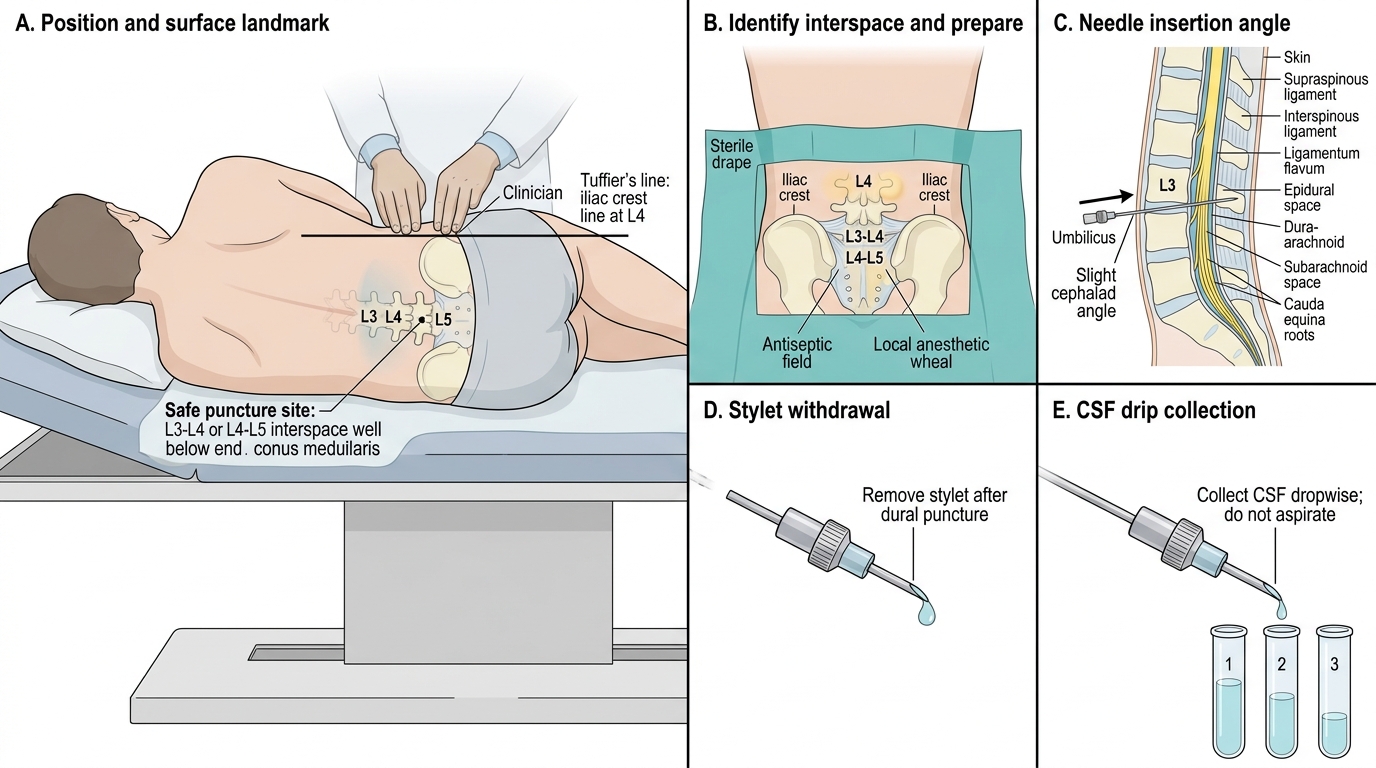
Lumbar Puncture Technique
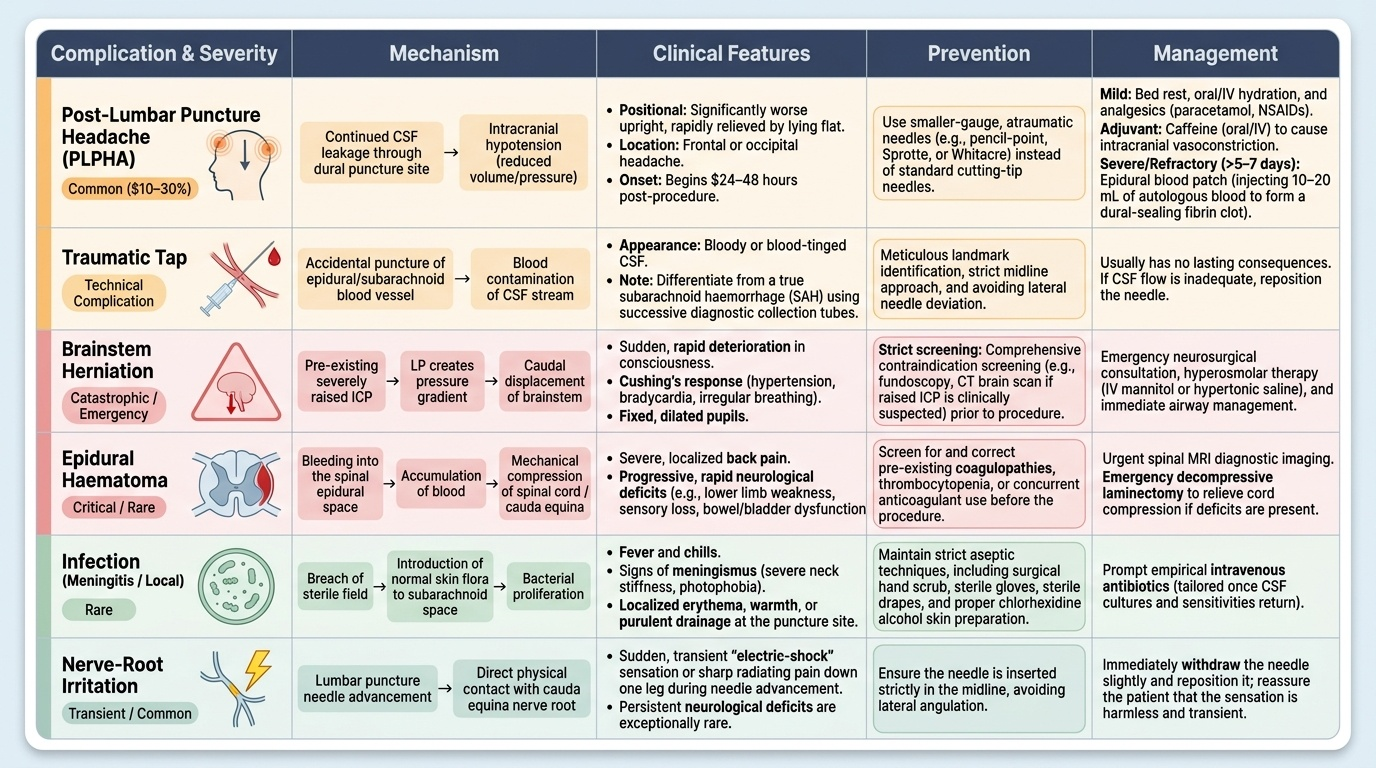
Complications of Lumbar Puncture and Their Management
No procedural SDL is complete without an honest account of complications. Knowing these empowers the clinician to anticipate, prevent, and manage them — and to counsel families honestly before obtaining consent.
Provided image
1. Post-lumbar puncture headache (PLPHA) — the most common complication. It occurs in up to 10-30% of patients and is caused by continued CSF leakage through the dural puncture site leading to intracranial hypotension. It is characteristically positional (worse upright, relieved by lying flat), frontal or occipital, and begins 24-48 hours post-LP. Mild cases resolve with bed rest and adequate oral hydration. Analgesics (paracetamol, NSAIDs) are used for symptomatic relief. Caffeine (oral or IV) can help by causing intracranial vasoconstriction that partially offsets the reduced CSF pressure. For severe or refractory PLPHA lasting more than 5-7 days, an epidural blood patch (10-20 mL of autologous blood injected epidurally at or near the original LP site) creates a fibrin clot that seals the dural leak and provides rapid, often dramatic relief. Using smaller-gauge, atraumatic (pencil-point, Sprotte or Whitacre) needles significantly reduces PLPHA incidence.
2. Traumatic (bloody) tap — occurs when the needle pierces an epidural or subarachnoid vessel. The CSF appears bloody. This is an important finding to characterise (see the next section on differentiating traumatic tap from SAH). In most cases it is a technical complication with no lasting consequence; the needle is repositioned if CSF flow is inadequate.
3. Herniation — the most feared and catastrophic complication, occurring when LP in a patient with raised ICP causes sudden caudal displacement of the brainstem. Signs: sudden deterioration in consciousness, Cushing's response, fixed dilated pupils. Prevention rests entirely on correct contraindication screening.
4. Local infection / meningitis — rare with strict aseptic technique. Breach of sterility can introduce skin flora (Staphylococci, Propionibacterium) into the subarachnoid space.
5. Nerve-root irritation / radicular pain — transient electric-shock sensation radiating to one leg at needle insertion; resolves when the needle is repositioned. Persistent neurological deficit is exceptionally rare.
6. Epidural haematoma — bleeding into the epidural space causing cord compression; risk is dramatically elevated in coagulopathy; presents as backache progressing to lower limb weakness and bladder dysfunction. Requires urgent MRI and neurosurgical decompression.
7. Failed (dry) tap — no CSF obtained. Most common causes: incorrect positioning (inadequate flexion), off-midline needle trajectory, or level too low. Remedy: reposition, reassess landmarks, try the adjacent interspace.
CLINICAL PEARL
Always replace the stylet before withdrawing the LP needle. This single step significantly reduces the incidence of post-LP headache. The mechanism: without the stylet, a strand of arachnoid or nerve root can be caught in the needle tip and drawn outward as the needle is pulled, creating a persistent CSF fistula through the dura. With the stylet replaced, the tip is sealed. Studies in adult populations show this reduces PLPHA from ~36% to ~5%. Apply this practice every single time — it costs nothing and prevents the most common post-procedural complaint (Ghai Essential Pediatrics, Nelson Textbook of Pediatrics).
SELF-CHECK
During lumbar puncture of a 7-year-old, CSF stops flowing after 1 mL is collected. The most likely cause and immediate corrective action is:
A. Needle has entered the subdural space — withdraw 5 mm
B. A nerve root is intermittently occluding the bevel — rotate the needle 90° and check flow
C. The subarachnoid space has been depleted — stop collecting
D. The manometer tubing is kinked — remove the manometer entirely
Reveal Answer
Answer: B. A nerve root is intermittently occluding the bevel — rotate the needle 90° and check flow
Intermittent or sudden cessation of flow during LP most often results from a cauda equina nerve root resting against the needle bevel, transiently occluding it. Rotating the needle 90° (changing the bevel direction) frees the root and usually restores flow immediately. Withdrawing 5 mm risks leaving the subarachnoid space. The subarachnoid space is not a finite reservoir that depletes over 1 mL. Manometer removal is not indicated when the problem is at the needle tip.
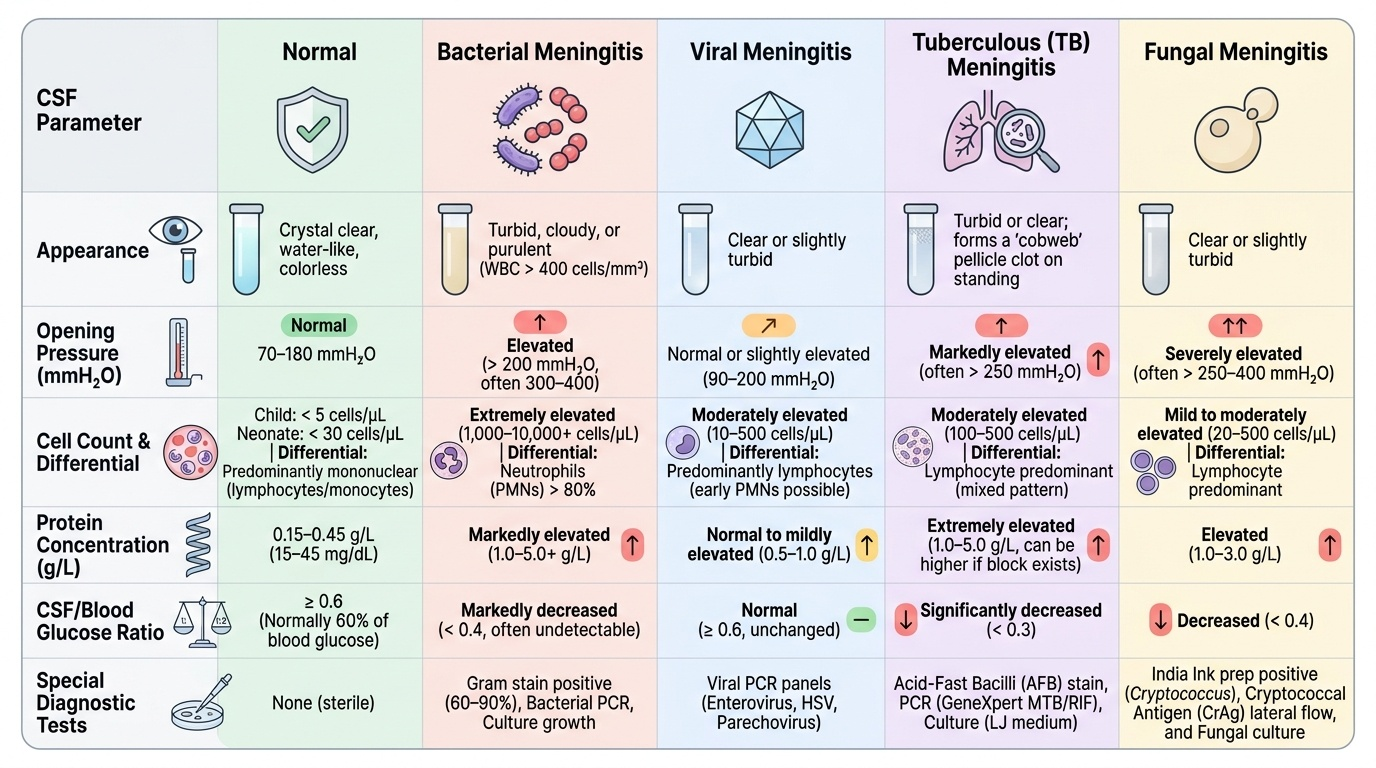
Interpreting CSF Analysis: Normal and Abnormal Findings
Accurate CSF interpretation requires a systematic approach — examining each parameter in isolation and then synthesising the pattern across all parameters simultaneously. No single CSF value alone establishes a diagnosis; it is the constellation that guides clinical decision-making. The following framework covers the five key CSF parameters examined in every sample, followed by a comparison table of the major diagnostic patterns encountered in paediatric practice.
Provided image
Parameter 1 — Appearance:
Hold the collection tube against a white background in good light. Normal CSF is crystal clear, water-like, colourless. Turbidity or cloudiness (opalescence) indicates a white cell count above approximately 400 cells/mm³ and is strongly associated with bacterial meningitis. Xanthochromia — a yellow or orange discolouration — indicates breakdown products of haemoglobin (oxyhaemoglobin → bilirubin) in CSF, occurring 2-4 hours after haemorrhage and persisting for up to 2-3 weeks; it is the hallmark of subarachnoid haemorrhage (not traumatic tap) and of severe jaundice or very high protein. A pellicle (cobweb clot) forms in TB meningitis due to the high protein content.
Parameter 2 — Pressure:
Normal opening pressure in children is 70-180 mmH2O (measure with the child relaxed, legs slightly straightened from the full knee-chest position). Elevated pressure (>200 mmH2O) is seen in bacterial meningitis (often >300-400 mmH2O), cryptococcal meningitis (often very high), and idiopathic intracranial hypertension. Reduced pressure occurs with dehydration or spinal block above the LP site.
Parameter 3 — Cell count and differential:
Normal: <5 white cells/mm³, ALL mononuclear (lymphocytes). Any polymorphonuclear (PMN/neutrophil) pleocytosis is pathological and strongly suggests bacterial infection. The cell count in bacterial meningitis typically runs in the hundreds to thousands (predominantly PMNs). Viral and TB meningitis predominantly show lymphocytic pleocytosis — though very early viral meningitis and listeria meningitis can transiently show neutrophils. Red cell count should be recorded on tube 1 and tube 3 to assess for traumatic tap.
Parameter 4 — Protein:
Normal CSF protein is 20-45 mg/dL. Protein is elevated in any inflammatory condition (the blood-brain barrier becomes leaky). Markedly elevated protein (>100 mg/dL) is typical of bacterial meningitis; protein >500 mg/dL is characteristic of Guillain-Barré syndrome (albuminocytological dissociation — high protein with normal cell count) and advanced TB meningitis. Mildly elevated protein (50-100 mg/dL) is seen in viral meningitis.
Parameter 5 — Glucose (and CSF:blood glucose ratio):
Always request a simultaneous blood glucose — the CSF glucose must be interpreted as a ratio. Normal CSF glucose is approximately 45-75 mg/dL; normal CSF:blood glucose ratio ≥0.6 (i.e., CSF glucose should be at least 60% of the simultaneous serum glucose). A ratio <0.4 is low and indicates bacterial, TB, or fungal meningitis — the organisms and the intense inflammatory response consume glucose. Viral meningitis characteristically has normal CSF glucose and a ratio ≥0.6, which is one of the most useful distinguishing features.
Special tests:
- Gram stain — positive in 60-90% of bacterial meningitis (highest yield in pneumococcal meningitis)
- Culture — gold standard for bacterial identification and antibiotic sensitivity; positive in 70-85%
- AFB smear and culture — low sensitivity (AFB smear ~20-40%) but essential if TB meningitis suspected
- India ink stain and CrAg — cryptococcal meningitis (immunocompromised children, HIV)
- PCR panels — HSV (essential in encephalitis), enterovirus, MTB, S. pneumoniae, N. meningitidis — increasingly available and sensitive