Page 42 of 48
PE27.13-14 | CSF Analysis and Lumbar Puncture — SDL Guide (Part 3)
Differentiating Traumatic Tap from True Subarachnoid Haemorrhage
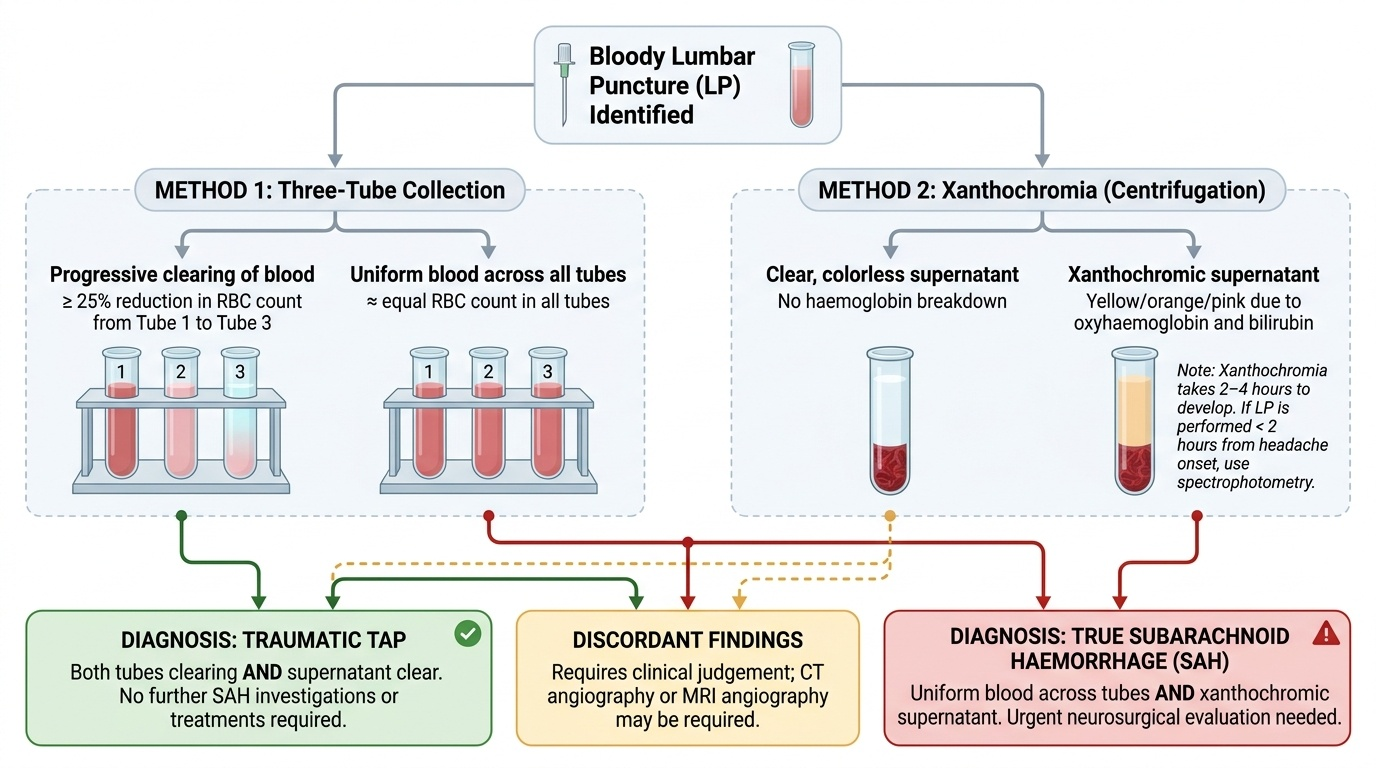
A bloody LP is a common dilemma that must be resolved correctly — treating a traumatic tap as SAH leads to unnecessary and potentially harmful investigations, while dismissing true SAH as a traumatic tap can have fatal consequences. The two conditions are distinguished by two methods, used together.
Provided image
Method 1 — The three-tube (or four-tube) sequential collection method:
During LP collection, blood from a traumatic vessel puncture is progressively diluted by the CSF flow. In a traumatic tap, the RBC count decreases progressively from tube 1 to tube 3 (and tube 4). In true SAH, blood has been mixed uniformly with CSF since the haemorrhage; there is no clearing — the RBC count is approximately equal across all tubes. As a rough guide, a ≥25% reduction in RBC count from tube 1 to tube 3 suggests traumatic tap.
Method 2 — Xanthochromia:
Centrifuge the CSF specimen. Examine the supernatant (the fluid above the spun-down cells):
- Traumatic tap: supernatant is clear and colourless (the RBCs were freshly introduced; there has been no time for haemoglobin breakdown to xanthochromic pigments)
- True SAH: supernatant is xanthochromic (yellow, orange, or pink) due to oxyhaemoglobin and bilirubin formed from red cell lysis that occurred hours to weeks earlier
Xanthochromia develops approximately 2-4 hours after haemorrhage and persists for up to 2-3 weeks. This means that if the clinical suspicion for SAH is high but the LP is performed within 2 hours of headache onset, xanthochromia may not yet be detectable — in that scenario, spectrophotometry (laboratory measurement of oxyhaemoglobin/bilirubin absorbance) is more sensitive than visual inspection.
Summary of the decision rule:
- Both tubes clearing AND supernatant clear → traumatic tap
- Uniform blood across tubes AND xanthochromic supernatant → true SAH
- Discordant findings → clinical judgement; CT angiography or MRI angiography may be required
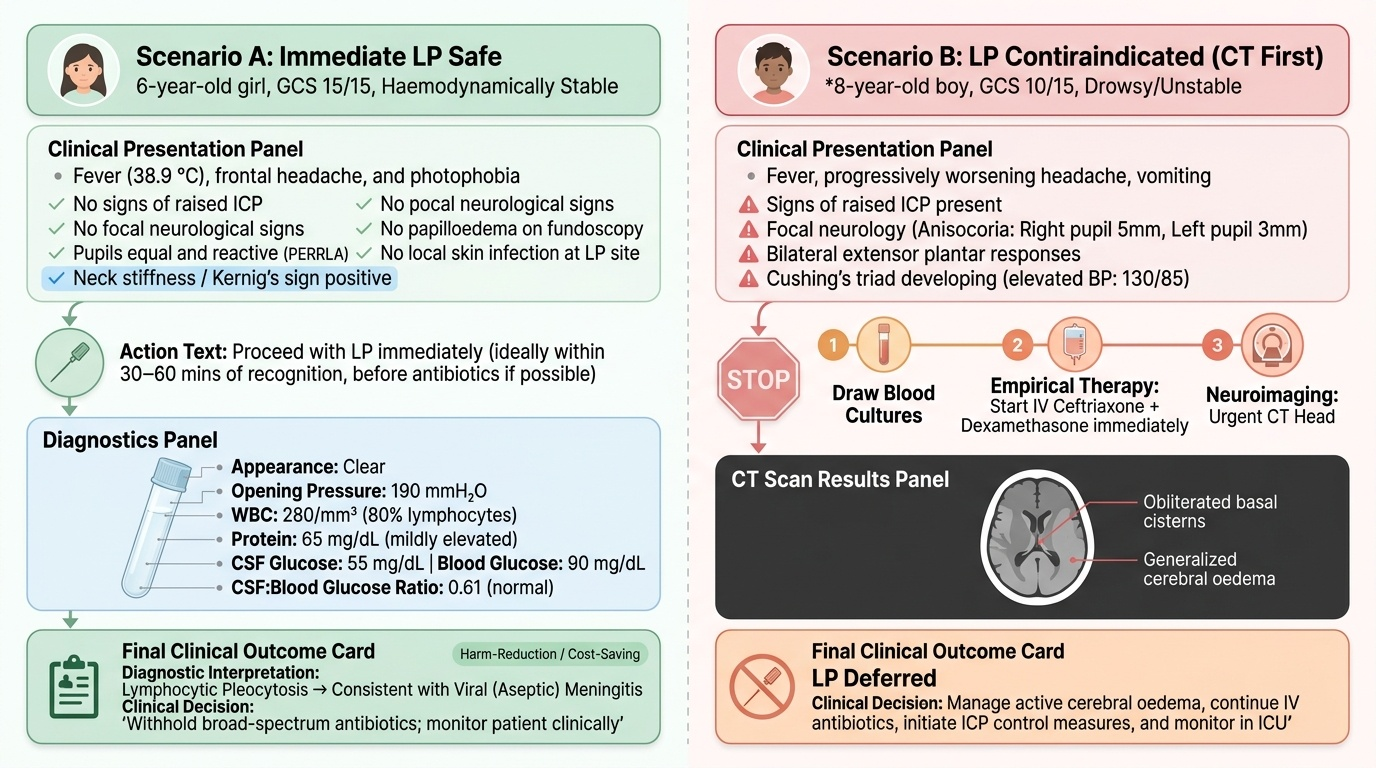
Applied Practice: Clinical Scenarios and Decision-Making
Apply your knowledge through these two paediatric clinical scenarios, each requiring a different decision pathway. Work through each before reading the discussion.
Provided image
Scenario A — Proceed with LP:
A 6-year-old girl presents with 3 days of fever (38.9 °C), frontal headache, and photophobia. She is alert, oriented, and able to cooperate. Examination shows Kernig's sign positive, neck stiffness, but pupils are equal and reactive, no papilloedema on fundoscopy, no focal neurological signs, and GCS 15/15. There is no local skin infection at the lumbar area. She is haemodynamically stable.
Decision: Safe to proceed with LP immediately. No contraindications are present — she has no signs of raised ICP, no focal neurology, no papilloedema, is haemodynamically stable, and has no local infection. Obtain LP before antibiotics if this can be done within 30-60 minutes of recognition. Her LP shows: clear CSF, pressure 190 mmH2O, WBC 280/mm³ (80% lymphocytes), protein 65 mg/dL, glucose 55 mg/dL; simultaneous blood glucose 90 mg/dL → CSF:blood ratio = 0.61. Interpretation: lymphocytic pleocytosis with normal glucose ratio and mildly elevated protein — this pattern is consistent with viral meningitis (aseptic meningitis). Gram stain is negative, culture is pending. This pattern supports withholding broad-spectrum antibiotics and monitoring — a clinically important cost and harm-reduction decision.
Scenario B — CT before LP:
An 8-year-old boy presents with fever, a 12-hour history of progressively worsening headache, one episode of vomiting, and increasing drowsiness. GCS is 10/15. Examination reveals: right pupil 5 mm, left pupil 3 mm (anisocoria), no response to verbal command, neck stiffness, and bilateral extensor plantar responses. Blood pressure is 130/85 (Cushing's triad developing).
Decision: Do NOT proceed with LP. This child has multiple signs of raised ICP with focal neurology (pupillary asymmetry, extensor response, GCS ≤10). Immediate action: draw blood cultures → start empirical ceftriaxone + dexamethasone IV immediately (do not delay beyond 30 minutes) → urgent CT head. If CT shows no mass lesion and cisterns are patent, LP may then be performed. His CT reveals obliterated basal cisterns consistent with generalised cerebral oedema. LP is deferred; he is managed with antibiotics, dexamethasone, and ICP management (head elevation, osmotherapy with mannitol 0.5 g/kg IV). CSF is obtained the following day after clinical stabilisation.
Synthesis: The two scenarios illustrate that the LP decision is always a clinical judgement integrating neurological status, presence or absence of raised ICP signs, urgency of the indication, and available imaging. The microbiological yield of LP is high if obtained before antibiotics; however, antibiotic safety always takes precedence over microbiological elegance.
Self-Assessment: LP Decision-Making and CSF Interpretation
Test your understanding of the core concepts from this module with the following self-check questions. Attempt each before reading the answer.
Self-check 1: A spinal needle is inserted in the L3-L4 interspace of an 8-year-old. Name in order the five ligamentous/meningeal structures the needle tip traverses before CSF is obtained.
Answer: Supraspinous ligament → interspinous ligament → ligamentum flavum (first resistance) → dura mater (second resistance) → arachnoid mater → subarachnoid space (CSF obtained). Note: subdural space is potential and not routinely encountered as a distinct structure.
Self-check 2: CSF results from a 5-year-old with fever and neck stiffness: turbid appearance, pressure 320 mmH2O, WBC 1,800/mm³ (92% PMNs), protein 180 mg/dL, glucose 18 mg/dL (simultaneous blood glucose 90 mg/dL → ratio 0.20). What is the most likely diagnosis, and what is the empirical antibiotic of choice in India?
Answer: This CSF pattern — turbid, elevated pressure, PMN pleocytosis in the hundreds-to-thousands, high protein, low glucose (ratio <0.4) — is classic for bacterial meningitis. The most common organisms in a 5-year-old are Streptococcus pneumoniae and Haemophilus influenzae (post-Hib vaccine era, pneumococcus predominates). Empirical treatment: ceftriaxone 100 mg/kg/day IV in 2 divided doses + dexamethasone 0.15 mg/kg 6-hourly for 4 days (to reduce hearing loss from the inflammatory cascade, especially in pneumococcal and Hib meningitis). (Refer IAP Guidelines on Bacterial Meningitis.)
Self-check 3: An LP is performed on a 10-year-old with suspected meningitis. Tube 1 RBC = 10,000/mm³; Tube 3 RBC = 2,000/mm³. Centrifuged CSF supernatant is crystal clear. What is your interpretation?
Answer: The RBC count falls progressively from tube 1 to tube 3 (80% reduction) AND the supernatant is clear (no xanthochromia) — this is consistent with a traumatic (bloody) tap. True SAH would show uniform RBC counts across tubes and a yellow/orange (xanthochromic) supernatant. No further investigation for haemorrhage is indicated based on these CSF findings alone.
SELF-CHECK
A 9-year-old's CSF shows: clear appearance, pressure 155 mmH2O, WBC 320/mm³ (95% lymphocytes), protein 58 mg/dL, glucose 62 mg/dL (blood glucose 95 mg/dL). Gram stain is negative. Which diagnosis does this pattern BEST support?
A. Bacterial meningitis
B. Tuberculous meningitis
C. Viral (aseptic) meningitis
D. Fungal meningitis
Reveal Answer
Answer: C. Viral (aseptic) meningitis
Viral (aseptic) meningitis is characterised by: clear CSF, normal or mildly elevated pressure, predominantly lymphocytic pleocytosis, mildly elevated protein, and — most importantly — NORMAL CSF glucose with a normal CSF:blood glucose ratio (62/95 = 0.65, well above 0.6). Bacterial meningitis shows PMN predominance and low glucose ratio. TB meningitis shows low glucose with very high protein (often >100-500 mg/dL) and may show xanthochromia or pellicle. Fungal meningitis also shows low glucose, is rare without immunocompromise, and requires India ink/CrAg testing.