Page 16 of 48
PE27.5 | Infantile Hemiplegia — SDL Guide
Learning Objectives
- Describe the clinical features of infantile hemiplegia including UMN signs and comorbidities
- Explain the prenatal, perinatal, and postnatal aetiopathogenesis
- Classify cerebral palsy by motor type and topography; apply the GMFCS
- Outline a logical investigative and management approach for a child with hemiplegia
INSTRUCTIONS
Infantile hemiplegia is one of the most common causes of unilateral motor disability encountered in general paediatric practice. Recognising its clinical hallmarks early — asymmetric hand preference, fisting, brisk reflexes — enables timely rehabilitation that exploits the remarkable neuroplasticity of the developing brain. This module walks you through the aetiology, classification within the cerebral palsy framework, investigation, and multidisciplinary management.
References
- Ghai Essential Pediatrics, 9th ed., Ch 18 (Neurology) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 616 (Cerebral Palsy) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 10-month-old boy is brought by his mother who is worried: "He always uses his right hand but never the left — he keeps it fisted." On examination he has brisk deep tendon reflexes on the left, a left Babinski sign, and reduced spontaneous movement of the left arm and leg. He sat without support only last month (slightly delayed). There is no family history of neurological disease, and he was born full-term after an uneventful pregnancy. His mother is anxious: 'Will he ever use his hand normally?' This child's presentation is the clinical hallmark of infantile hemiplegia — a unilateral upper motor neurone deficit acquired in the first two years of life, most commonly within the spectrum of hemiplegic cerebral palsy (CP).
WHY THIS MATTERS
Hemiplegic CP is the most common topographic subtype of CP seen in term-born children, with an incidence of approximately 0.6–0.7 per 1000 live births in India. Paediatricians and general practitioners are the first point of contact for parents who notice that their child favours one hand or has asymmetric motor development. Early diagnosis allows early enrolment into physiotherapy and constraint-induced movement therapy programmes during the window of maximal neuroplasticity (before age 4–5 years), substantially improving functional outcomes. A minority of affected children also develop epilepsy and cognitive impairment, requiring proactive surveillance and multidisciplinary coordination — skills that every final-year student must master.
RECALL
Before proceeding, recall from Physiology (PY) and Anatomy (AN): the corticospinal (pyramidal) tract runs from the primary motor cortex → posterior limb of the internal capsule → cerebral peduncle → decussates in the medullary pyramids → contralateral spinal cord. An upper motor neurone (UMN) lesion above the decussation produces contralateral spasticity, hyperreflexia, extensor plantar response (Babinski sign), and weakness without wasting. In contrast, a lower motor neurone (LMN) lesion produces ipsilateral flaccidity, hyporeflexia, and wasting. Infantile hemiplegia is a UMN lesion — understanding the tract anatomy explains every physical sign you will find.
Clinical Presentation of Infantile Hemiplegia
Infantile hemiplegia is defined as a unilateral upper motor neurone deficit that is acquired before two years of age. When the deficit is non-progressive and results from a static brain lesion acquired prenatally or perinatally, it falls within the clinical spectrum of hemiplegic cerebral palsy. The most reliable early sign is asymmetric hand preference before 12 months of age — normally, hand dominance does not emerge until 18–24 months; hand preference before this age indicates that the opposite hand is being used because the preferred hand cannot be used normally. The affected hand adopts a characteristic fisted posture with the thumb tucked inside, and the wrist and elbow may be mildly flexed.
On formal neurological examination, the affected limbs — upper limb more severely than lower in most cases — show:
• Spasticity: increased tone in a velocity-dependent manner (clasp-knife character on rapid stretch)
• Hyperreflexia: brisk or exaggerated deep tendon reflexes (biceps, triceps, knee, ankle)
• Positive Babinski sign (extensor plantar response)
• Weakness: reduced voluntary movement, difficulty releasing objects
• Reduced arm swing on the affected side when the child begins to walk
• Circumduction gait with equinus posture of the affected foot when walking begins
Motor developmental milestones may be globally delayed or only mildly affected depending on lesion extent. Because the contralateral (unaffected) hemisphere is normal, cognitive development may be preserved, especially in unilateral strokes confined to motor cortex.
Sensory involvement (hemisensory loss — reduced pain/temperature and proprioception) occurs in a minority but may contribute to the functional disability and is often underrecognised. Homonymous hemianopia (ipsilateral visual field cut from optic radiation involvement) occurs when the lesion extends to the parieto-occipital cortex.
In the clinic, the priority is to document:
1. Age of symptom onset (parent observation of hand preference / motor asymmetry)
2. Course — static (cerebral palsy) vs progressive (metabolic, tumour, demyelination)
3. Presence of seizures (comorbid epilepsy in ~35–40%)
4. Developmental trajectory across all streams (motor, language, cognitive, social)
Pathophysiology and Aetiology
The pathological substrate of infantile hemiplegia is a unilateral injury to the corticospinal tract at any level — motor cortex, subcortical white matter, internal capsule, or descending tracts — acquired during a period when the brain is still developing. The resultant clinical picture is shaped both by the site and timing of the insult and by the compensatory plasticity of the developing hemisphere. It is important to remember that the underlying cause is not always identified clinically before MRI is performed; the imaging appearance itself guides aetiological classification. Timing matters enormously: a lesion at 20 weeks of gestation produces a very different imaging pattern from a perinatal arterial stroke at 38 weeks, even though both eventually produce a similar clinical picture of hemiplegia. Understanding the timing-cause-mechanism triad enables targeted aetiological workup and counselling of families regarding recurrence risk and prognosis.
Prenatal causes (occurring before 28 weeks gestation or structurally at birth):
• Cerebral cortical dysplasia / malformation — focal polymicrogyria, hemimegalencephaly, or schizencephaly disrupts the normal laminar architecture of the motor cortex. The cleft (schizencephaly) or excess small convolutions (polymicrogyria) result in disorganised motor representation and early-onset epilepsy in addition to hemiplegia.
• Prenatal arterial ischaemic stroke — in-utero occlusion of the middle cerebral artery (MCA) — the most common site — produces a large periventricular or corticosubcortical infarct; detected incidentally on postnatal imaging as porencephalic cyst.
• Periventricular leukomalacia (PVL) — ischaemic injury to periventricular white matter, predominantly in preterm infants, injures the corticospinal fibres as they run close to the ventricles.
Perinatal causes (around the time of birth, typically in term infants):
• Hypoxic-ischaemic encephalopathy (HIE) — generalised hypoxia-ischaemia may cause asymmetric cortical/subcortical injury particularly if there is focal vascular territory vulnerability, resulting in hemiplegia rather than diplegia.
• Neonatal arterial ischaemic stroke — thromboembolism of the MCA (left > right) presenting as neonatal seizures; the most common cause of congenital hemiplegia in term neonates. Risk factors: maternal thrombophilia, cardiac defects, polycythaemia, perinatal infection.
• Neonatal haemorrhagic stroke — intraparenchymal haemorrhage from arteriovenous malformation (AVM) or haemostatic disorder.
Postnatal causes (acquired after 1 month of age — "acute hemiplegia of childhood"):
• Acute encephalitis — viral (herpes simplex encephalitis — unilateral temporal lobe tropism), bacterial meningitis with cerebrovascular complication, or autoimmune encephalitis.
• Cerebrovascular accidents — sickle cell disease (moyamoya-like vasculopathy), cardioembolism (cyanotic CHD, cardiomyopathy), thrombophilia, or MELAS (mitochondrial encephalopathy with lactic acidosis and stroke-like episodes).
• Trauma — severe traumatic brain injury (TBI), non-accidental injury.
• Hemiconvulsion-hemiplegia-epilepsy (HHE) syndrome — prolonged febrile or afebrile seizures in a young child cause unilateral ischaemic/oedematous injury producing ipsilateral (to the seizure) hemiplegia followed by epilepsy.
The neuroplasticity of the immature brain is a key pathophysiological concept: the contralateral (unaffected) hemisphere can partially compensate for the injured hemisphere, particularly when the lesion occurs early. Ipsilateral corticospinal projections from the unaffected hemisphere may reinforce control of the affected hand — the basis of constraint-induced movement therapy.
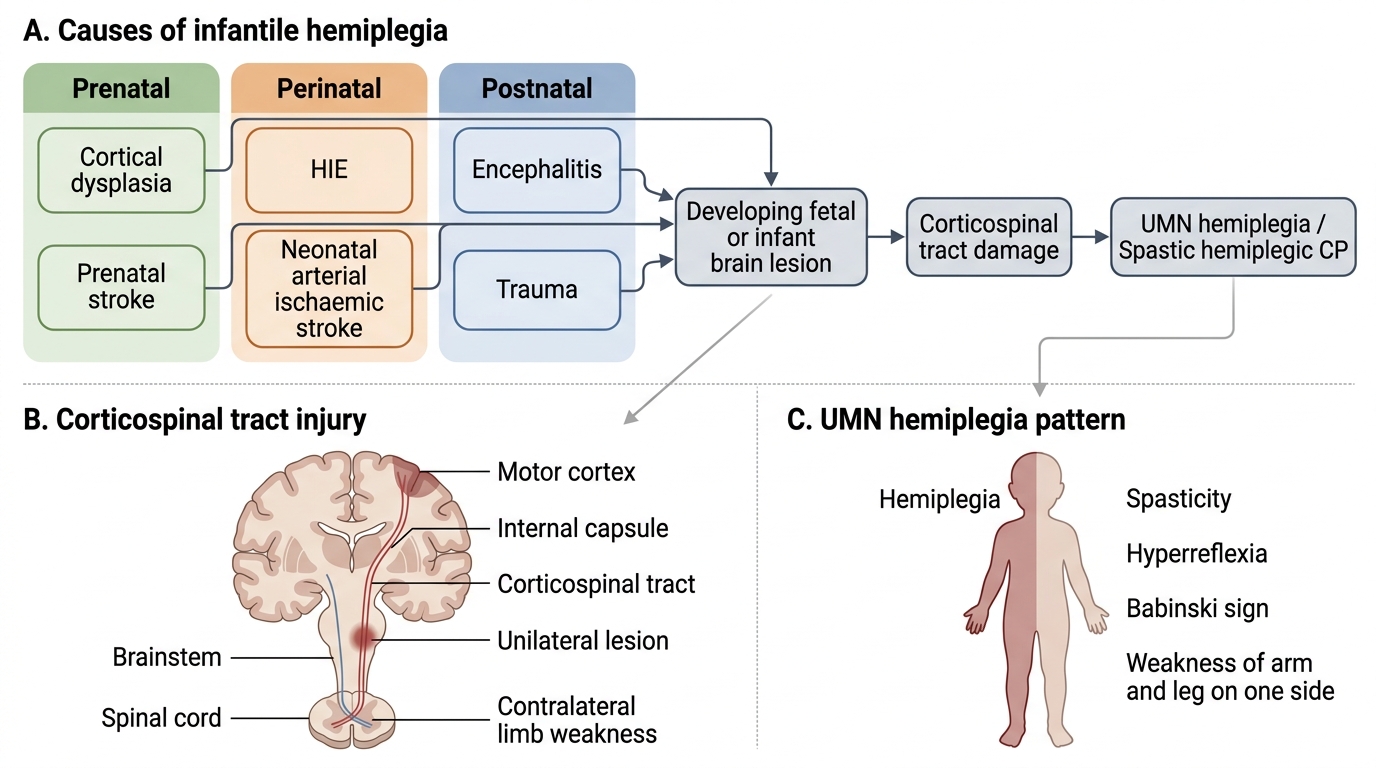
Causes and Mechanism of Infantile Hemiplegia
Types: Cerebral Palsy Classification and GMFCS
Cerebral palsy (CP) is defined as a group of permanent disorders of movement and posture, causing activity limitation, attributed to non-progressive disturbances in the developing fetal or infant brain. Infantile hemiplegia most commonly represents the hemiplegic topographic subtype of CP when the lesion is acquired prenatally or perinatally. Understanding the full CP classification helps you place infantile hemiplegia accurately within the spectrum and anticipate associated impairments. CP is classified by two independent axes: first, the predominant motor type (which reflects the pathological substrate and movement quality), and second, the topographic distribution of affected limbs (which reflects lesion location and extent). Applying both axes together gives a complete clinical description — for example, 'spastic hemiplegic CP, GMFCS level II' — and directly informs prognosis, rehabilitation planning, and orthopaedic surveillance. Knowing the classification also prevents a common error: assuming that all CP is the same.
Classification by motor type (tone/movement quality):
| Type | Motor feature | Pathological substrate |
|---|---|---|
| Spastic (most common ~80%) | Velocity-dependent increased tone; hyperreflexia; Babinski | Corticospinal tract / periventricular white matter |
| Dyskinetic (athetoid/dystonic ~15%) | Involuntary writhing (athetosis) or sustained twisting (dystonia); variable tone | Basal ganglia (putamen) ± thalamus |
| Ataxic (rare ~5%) | Hypotonia, broad-based gait, incoordination, nystagmus | Cerebellar pathways |
| Mixed | Features of ≥2 types | Combined corticospinal + extrapyramidal |
Topographic subtypes of spastic CP:
• Hemiplegia — one side (arm > leg); term infants, MCA territory lesions
• Diplegia — both legs > arms; predominantly preterm, PVL
• Quadriplegia (tetraplegia) — all four limbs severely affected; diffuse brain injury
The Gross Motor Function Classification System (GMFCS) is a five-level functional classification (not an impairment scale):
| Level | Functional ability |
|---|---|
| I | Walks indoors and outdoors without restriction; runs and climbs |
| II | Walks most settings; limitations on uneven terrain, stairs without handrail |
| III | Walks with a hand-held mobility device; uses wheeled mobility outdoors |
| IV | Uses wheeled mobility most of the time; limited independent movement |
| V | Transported in manual wheelchair; severely limited even in supported positions |
Most children with hemiplegic CP function at GMFCS levels I–III — emphasising that despite the motor deficit, the majority ambulate independently. GMFCS level is relatively stable after age 4–5 years and guides prognosis and rehabilitation goals.
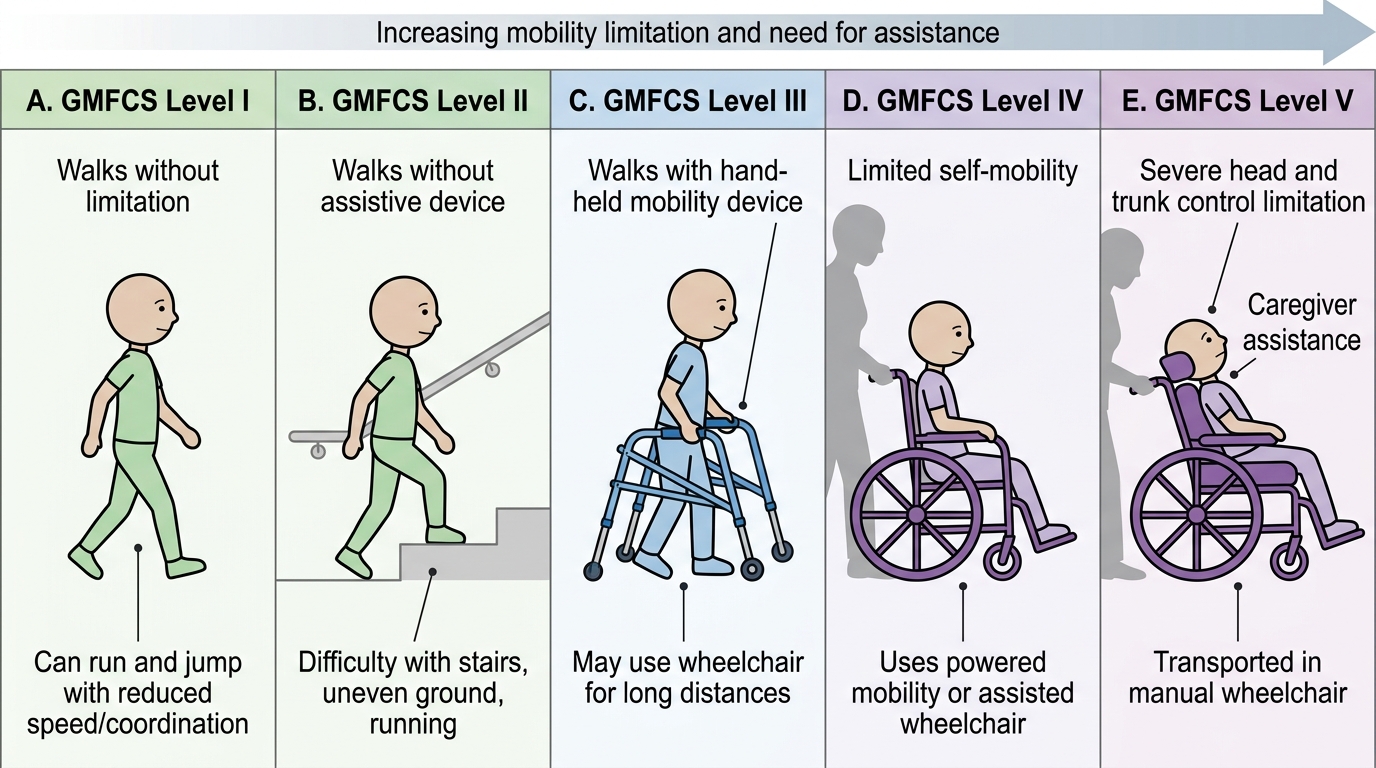
GMFCS Levels I-V: Child Mobility and Functional Ability