Page 17 of 48
PE27.5 | Infantile Hemiplegia — SDL Guide (Part 2)
Associated Comorbidities
Infantile hemiplegia is not simply a motor disorder; the same brain lesion that disrupts the corticospinal tract may also injure adjacent structures, producing a constellation of neurodevelopmental comorbidities that are often clinically more disabling than the motor deficit itself. Systematic surveillance for these comorbidities is essential at every follow-up visit.
Epilepsy is the most significant comorbidity, occurring in approximately 35–40% of children with hemiplegic CP. Seizure onset is often within the first year of life, though it can emerge in late childhood. The semiology depends on the lesion site — focal onset impaired awareness seizures (temporal/parietal) and focal tonic/clonic seizures (frontal) are characteristic. Drug-resistant epilepsy is commoner in cortical dysplasia than in stroke-related hemiplegia. For drug-resistant cases with clear unilateral lesion and concordant EEG, hemispherotomy (disconnection surgery) offers the best chance of seizure freedom.
Cognitive and intellectual impairment affects 20–50% of children with hemiplegic CP; severity correlates with lesion extent. When the left hemisphere is dominant and the lesion is extensive, expressive language delay and reading difficulties are common. Lesions confined to motor cortex with sparing of association areas may leave cognition entirely intact.
Sensory deficits — hemiaesthesia (impaired touch, proprioception, two-point discrimination) — occur when the parietal sensory cortex or thalamocortical projections are involved. These impair the functional use of the affected hand even after motor recovery and are a target of sensory rehabilitation.
Visual impairment: homonymous hemianopia from optic radiation involvement or visual-field restriction due to occipital involvement; strabismus from imbalanced oculomotor input. Eye examination and visual field testing should be routine.
Behavioural and emotional problems: attention deficit hyperactivity disorder (ADHD), anxiety, and low self-esteem are overrepresented. Fatigue is prominent — the metabolic cost of walking with spasticity is significantly higher than for able-bodied peers.
Orthopaedic complications: progressive equinus deformity (heel-cord shortening), hip subluxation/dislocation (especially GMFCS III–V), scoliosis, and leg-length discrepancy from limb growth retardation on the affected side. Orthopaedic surveillance with serial Reimer's index (hip migration percentage) is standard practice.
Communication and feeding difficulties are less common in pure hemiplegia than in bilateral CP but may occur when the dominant hemisphere is affected.
SELF-CHECK
A 9-month-old infant consistently uses her right hand for reaching and keeps her left hand fisted. On examination, left biceps reflex is brisk and there is a left Babinski sign. Which single investigation will best define the nature and extent of the brain lesion?
A. CT brain without contrast
B. MRI brain with and without contrast
C. EEG
D. Nerve conduction studies
Reveal Answer
Answer: B. MRI brain with and without contrast
MRI brain is the investigation of choice in infantile hemiplegia. It provides superior soft-tissue resolution to CT, clearly delineating cortical dysplasia, periventricular leukomalacia, porencephalic cysts, and stroke evolution (DWI for acute; FLAIR/T2 for chronic lesions). CT is useful in emergencies (haemorrhage, trauma) but misses subtle cortical malformations. EEG characterises associated epilepsy but does not identify the structural lesion. Nerve conduction studies assess LMN pathways and are not relevant for a UMN hemiplegia.
Diagnosis and Investigation
The diagnosis of infantile hemiplegia is primarily clinical — based on the history of early asymmetric motor development and the neurological findings of UMN hemiplegia. Investigations serve four distinct purposes: first, to establish the underlying aetiology (structural, vascular, metabolic, or malformative) so that aetiologically specific counselling and management can be provided; second, to characterise the epilepsy if present, since seizure type determines AED selection; third, to quantify associated neurodevelopmental impairments across cognitive, language, sensory, and behavioural domains; and fourth, to screen for orthopaedic complications and monitor hip development. A structured investigative approach — rather than a blanket battery of tests — saves resources and guides intervention. The order of priority is neuroimaging first (defines the lesion), EEG second (if seizures or suspected), and developmental and aetiological workup thereafter based on the clinical context.
Neuroimaging:
• MRI brain (with and without contrast; include DWI for acute presentations) is the single most important investigation. It identifies the structural lesion in >90% of children with CP.
- Porencephalic cyst in MCA territory → prenatal or perinatal stroke
- Periventricular leukomalacia (PVL) — bilateral but asymmetric periventricular white matter signal change → preterm injury
- Focal cortical dysplasia / polymicrogyria — abnormal cortical thickness and gyral pattern on FLAIR/T1
- Unilateral cortical/subcortical atrophy with ex-vacuo ventricular dilatation → remote infarct
- Restricted diffusion (DWI) → acute stroke in postnatal presentations
• MR angiography / venography — when vascular malformation, sinovenous thrombosis, or moyamoya is suspected.
Electroencephalogram (EEG):
• Indicated in all children with infantile hemiplegia to screen for subclinical epileptic activity and characterise seizure semiology.
• Focal or multifocal discharges over the lesional hemisphere are expected; independent bilateral discharges raise concern for bilateral disease.
• Video-EEG is essential for pre-surgical evaluation in drug-resistant epilepsy.
Developmental assessment:
• Formal developmental assessment using standardised tools (Developmental Assessment Scale for Indian Infants — DASII; Bayley Scales) to quantify cognitive, language, and adaptive function domains.
• Hearing and vision assessment are mandated given the frequency of sensory comorbidities.
Aetiological workup (based on history):
• Thrombophilia screen (protein C, protein S, factor V Leiden, antiphospholipid antibodies) — in arterial ischaemic stroke
• TORCH serology — if congenital infection suspected
• Metabolic screen (lactate, ammonia, organic acids) — MELAS, organic acidaemia
• Haemoglobin electrophoresis — sickle cell disease screening
• ECHO and ECG — if cardioembolic stroke suspected
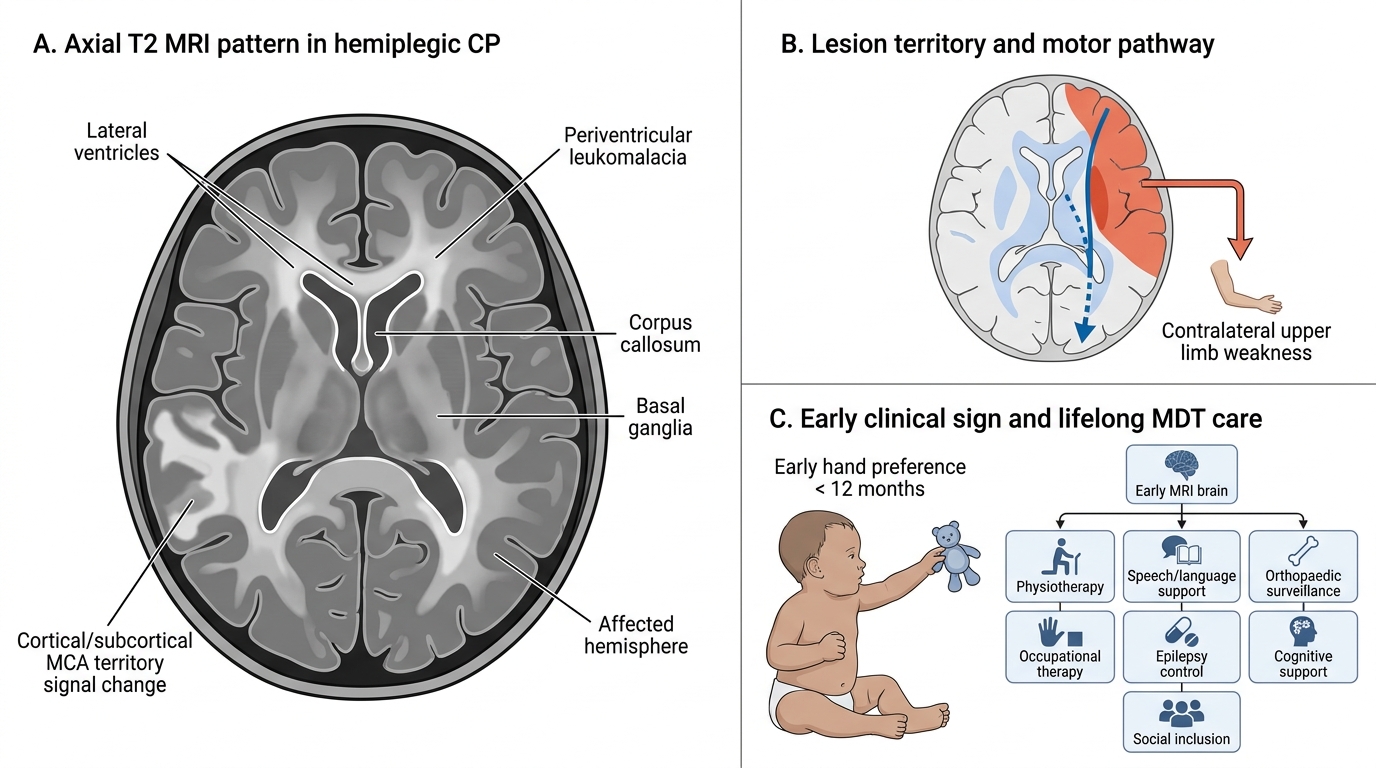
MRI Pattern and Clinical Clues in Hemiplegic Cerebral Palsy
CLINICAL PEARL
The single most sensitive early sign of infantile hemiplegia is hand preference before 12 months of age. Normally, children do not demonstrate consistent hand dominance until 18–24 months. Any infant who consistently favours one hand and keeps the other fisted should be presumed to have a contralateral brain lesion until proven otherwise. This 'early hand preference' sign is more sensitive than any single motor milestone and should prompt immediate neuroimaging (MRI brain). Do not wait for the child to fail multiple milestones before investigating — the window for early rehabilitation is narrow.
Management
Management of infantile hemiplegia requires a multidisciplinary team (MDT) approach and is lifelong in nature. The goals are: (1) maximise functional motor ability of the affected limb; (2) prevent secondary musculoskeletal complications; (3) control associated epilepsy; (4) support cognitive and language development; and (5) promote social inclusion and quality of life. Early referral — ideally in infancy — optimises outcomes by capitalising on the neuroplasticity window that is widest before age four to five years. No single therapy can address all domains; the MDT typically includes a paediatric neurologist or developmental paediatrician, physiotherapist, occupational therapist, speech-language therapist, orthopaedic surgeon, educational psychologist, and the child's family as active participants. Treatment decisions are guided by GMFCS level, seizure control, and the child's specific functional goals rather than a one-size-fits-all protocol.
Physiotherapy and occupational therapy (cornerstone of management):
• Early physiotherapy focuses on facilitation of normal movement patterns, stretching of spastic muscles, and prevention of contractures.
• Constraint-Induced Movement Therapy (CIMT): the unaffected arm is constrained (cast or mitt) for 2–6 hours daily over a 2-week intense programme, forcing use of the affected limb. CIMT is the most evidence-based intervention for improving upper-limb function in hemiplegic CP (GMFCS I–II, age 2–12 years). It works by enhancing corticospinal projections from the ipsilateral unaffected hemisphere.
• Goal-directed training and bimanual therapy (bilateral activities) are used as complementary approaches.
Spasticity management:
• Botulinum toxin A (BTA) injections into spastic upper-limb muscles (FCU, FCR, PT) and gastrocnemius (equinus) reduce tone and improve range of motion for 3–6 months, facilitating physiotherapy. Typically repeated every 4–6 months.
• Oral baclofen or tizanidine — for generalised spasticity; limited role in pure hemiplegia.
• Intrathecal baclofen (ITB) pump — reserved for severe spasticity affecting function and care (GMFCS IV–V).
• Selective dorsal rhizotomy (SDR) — for spastic diplegia primarily; rarely used in hemiplegia.
Epilepsy management:
• Anti-epileptic drugs (AEDs) are chosen based on seizure type (per ILAE classification). For focal onset seizures in hemiplegic CP: levetiracetam, carbamazepine, oxcarbazepine, or lacosamide are preferred. Valproate is used for mixed or generalised seizures.
• Carbamazepine must be avoided if there is a myoclonic component (worsens myoclonic seizures).
• Dosing is always weight-based (mg/kg) in children; regular therapeutic drug monitoring where applicable.
• Epilepsy surgery (hemispherotomy) — for drug-resistant epilepsy with a clear unilateral lesion (cortical dysplasia, porencephalic cyst) and concordant ictal EEG; the most effective intervention for achieving seizure freedom in selected cases, with minimal added neurological deficit in an already-hemiplegic hemisphere.
Orthopaedic interventions:
• Serial casting or ankle-foot orthoses (AFOs) — for equinus; worn during sleep and activity.
• Botulinum toxin + casting as first-line before surgical correction.
• Orthopaedic surgery — intramuscular lengthening of heel cord (Achilles tendon lengthening), derotation osteotomy for femoral anteversion, hip reconstruction for subluxation.
Cognitive and educational support:
• Early intervention programmes, learning support in school, and neuropsychological input for children with intellectual impairment.
• Speech-language therapy for expressive language and communication difficulties.
• Assistive technology (adapted keyboards, voice-to-text) for children with significant upper-limb dysfunction.
Family-centred care:
• Parents require counselling, education, and psychological support. Realistic goal-setting (GMFCS-based) helps families plan.
• Regular MDT reviews every 6–12 months with a paediatric neurologist, physiotherapist, occupational therapist, orthopaedic surgeon, and educational psychologist.
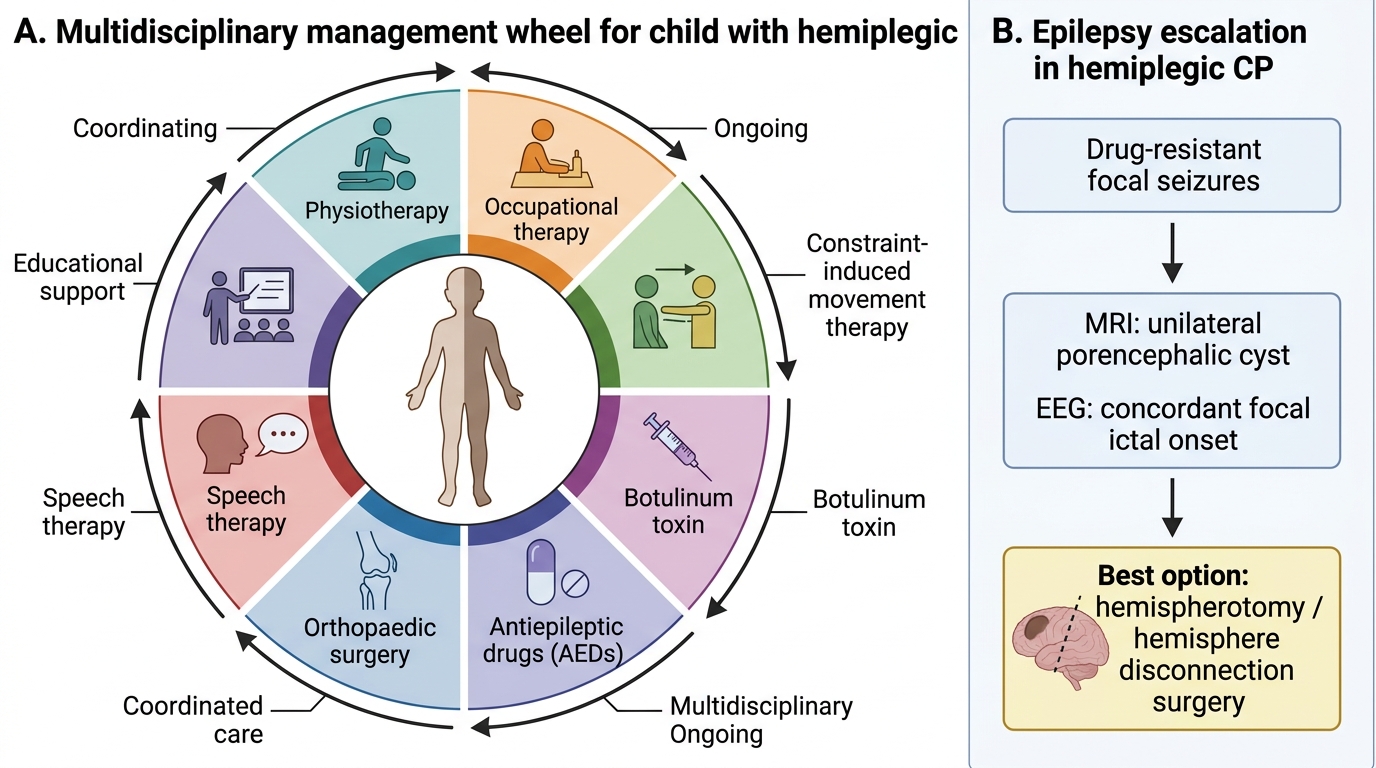
Multidisciplinary Management of Hemiplegic Cerebral Palsy
SELF-CHECK
A 3-year-old girl with right hemiplegic CP (GMFCS level II) has drug-resistant focal seizures despite two appropriate AEDs. MRI shows a right frontal porencephalic cyst from a perinatal MCA territory stroke. EEG shows right frontal ictal onset. The BEST treatment option for seizure freedom is:
A. Add a third AED (lacosamide)
B. Right hemisphere disconnection surgery (hemispherotomy)
C. Ketogenic diet
D. Vagus nerve stimulation
Reveal Answer
Answer: B. Right hemisphere disconnection surgery (hemispherotomy)
In a child with drug-resistant focal epilepsy, a clear unilateral structural lesion, and concordant ictal EEG, resective or disconnective epilepsy surgery (hemispherotomy/hemispherectomy) offers the highest rate of seizure freedom (~60–70%). Because the hemisphere is already non-functional (hemiplegia), disconnection adds no additional neurological deficit. A third AED is unlikely to provide seizure freedom (two AED failures define drug resistance). Ketogenic diet and VNS are palliative options with lower seizure-freedom rates, used when surgery is contraindicated or the family declines.
Self-Assessment
Test your understanding of infantile hemiplegia with the following case-based questions:
Case: An 8-month-old male infant is referred by a general practitioner. The mother noted at 5 months that he always reaches with his right hand and never uses his left. On examination: left arm held in flexion with fisted hand; left lower limb has mild increased tone and brisk reflexes; Babinski sign present on the left; right-sided examination normal. He sits with support. There is no family history of neurological illness; pregnancy and delivery were uncomplicated at term.
Q1. What is the MOST LIKELY diagnosis, and which anatomical hemisphere is injured?
Answer: Infantile hemiplegia (hemiplegic cerebral palsy) due to a right hemisphere lesion. The left-sided UMN signs (spasticity, hyperreflexia, Babinski, fisted posture) localise to a contralateral (right) corticospinal tract injury — in the motor cortex, subcortical white matter, or internal capsule.
Q2. List THREE prenatal and TWO perinatal causes of infantile hemiplegia.
Answer: Prenatal: (i) cerebral cortical dysplasia (focal polymicrogyria, schizencephaly); (ii) prenatal arterial ischaemic stroke (MCA territory); (iii) periventricular leukomalacia (white matter injury). Perinatal: (i) neonatal arterial ischaemic stroke (MCA — most common cause in term neonates); (ii) hypoxic-ischaemic encephalopathy with asymmetric cortical injury.
Q3. This child is assessed at 2 years of age and is walking independently with a mild limp and mild arm swing asymmetry; he can run on flat ground but has difficulty on stairs. What is his GMFCS level, and what is the most evidence-based intervention for his affected upper limb?
Answer: GMFCS level II (walks most settings; limitations on uneven terrain/stairs). The most evidence-based upper-limb intervention is Constraint-Induced Movement Therapy (CIMT) — constraining the unaffected right arm for several hours daily over an intensive course forces use of the affected left arm, exploiting ipsilateral corticospinal neuroplasticity.
Key summary points:
• Early hand preference (<12 months) is the hallmark sign — refer urgently for MRI brain.
• Classify CP by motor type (spastic/dyskinetic/ataxic) AND topography (hemiplegia/diplegia/quadriplegia).
• GMFCS I–V guides prognosis and rehabilitation goals — most hemiplegic CP is GMFCS I–III.
• Screen for epilepsy (35–40%), cognitive impairment, and visual/sensory deficits.
• Management = MDT (PT/OT/CIMT + botulinum toxin + AEDs + orthopaedic ± epilepsy surgery).