Page 28 of 48
PE27.9 | Intellectual Disability — SDL Guide
Learning Objectives
- Define intellectual disability using the DSM-5 framework and identify its core diagnostic criteria
- List the major aetiological categories of intellectual disability including genetic, perinatal, and postnatal causes
- Classify severity of intellectual disability by adaptive functioning across conceptual, social, and practical domains
- Outline the multidisciplinary assessment and management approach including early intervention principles
- Counsel families about prognosis, educational options, and community support services
INSTRUCTIONS
Intellectual disability (ID) is one of the most prevalent neurodevelopmental conditions encountered in paediatric practice, affecting approximately 1–3% of the global population. In India, the Rights of Persons with Disabilities Act 2016 recognises intellectual disability as a defined category deserving legal protection, educational entitlements, and welfare support. As a future clinician, your ability to identify early developmental red flags, conduct structured assessments, determine the underlying cause, and coordinate a multidisciplinary care plan directly impacts the child's long-term independence and quality of life. Early intervention — particularly before age 5 — can meaningfully improve adaptive functioning outcomes.
References
- Ghai Essential Pediatrics, 9th Edition, Ch. 18 (Developmental Paediatrics) (textbook)
- Nelson Textbook of Pediatrics, 21st Edition, Ch. 54 (Intellectual Disability) (textbook)
- DSM-5, American Psychiatric Association — Neurodevelopmental Disorders (guideline)
- Rights of Persons with Disabilities Act, 2016 (RPWD Act) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Ravi is a 5-year-old boy brought by his parents with the complaint that he is 'not like other children his age.' He does not yet speak in sentences, cannot dress himself, has difficulty following two-step instructions, and has never attended nursery school because the teachers said he 'could not keep up.' His parents, both labourers, did not seek help earlier, assuming he was a 'late developer.' On examination, his weight is appropriate for age, he makes eye contact and is affectionate. He can name familiar objects but speaks in single words only. He cannot draw a circle or copy simple shapes. The paediatrician suspects a neurodevelopmental disorder. What is the likely diagnosis, what tests would you order, and how would you explain this to his family?
WHY THIS MATTERS
Intellectual disability affects approximately 1–3% of children worldwide, with higher prevalence in low-resource settings where preventable causes such as perinatal asphyxia, iodine deficiency, and postnatal infections are more common. India's burden of ID is substantial, with millions of children requiring special education, rehabilitation, and family support. The condition spans a lifelong trajectory — early recognition and intervention in the first five years of life are the most powerful determinants of eventual adaptive functioning. Clinicians who can identify developmental red flags, perform structured assessments, recognise treatable causes, and coordinate multidisciplinary care directly improve the child's trajectory. Furthermore, legal frameworks including the RPWD Act 2016 place obligations on healthcare providers to certify disability and facilitate access to educational and welfare entitlements.
RECALL
Before proceeding, consolidate your prior knowledge on the following:
• Normal developmental milestones — social smile ~6–8 weeks; neck control ~3 months; sitting without support ~6–8 months; walking alone ~12–15 months; 2-word phrases ~18–24 months. These are the reference points against which developmental delay is identified.
• Domains of development — gross motor, fine motor, language/speech, social/adaptive — a child can be delayed in one or all domains.
• Chromosomal syndromes — Down syndrome (trisomy 21) is the commonest chromosomal cause; Fragile X syndrome is the commonest inherited cause of ID.
• Bayley Scales and DASII — Developmental Assessment Scales for Indian Infants (DASII) and the Vineland Adaptive Behaviour Scales are the standard Indian tools for early developmental assessment.
• IQ testing — standardised intelligence tests (Wechsler, Stanford-Binet, Binet-Kamat for India) measure cognitive ability; however, DSM-5 requires BOTH cognitive AND adaptive behaviour deficits for the diagnosis of ID.
Clinical Presentation: Recognising Intellectual Disability
Intellectual disability (ID) is defined by the DSM-5 as a neurodevelopmental disorder characterised by significant deficits in BOTH intellectual functions (reasoning, abstract thinking, academic learning, problem-solving) AND adaptive behaviour (the conceptual, social, and practical skills needed for day-to-day functioning), with onset during the developmental period (before 18 years of age). This dual-criterion definition is clinically critical: a child with a low IQ score but fully intact adaptive functioning does NOT meet DSM-5 criteria, and conversely, a child with severe adaptive limitations may meet criteria even if formal IQ testing is unreliable.
In clinical practice, ID most commonly comes to attention through developmental surveillance. Parents may report the child is 'slow,' not speaking like peers, unable to follow instructions, or failing to acquire self-care skills such as feeding, dressing, or toileting at the expected age. Teachers may flag that the child cannot cope with classroom learning. The paediatrician's first task is to document which developmental domains are affected, for how long, and whether there are any associated neurological or dysmorphic features.
Common presenting features across age groups:
• Infancy: failure to achieve developmental milestones (head holding, sitting, babbling), poor visual tracking, hypotonia, abnormal cry.
• Toddler and preschool: delayed speech, poor play skills, inability to follow commands, limited curiosity about environment.
• School age: academic failure, inability to read or write, difficulty with peer relationships, behavioural problems (aggression, self-injury).
• Associated features: epilepsy (in up to 30% of children with ID), autism spectrum features, sensory impairments (vision, hearing), behavioural and psychiatric comorbidities, physical anomalies (particularly with chromosomal syndromes).
Dysmorphic features suggesting a specific syndrome: Down syndrome — upslanting palpebral fissures, epicanthic folds, flat nasal bridge, single palmar crease, short stature, atlantoaxial instability. Fragile X — large head, prominent ears, long face, macro-orchidism post-puberty. Prader-Willi — hypotonia, hyperphagia, hypogonadism. Turner syndrome (in girls) — webbed neck, short stature, wide carrying angle. Recognition of a syndrome guides investigations and genetic counselling.
Aetiological Classification of Intellectual Disability
Aetiology and Pathogenesis
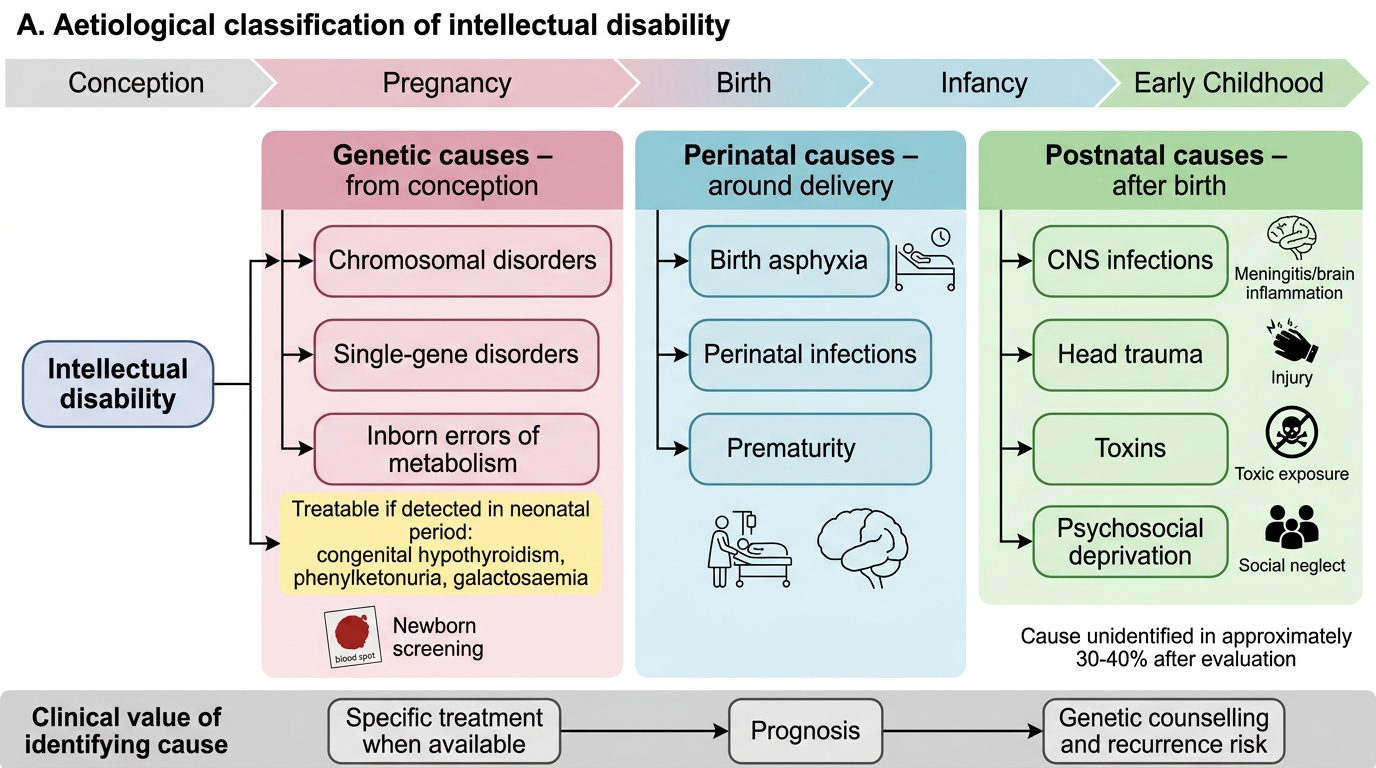
The causes of intellectual disability are heterogeneous and may act at any point from conception through early childhood. A systematic aetiological classification helps identify the underlying cause, which is essential for genetic counselling, prognostication, and in some cases, specific treatment. Crucially, a subset of ID causes are amenable to treatment — congenital hypothyroidism, phenylketonuria, and galactosaemia can be fully prevented if identified and treated within the neonatal period, making newborn screening programmes a vital public health tool. Even where no treatment exists, establishing the aetiology guides recurrence-risk counselling for future pregnancies and helps families understand the child's developmental trajectory. Clinically, causes are grouped by timing of the insult — genetic or chromosomal (from conception), prenatal environmental (acting on the developing fetus during organogenesis), perinatal (around the time of delivery), and postnatal (acting on the child's developing brain after birth). In approximately 30–40% of thoroughly evaluated cases, a specific cause is not identified, a proportion that is even higher in resource-limited settings with restricted access to advanced genetic testing.
1. Genetic and chromosomal causes (pre-conceptional/prenatal):
• Chromosomal: Down syndrome (trisomy 21 — nondisjunction 95%, translocation 4%, mosaic 1%), Edwards syndrome (trisomy 18), Patau syndrome (trisomy 13), Turner (45,XO), Klinefelter (47,XXY), deletions and duplications (22q11, Angelman, Prader-Willi).
• Single-gene disorders: Fragile X syndrome (FMR1 gene — triplet repeat CGG expansion; X-linked), Phenylketonuria (PKU — autosomal recessive, phenylalanine hydroxylase deficiency), homocystinuria, maple syrup urine disease, galactosaemia, hypothyroidism (if untreated; congenital hypothyroidism is treatable and included on newborn screening).
• Neurocutaneous syndromes: tuberous sclerosis, neurofibromatosis type 1.
2. Prenatal environmental causes:
• Infections: TORCH (toxoplasmosis, rubella, CMV, herpes) — particularly rubella is a vaccine-preventable cause; congenital Zika.
• Toxins: alcohol (fetal alcohol syndrome — leading preventable cause in many populations); lead, mercury exposure.
• Nutritional: maternal iodine deficiency (endemic cretinism — preventable with iodised salt); folic acid deficiency (neural tube defects).
• Radiation, hypoxia: placental insufficiency, maternal anaemia, toxaemia.
3. Perinatal causes:
• Birth asphyxia (hypoxic-ischaemic encephalopathy, HIE) — one of the most important and common causes in India; grades I–III (Sarnat classification); grade III HIE carries high risk of severe ID, cerebral palsy, epilepsy.
• Prematurity and low birth weight — intraventricular haemorrhage, periventricular leukomalacia.
• Neonatal hypoglycaemia, hyperbilirubinaemia (kernicterus) — both treatable causes; prevention emphasises newborn monitoring.
• Neonatal meningitis — GBS, Listeria, gram-negative organisms.
4. Postnatal causes:
• CNS infections: bacterial meningitis, encephalitis (measles encephalitis — vaccine-preventable), Japanese encephalitis, cerebral malaria.
• Trauma: non-accidental head injury (child abuse), road traffic accidents.
• Toxins: lead poisoning (pica, old paint, utensils), mercury.
• Psychosocial deprivation: extreme neglect, environmental deprivation — particularly severe in institutional settings; responds to enriched environments.
• Epilepsy: recurrent severe seizures (status epilepticus) can cause progressive intellectual decline.
Pathogenesis: The brain's vulnerability depends on the timing and nature of the insult. Prenatal insults (especially in the first trimester) disrupt neuronal proliferation and migration, producing structural malformations. Perinatal hypoxia causes selective necrosis in metabolically active areas (basal ganglia, hippocampus, cortex). Postnatal infections and toxins affect myelination and synaptic connectivity. In chromosomal syndromes, gene-dosage effects alter neurodevelopmental signalling pathways from conception.
Diagnosis and Assessment
The diagnosis of intellectual disability requires a structured, multidisciplinary evaluation encompassing history, developmental assessment, neurological examination, investigations, and formal psychometric testing. The DSM-5 requires deficits in BOTH intellectual function AND adaptive behaviour, confirmed by clinical assessment and standardised testing. Clinicians must approach assessment systematically: first establishing that global developmental delay is present (distinguishing from isolated language or motor delay), then determining severity across the three adaptive behaviour domains, and finally pursuing aetiological investigations guided by clinical findings. It is equally important to assess for comorbidities — epilepsy, sensory impairments, autism spectrum features, and psychiatric disorders — that substantially affect management and prognosis. A thorough birth and developmental history frequently points to the cause, and in many resource-limited settings, careful clinical assessment and targeted investigations yield the aetiology without expensive genomic panels.
Provided image
History taking — key points:
• Birth history: antenatal events, gestational age, delivery mode, APGAR scores, need for resuscitation, postnatal complications (hypoglycaemia, jaundice, infections).
• Developmental history: milestones in all four domains, any regression (suggests a metabolic or degenerative disorder).
• Family history: consanguinity (raises suspicion of autosomal recessive metabolic disorders), other affected members, parental cognitive level.
• Social history: school attendance, academic performance, home environment, any exposure to toxins or deprivation.
Physical and neurological examination:
• Growth parameters: head circumference (microcephaly — TORCH, structural; macrocephaly — hydrocephalus, Fragile X, Sotos); height and weight.
• Dysmorphic features suggesting a specific syndrome.
• Neurological examination: tone (hypotonia vs hypertonia), reflexes, coordination, vision, hearing.
• Skin: neurocutaneous markers (ash-leaf macules — tuberous sclerosis; café-au-lait spots — NF1).
Developmental and psychometric assessment:
• DASII (Developmental Assessment Scales for Indian Infants): norm-referenced tool for 0–30 months, assessing motor and mental development quotients.
• Vineland Adaptive Behaviour Scales (VABS): evaluates communication, daily living skills, socialisation, and motor skills; norm-referenced on age; essential for DSM-5 adaptive behaviour criterion.
• Binet-Kamat Test (BKT): Indian standardisation of the Stanford-Binet; used for IQ measurement in Indian children.
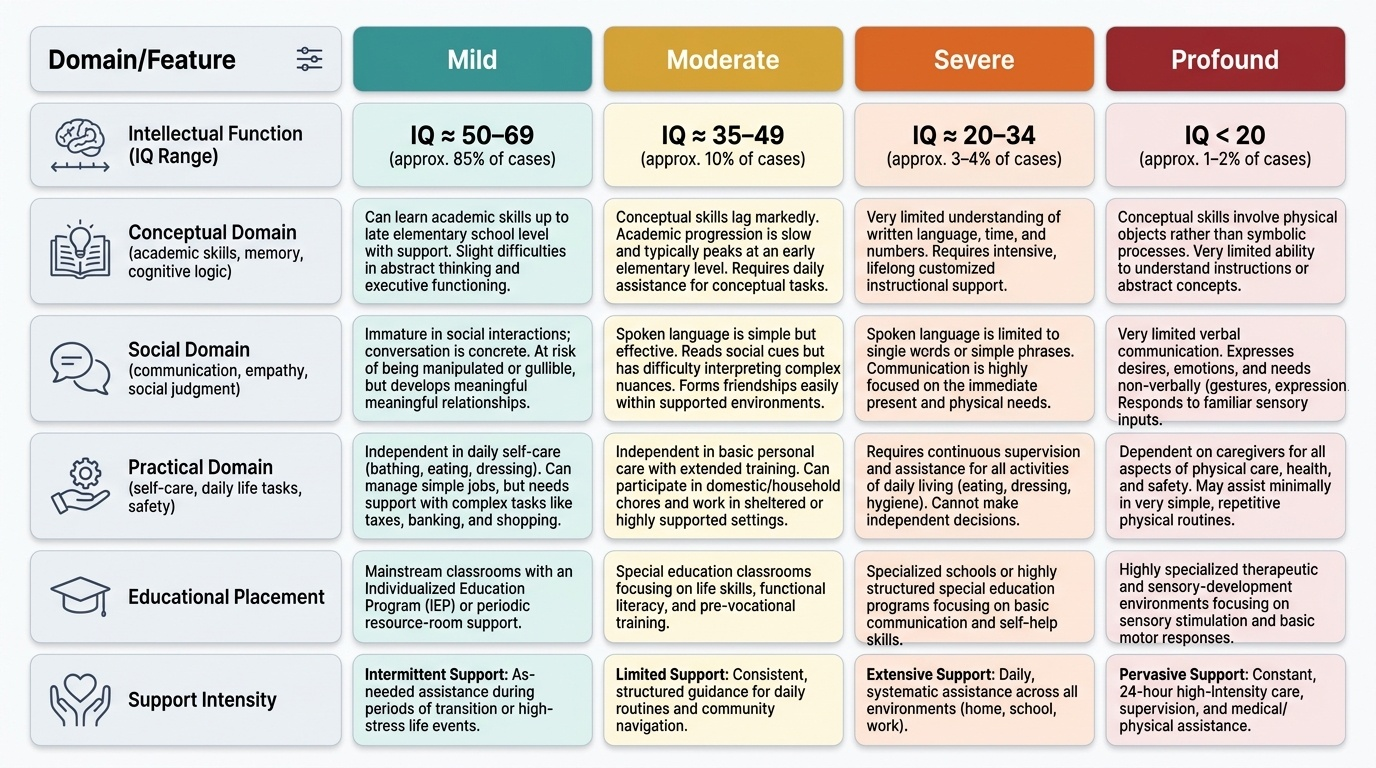
• IQ interpretation (supportive, not sole criterion): Mild 50–69, Moderate 35–49, Severe 20–34, Profound <20. IQ below 70 is a threshold, but severity classification per DSM-5 is based on ADAPTIVE FUNCTION across three domains: conceptual (academic, language, memory), social (empathy, communication, social judgement), practical (self-care, money management, task organisation).
Investigations — directed by history and examination:
• Thyroid function tests (T4, TSH): congenital hypothyroidism — treatable cause.
• Metabolic screen: serum amino acids, urine organic acids (if metabolic cause suspected — regression, acute illness, family history).
• Karyotype: for dysmorphic features suggesting chromosomal syndrome; FISH/microarray for microdeletion syndromes.
• FMR1 mutation testing: if Fragile X suspected (boy with family history, behaviour, physical features).
• Neuroimaging (MRI brain): if structural brain malformation, intractable epilepsy, or neurological signs; not routinely for all ID.
• EEG: if clinical seizures or paroxysmal events.
• Vision and hearing assessment: essential — uncorrected sensory deficits can mimic or aggravate ID.
• TORCH serology: if congenital infection suspected (microcephaly, chorioretinitis, calcifications).
• Lead levels: if pica or environmental exposure.
SELF-CHECK
A 6-year-old child has an IQ of 58 on the Binet-Kamat Test. He can feed himself, dress with minimal assistance, and plays with peers, though he needs support for complex instructions. According to DSM-5, how should this child's intellectual disability be classified?
A. Borderline intellectual functioning — IQ of 58 is too high for ID
B. Mild intellectual disability — adaptive function shows limited deficits with support
C. Moderate intellectual disability — IQ of 58 places him in the moderate range
D. Severe intellectual disability — school-age children with any ID are classified as severe
Reveal Answer
Answer: B. Mild intellectual disability — adaptive function shows limited deficits with support
DSM-5 classifies ID severity by ADAPTIVE FUNCTIONING, not IQ alone. IQ < 70 confirms significant intellectual deficit. This child's adaptive behaviour shows mild impairment — he can self-care and interact socially with support — which maps to MILD ID. Moderate ID is characterised by more substantial adaptive deficits (needs support for most daily living activities). IQ of 58 does not place him in borderline (IQ 70–85) or severe (IQ 20–34) range.