Page 29 of 48
PE27.9 | Intellectual Disability — SDL Guide (Part 2)
Management and Early Intervention
Management of intellectual disability is multidisciplinary, lifelong, and family-centred. There is no pharmacological cure for ID as a neurodevelopmental condition, but early intervention, targeted therapies, educational placement, and systematic treatment of comorbidities can substantially improve adaptive functioning and quality of life. The overarching goal shifts from eliminating the condition — which is not achievable in most cases — to maximising the child's functional independence and participation in society. The most important single principle is that early intervention before age 5 years yields the greatest developmental gains, because this period coincides with the brain's maximum neuroplasticity, the biological window during which guided experience most powerfully shapes neural architecture. Starting intervention at diagnosis — even in infancy — and maintaining it through school entry is therefore paramount. A second overarching principle is the family-centred care model: parents and caregivers are the child's primary rehabilitation providers in the home environment, and equipping them with skills, knowledge, and psychosocial support is as important as the direct therapy sessions delivered by professionals.
1. Treating the underlying cause where possible:
• Congenital hypothyroidism: thyroxine replacement — if started within the first 2 weeks, normal IQ can be achieved. This underscores the importance of neonatal screening.
• Phenylketonuria (PKU): low-phenylalanine diet from the neonatal period prevents ID.
• Galactosaemia, MSUD: dietary restriction.
• Hydrocephalus: surgical shunting.
• Lead poisoning: chelation therapy + source removal.
• Iodine deficiency: iodised salt at population level; potassium iodide supplements in pregnancy in deficient areas.
2. Early Intervention Programme (EIP):
Early intervention encompasses structured programmes targeting all developmental domains, typically from the time of diagnosis (even in infancy). Components include:
• Physiotherapy: for motor delay, hypotonia, to achieve gross motor milestones.
• Occupational therapy (OT): fine motor skills, sensory integration, activities of daily living (ADL).
• Speech and language therapy (SLT): for language and communication delays; augmentative and alternative communication (AAC) for non-verbal children.
• Special education: structured individualised education plans (IEPs); India's RPWD Act 2016 mandates inclusive education with appropriate support.
• Behavioural therapy (Applied Behaviour Analysis — ABA): for managing maladaptive behaviours, social skill training.
3. Management of comorbidities:
• Epilepsy (30% of children with ID): appropriate anticonvulsant therapy (valproate, carbamazepine, levetiracetam — weight-based dosing; never adult fixed dose).
• Psychiatric comorbidities: ADHD, autism spectrum disorder, anxiety, depression — screen and treat.
• Sensory impairments: hearing aids, glasses — correct correctable deficits that worsen functioning.
• Nutritional support: many children with ID have feeding difficulties; dietitian involvement.
4. Family counselling and support:
• Explanation of diagnosis: honest, compassionate communication; avoid prognostic pessimism; emphasise what the child CAN do and what intervention can achieve.
• Genetic counselling: for chromosomal/single-gene causes — recurrence risk, prenatal diagnosis options.
• Caregiver wellbeing: caregiver burnout is high; refer to parent support groups (National Trust, Asha Support Groups).
• Legal entitlements under RPWD Act 2016: disability certificate, educational support, welfare schemes (CBR — Community-Based Rehabilitation).
5. Educational placement:
• Mild ID: inclusive mainstream education with support (IEP, resource room).
• Moderate ID: special schools with vocational training emphasis.
• Severe/profound ID: intensive day care and residential support; focus on self-care and basic life skills.
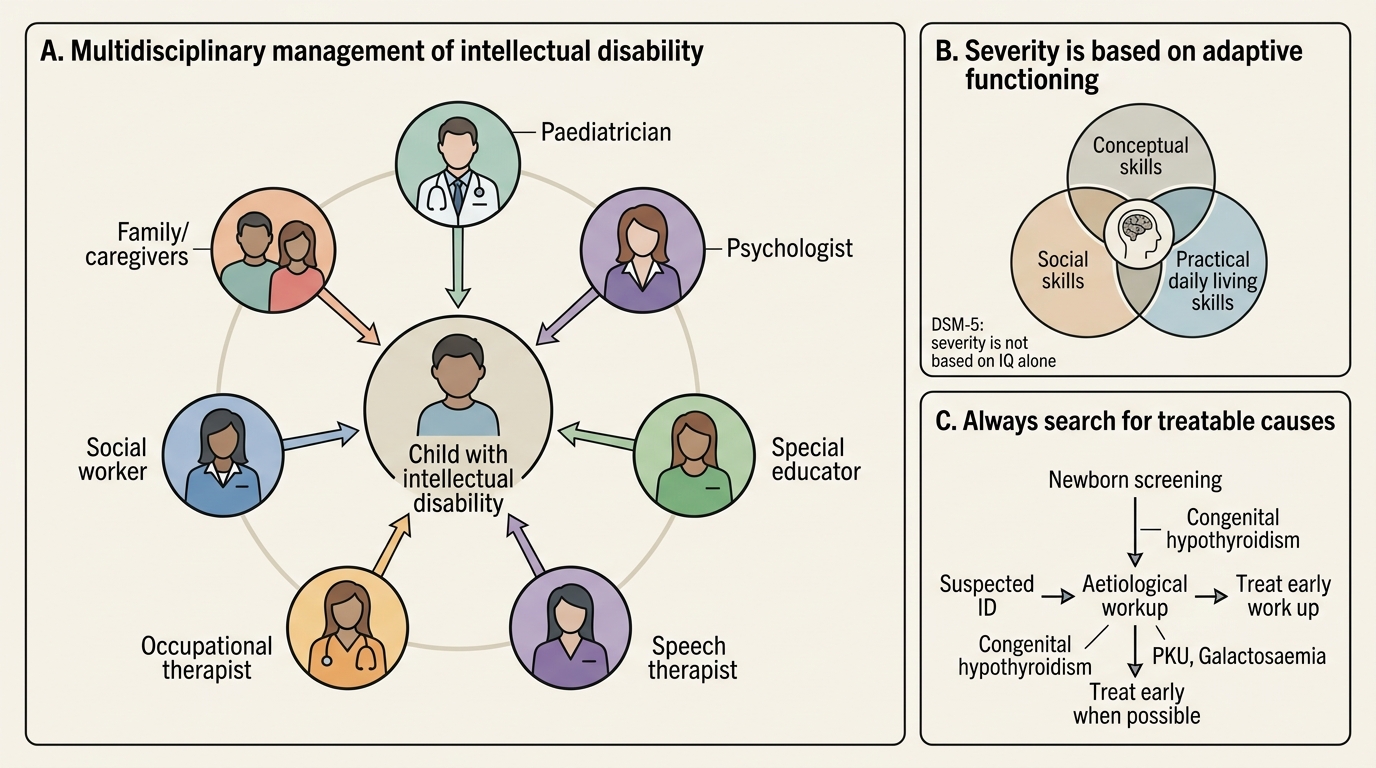
Multidisciplinary Management of Intellectual Disability
CLINICAL PEARL
The single most important clinical trap in intellectual disability is relying on IQ alone for diagnosis and severity classification. DSM-5 explicitly states that severity is determined by ADAPTIVE FUNCTIONING — not IQ score — across the conceptual, social, and practical domains. A child with an IQ of 60 who is fully independent in daily living, communicates effectively, and maintains peer friendships may not meet criteria for moderate ID, whereas a child with an IQ of 65 but severe adaptive deficits does. Always assess all three adaptive behaviour domains using a validated scale (Vineland Adaptive Behaviour Scales) and correlate with IQ. A second critical point: ALWAYS look for a treatable cause — congenital hypothyroidism, PKU, and galactosaemia are entirely preventable causes of ID if detected and treated on newborn screening. Every case of ID deserves a systematic aetiological workup.
SELF-CHECK
A 3-year-old girl with trisomy 21 (Down syndrome) is brought for a routine developmental assessment. Her parents ask whether early intervention will 'make a difference.' Which statement is most accurate regarding early intervention in intellectual disability?
A. Early intervention has no proven benefit in chromosomal causes of ID such as Down syndrome
B. Early intervention is most beneficial if started after formal schooling at age 5–6 years
C. Early intervention before age 5 years exploits neuroplasticity and can significantly improve adaptive functioning
D. Early intervention is indicated only for mild ID; it has no role in moderate or severe ID
Reveal Answer
Answer: C. Early intervention before age 5 years exploits neuroplasticity and can significantly improve adaptive functioning
Early intervention (physiotherapy, speech therapy, OT, special education) works by exploiting maximum neuroplasticity in the first five years of life, improving adaptive functioning outcomes even in chromosomal causes like Down syndrome. Multiple studies and guidelines (including WHO/IAP) support early intervention across all severity levels of ID. Starting after age 5–6 misses the critical developmental window. Early intervention benefits mild, moderate, and severe ID — with the most intensive programmes for more severe forms.
Self-Assessment: Intellectual Disability
Use these case vignettes and concept questions to test your understanding of intellectual disability before your next clinical encounter or examination. Self-assessment at this stage consolidates the SDL arc: from recognising the clinical presentation, to building an aetiological differential, to planning a structured diagnostic workup, and finally to counselling a family and coordinating multidisciplinary intervention. Attempt each question independently before reading the suggested answers, and use the "Key concepts" list as a final revision checklist to ensure you have retained the core framework for approaching intellectual disability in clinical practice.
Case vignette 1: A 7-year-old boy with upslanting palpebral fissures, a single palmar crease, a flat nasal bridge, and generalised hypotonia has never attended school. On DASII assessment his developmental quotient is significantly below age norms. His mother is 38 years old. Questions:
1. What is the most likely diagnosis and its chromosomal basis?
2. What associated conditions should you screen for (cardiac, ophthalmological, thyroid, atlantoaxial)?
3. What legal entitlements is this child eligible for under the RPWD Act 2016?
Case vignette 2: A 4-year-old girl presents with language delay, self-injurious behaviour, and a seizure disorder. Her MRI shows periventricular leukomalacia. Her mother had a difficult delivery with prolonged second stage. Questions:
1. What is the most likely cause of her intellectual disability?
2. How would you classify her severity using adaptive behaviour?
3. What early intervention services would you recommend?
Key concepts to consolidate:
• DSM-5 criteria: deficits in intellectual function + adaptive behaviour, onset in developmental period.
• Severity classification by adaptive functioning (NOT IQ alone): mild (IQ 50–69) → moderate (35–49) → severe (20–34) → profound (<20).
• Three domains of adaptive behaviour: conceptual (language, reading, reasoning), social (empathy, communication, social judgement), practical (self-care, organisation, money).
• Treatable causes to always exclude: congenital hypothyroidism, PKU, galactosaemia, lead poisoning, hydrocephalus.
• Early intervention before age 5 is the most impactful intervention window.
• MDT: paediatrician, psychologist, special educator, speech therapist, OT, social worker, family.