Page 5 of 48
PE27.2 | Tuberculous Meningitis — SDL Guide
Learning Objectives
- Describe the subacute clinical presentation and staging (I/II/III) of tuberculous meningitis
- Explain the pathogenesis of TBM from primary pulmonary focus to basal meningeal inflammation
- Interpret the characteristic CSF profile of TBM and distinguish it from bacterial and viral meningitis
- Outline the NTEP ATT regimen for TBM including the extended duration and adjunctive dexamethasone
- Identify the major complications of TBM and describe preventive strategies
INSTRUCTIONS
Tuberculous meningitis (TBM) is the most severe and potentially fatal form of extrapulmonary tuberculosis in children. India carries more than a quarter of the world's TB burden, and TBM remains a significant cause of childhood morbidity and long-term neurological disability in our setting. Unlike bacterial meningitis, TBM presents insidiously over days to weeks, making early recognition genuinely challenging. The clinical stage at which treatment begins is the single strongest predictor of outcome — outcomes in Stage I are good; by Stage III, death and severe disability are common. This module gives you the tools to recognise TBM early, interpret the diagnostic tests correctly, and prescribe the right regimen for the right duration.
References
- Ghai Essential Pediatrics, 9th ed., Ch 17 (CNS Infections — Tuberculous Meningitis) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 215 (Tuberculosis) (textbook)
- National TB Elimination Programme (NTEP) Treatment Guidelines (current edition) (guideline)
- IAP Guidelines on Childhood Tuberculosis (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old girl is brought to the paediatric OPD with a 3-week history of gradually worsening headache, low-grade fever, and increasing irritability. Over the past 3 days she has vomited twice daily and seems confused. Her mother mentions that the family's grandfather was treated for tuberculosis 6 months ago but she does not know if the child received any chemoprophylaxis. On examination: febrile 37.8°C, neck stiffness present, left lateral rectus palsy (CN VI), no papilloedema. Mantoux test is 12 mm. CSF shows 120 cells/mm³ (90% lymphocytes), protein 280 mg/dL, glucose 22 mg/dL (serum 85 mg/dL). What stage is this child's TBM, and what treatment must be started today?
WHY THIS MATTERS
India has the highest TB burden in the world, and children account for roughly 10–15% of all TB cases in the country. Tuberculous meningitis, while less common than pulmonary TB, carries the worst prognosis of any TB form — even with optimal treatment, 10–30% of children die and 20–30% of survivors have permanent neurological deficits. The key prognostic factor is not the potency of the drugs but the clinical stage at which treatment begins. A child treated in Stage I has an excellent chance of full recovery; the same child reaching Stage III before diagnosis faces likely death or severe disability. For you as a clinician in India, where TB contact is ubiquitous, recognising TBM early — especially in children with a subacute febrile illness and any neurological sign — is one of the highest-yield diagnostic skills you can develop.
RECALL
Before proceeding, recall the following:
• Mycobacterium tuberculosis (from MI): acid-fast bacillus, slow-growing (culture takes 4–8 weeks); detected on Ziehl-Neelsen stain; BCG = live attenuated vaccine from M. bovis.
• Primary tuberculosis (from MI/PY): Ghon focus (subpleural lung) + hilar lymph node = Ghon complex; subsequent haematogenous spread seeds organs including the CNS.
• Normal CSF (from PY): WBC <5/mm³ (lymphocytes), protein 15–45 mg/dL, glucose 60–70% of serum; clear and colourless.
• NTEP regimen notation: H = isoniazid, R = rifampicin, Z = pyrazinamide, E = ethambutol, S = streptomycin; prefix = months, e.g. 2HRZE = 2 months of all four drugs.
• Contrast with bacterial meningitis: bacterial meningitis is acute (hours–days) with neutrophilic CSF; TBM is subacute (weeks) with lymphocytic CSF.
Clinical Presentation and Staging of TBM
The hallmark of tuberculous meningitis that distinguishes it from bacterial meningitis is its subacute onset — symptoms typically evolve over 1–6 weeks rather than hours. This insidious progression reflects the nature of the underlying pathology: slowly expanding granulomatous inflammation at the base of the brain, rather than the explosive cytokine storm of pyogenic meningitis. Recognising this subacute temporal profile is the first and most important step in suspecting TBM before any laboratory results are available.
The clinical prodrome of TBM lasts 1–2 weeks and consists of non-specific constitutional symptoms: low-grade fever, headache, malaise, loss of appetite, and behavioural change or irritability in young children. In infants, the presentation may be even less specific — vomiting, poor feeding, and irritability without any clear meningeal signs. Many of these children have been assessed and dismissed as having a viral illness or poor appetite before the diagnosis is made.
As inflammation progresses to involve the meninges and the cranial nerves traversing the subarachnoid space, more specific neurological signs emerge:
• Meningism (neck stiffness, Kernig's sign, Brudzinski's sign) — indicates established meningeal inflammation
• Cranial nerve palsies — CN VI (abducens) is most commonly affected (lateral rectus palsy → convergent squint); CN III, VII also affected; result from compression by basal exudate
• Altered consciousness — from mild confusion to stupor
• Seizures — focal or generalised, reflecting cortical irritation or infarction
• Signs of raised ICP — headache, vomiting, papilloedema, Cushing's triad — from communicating hydrocephalus
The British Medical Research Council (MRC) staging system for TBM:
This staging system is critical because it directly determines prognosis and guides intensity of monitoring:
| Stage | Consciousness | Neurological deficit |
|---|---|---|
| Stage I | Alert, oriented | No focal deficit, no cranial nerve palsy, no hydrocephalus |
| Stage II | Confused or drowsy | Mild to moderate focal deficit or cranial nerve palsy |
| Stage III | Stuporous or comatose | Dense hemiplegia, paraplegia, or multiple cranial nerve palsies |
Stage at diagnosis is the single strongest predictor of outcome: Stage I survivors have ~90% chance of full recovery; Stage III mortality is 30–50% with permanent deficits in most survivors.
Pathogenesis of Tuberculous Meningitis
Pathophysiology and Aetiology of TBM
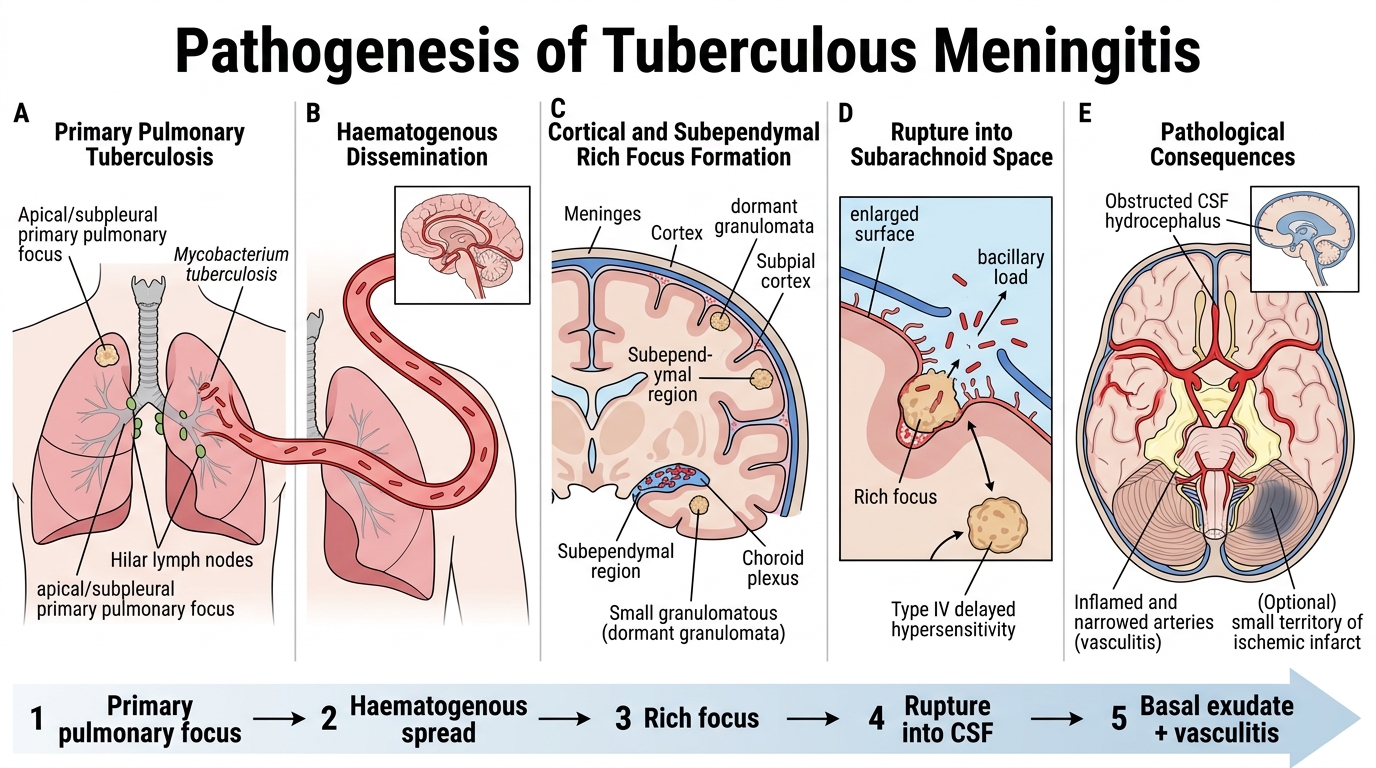
Tuberculous meningitis is caused exclusively by Mycobacterium tuberculosis in most cases (rarely M. bovis from unpasteurised milk). The pathogenesis follows a characteristic two-stage sequence that explains both the typical patient history of preceding TB exposure or pulmonary disease and the particular pattern of injury seen in TBM — basal predominance, hydrocephalus, and vasculitis.
Stage 1 — Haematogenous seeding and Rich focus formation: Following primary pulmonary infection, M. tuberculosis enters the bloodstream during the phase of haematogenous dissemination (part of primary complex spread). The organisms seed multiple organs simultaneously, including the subependymal or subpial regions of the brain cortex and choroid plexus. Here, granulomata form and lie dormant for weeks to years as Rich foci (first described by Arnold Rich, 1933). These cortical and subependymal granulomata are asymptomatic during this stage.
Stage 2 — Rupture into the subarachnoid space: When a Rich focus ruptures — triggered by declining immunity, malnutrition, or intercurrent illness — a large bacillary load is released into the CSF. The intense hypersensitivity reaction (Type IV delayed hypersensitivity) that follows produces the pathological hallmarks of TBM:
• Thick gelatinous basal exudate — concentrates at the base of the brain (basal cisterns, around the midbrain and circle of Willis); responsible for cranial nerve palsies by compression and trapping
• Obliterative vasculitis — inflammation of perforating arteries supplying the basal ganglia and internal capsule → lacunar infarcts → focal neurological deficits
• Communicating hydrocephalus — basal exudate obstructs CSF flow in the basal cisterns and impairs resorption at the arachnoid granulations; the ventricles dilate
• Cerebral oedema — from BBB breakdown and local cytokine release
• Cortical granulomata (tuberculomata) — discrete granulomatous masses within brain parenchyma, visible on CT/MRI as ring-enhancing lesions
This basal-predominant pathology directly explains the clinical features: the cranial nerve palsies come from the exudate at the skull base; the hydrocephalus from cistern blockade; the focal deficits from vasculitic infarcts in the territories of the perforating arteries.
SELF-CHECK
A 6-year-old child with TBM presents with a 3-week history of headache and fever, is now confused and drowsy, and has a right facial nerve palsy. According to the MRC staging system, this child is:
A. Stage I — alert with no deficits
B. Stage II — confused with cranial nerve palsy
C. Stage III — comatose with hemiplegia
D. Unstaged — requires CT first
Reveal Answer
Answer: B. Stage II — confused with cranial nerve palsy
MRC Stage II TBM is defined by altered consciousness (confused or drowsy) OR the presence of focal neurological deficit or cranial nerve palsy. This child has both (confusion + cranial nerve VII palsy), placing her firmly in Stage II. Stage I requires the child to be alert and neurologically intact. Stage III requires stupor/coma or dense hemiplegia/paraplegia. Staging is clinical and should not be deferred for CT results.
Diagnosis: CSF, Imaging and Microbiological Tests
The diagnosis of TBM rests on the integration of clinical features, CSF analysis, neuroimaging, and supporting tests for tuberculosis. No single test provides both high sensitivity and high specificity for TBM — the GeneXpert detects only about 60–70% of confirmed CSF cases; ZN stain is positive in fewer than 40%; culture takes 4–8 weeks; and even the Mantoux is negative in up to half of children with TBM. You must therefore approach this diagnosis probabilistically: gather all available information, weight each finding appropriately, and start treatment when the clinical and CSF picture is consistent even before molecular confirmation arrives. The clinician who waits for a definitive culture result before starting ATT will watch a Stage I patient progress to Stage II or III during that wait — an entirely preventable deterioration. This section gives you the framework to synthesise the diagnostic data correctly.
CSF analysis in TBM:
The CSF profile of TBM is distinct from both bacterial and viral meningitis, though there is overlap in early or treated cases:
• Appearance: typically clear or faintly turbid (not purulent as in bacterial meningitis); may show a characteristic cobweb clot when the tube is left to stand, caused by very high fibrinogen precipitating in a fine web pattern — this is highly suggestive of TBM
• Opening pressure: elevated (>20 cmH₂O) due to hydrocephalus
• Cell count: elevated, typically 100–500 cells/mm³, with >80% lymphocytes (lymphocytic pleocytosis) — distinguishes TBM from bacterial meningitis
• Protein: markedly elevated, often >100 mg/dL and sometimes >500 mg/dL — one of the highest protein levels in any meningitis
• Glucose: low, typically well below 40 mg/dL, often very low (<30 mg/dL); the CSF:serum glucose ratio is typically <0.4 and may be extremely low
Microbiological tests:
• CSF Ziehl-Neelsen (ZN) stain for AFB: sensitivity only 10–40%; a negative result does NOT exclude TBM
• CSF culture for M. tuberculosis: gold standard, sensitivity ~45–90% with large-volume culture; takes 4–8 weeks — too slow to guide initial treatment
• GeneXpert MTB/RIF (Xpert): NAAT-based; sensitivity ~60–70% on CSF (lower than sputum); specificity ~98%; detects rifampicin resistance; result in 2 hours — recommended by NTEP as first-line rapid test on CSF
• Mantoux test (TST): positive (≥10 mm in immunocompetent) supports TB exposure but is negative in 30–50% of TBM cases (due to immunosuppression from severe disease); a negative Mantoux does NOT exclude TBM
• IGRA (interferon-gamma release assay): more specific than Mantoux; but also has reduced sensitivity in severe TBM
Neuroimaging (CT or MRI brain):
CT with contrast is the practical first-line imaging in most Indian settings:
• Basal meningeal enhancement — thickened, bright enhancement of the basal cisterns (interpeduncular, suprasellar, sylvian) is the most characteristic CT finding in TBM
• Communicating hydrocephalus — enlarged ventricles, periventricular lucency (transependymal CSF seepage)
• Infarcts — in the distribution of perforating arteries (basal ganglia, internal capsule)
• Tuberculomata — ring-enhancing parenchymal lesions
MRI is more sensitive than CT, particularly for brainstem involvement and early ischaemia.
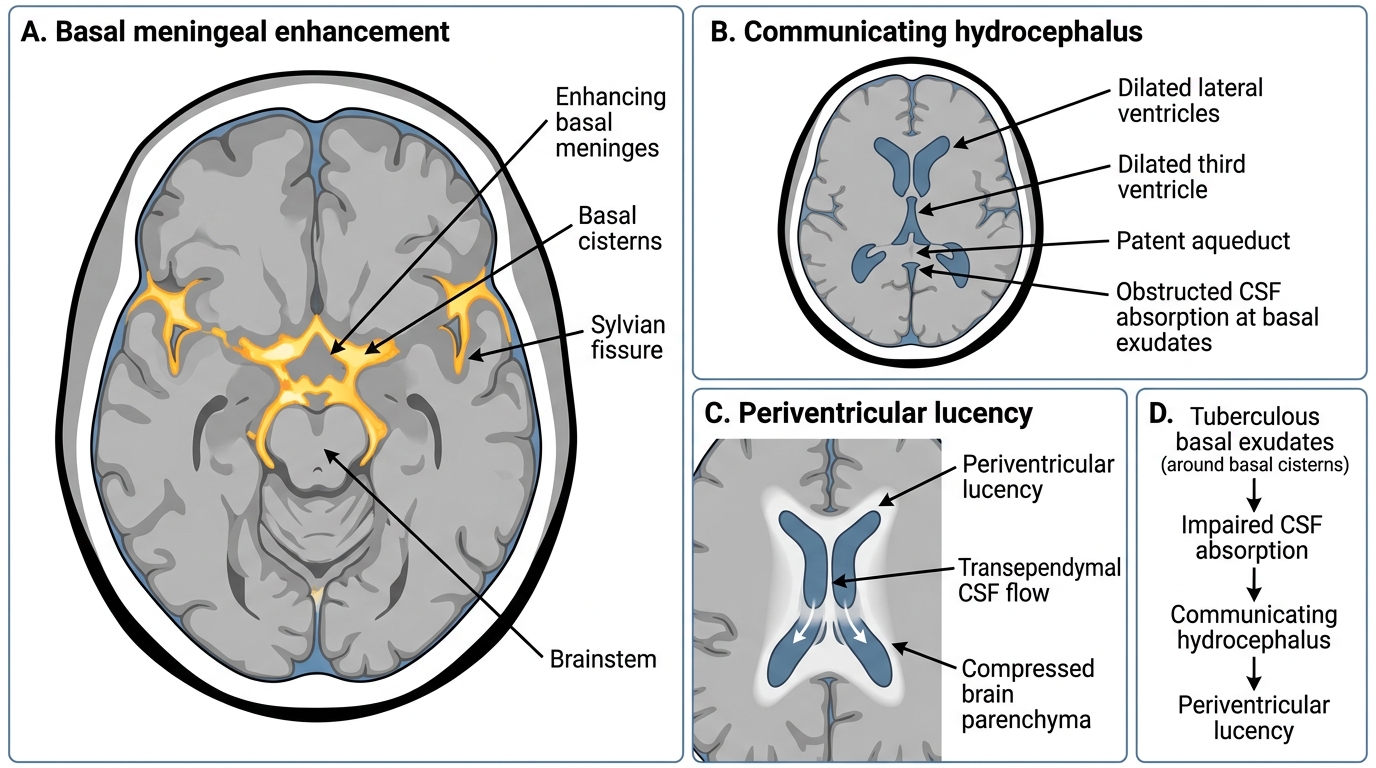
CT Findings in Tuberculous Meningitis