Page 6 of 48
PE27.2 | Tuberculous Meningitis — SDL Guide (Part 2)
Complications of TBM
The complications of TBM arise from three core pathological processes — the expanding basal exudate, obliterative vasculitis, and progressive hydrocephalus — and may develop during treatment as well as at presentation. Recognising and proactively managing complications is inseparable from antibiotic therapy and is the main determinant of long-term outcome in treated patients.
Hydrocephalus: The most common complication and a major driver of raised ICP in TBM. The communicating type (from basal cistern obstruction) is most frequent; occasionally an obstructive type occurs from tuberculoma at the aqueduct. Clinical features: bulging fontanelle in infants, declining level of consciousness, Cushing's triad, papilloedema, and sun-setting sign in infants (tonic downward eye deviation — discussed in the Hydrocephalus SDL). Management: treat the underlying TBM with ATT; dexamethasone reduces cerebral oedema; VP shunt or serial LPs may be needed for symptomatic communicating hydrocephalus not responding to medical management.
Cerebrovascular complications (stroke/vasculitis): Obliterative vasculitis of perforating arteries causes ischaemic infarcts in the basal ganglia, internal capsule, and thalamus. Presents as new focal neurological deficit (hemiplegia, cranial nerve palsy) during treatment — may be confused with treatment failure or paradoxical reaction.
Cranial nerve palsies: CN VI most commonly (lateral rectus palsy → convergent squint); CN III, VII affected as the basal exudate traps cranial nerve roots. Usually improve with effective ATT and steroids.
Seizures: Occur in 20–30% during the acute phase from cortical irritation, vasculitis, or hyponatraemia. Anti-epileptic drugs are required; important drug interaction note: phenytoin and carbamazepine are enzyme inducers and significantly reduce plasma rifampicin and isoniazid levels — prefer levetiracetam where available.
SIADH: Hyponatraemia from inappropriate ADH secretion; commonest electrolyte abnormality in TBM; treat with fluid restriction and correct sodium carefully.
Paradoxical reaction (immune reconstitution): Worsening of neurological symptoms or appearance of new tuberculomata 4–8 weeks after starting ATT, despite microbiological response. Caused by immune system reconstitution and enhanced inflammatory response to dying bacilli. Management: continue ATT, increase steroid dose.
Long-term sequelae: Intellectual disability and learning problems, epilepsy, spastic hemiplegia or diplegia, visual impairment (optic atrophy from chiasmal compression), and deafness.
CLINICAL PEARL
The cobweb clot is pathognomonic of TBM (when present): If you allow a tube of CSF to stand at room temperature for 30–60 minutes and observe a delicate fibrin web settling at the top or forming a clot — this is a cobweb clot. It is caused by the very high fibrinogen content of TBM CSF (which does not clot as fast as pus in bacterial meningitis). It is not always present but when seen it is highly specific for TBM. In resource-limited settings without immediate molecular diagnostics, this simple bedside observation can clinch the diagnosis. Teach yourself to observe the CSF tube — do not discard it after the sample is sent.
Management: ATT Regimen, Steroids and Supportive Care
Treatment of TBM requires starting anti-tuberculous therapy empirically as soon as the diagnosis is clinically and biochemically suspected — do not wait for culture or GeneXpert results. The core of management is the NTEP ATT regimen, which differs critically from the standard 6-month pulmonary TB regimen in its extended duration, because drug penetration into the CSF is lower than into lung tissue, and the granulomatous basal exudate acts as a pharmacological sanctuary harbouring viable bacilli even when serum drug levels appear adequate. The standard pulmonary TB continuation phase of 4 months is therefore insufficient for TBM: NTEP mandates a 10-month continuation phase (total 12 months), and prescribing only 6 months is a common and dangerous error. In addition to ATT, adjunctive dexamethasone has strong evidence for mortality reduction in TBM and must be given in all clinical stages from the outset. Management of complications — particularly hydrocephalus, seizures, and SIADH — runs concurrently and requires equal attention.
ATT regimen for TBM (NTEP/WHO):
The standard regimen is divided into two phases:
• Intensive phase: 2 months — HRZE — isoniazid (H) + rifampicin (R) + pyrazinamide (Z) + ethambutol (E), all four drugs daily, in weight-band fixed-dose combination tablets
• Continuation phase: 10 months — HR — isoniazid + rifampicin daily for 10 further months
• Total duration: 12 months (not 6 months as in pulmonary TB; TBM requires the extended continuation phase)
Weight-based dosing (per NTEP paediatric FDC bands):
| Drug | Dose (mg/kg/day) |
|---|---|
| Isoniazid (H) | 10 (range 7–15) |
| Rifampicin (R) | 15 (range 10–20) |
| Pyrazinamide (Z) | 35 (range 30–40) |
| Ethambutol (E) | 20 (range 15–25) |
Note: Ethambutol optic neuritis is dose-dependent; monitor visual acuity monthly. Isoniazid → peripheral neuropathy (give pyridoxine 5–10 mg/day supplement). Rifampicin → orange urine, hepatotoxicity; monitor LFT. Pyrazinamide → hepatotoxicity, hyperuricaemia.
Adjunctive dexamethasone (mandatory in all stages):
Dexamethasone is given alongside ATT in ALL stages of TBM to reduce vasogenic and cytotoxic oedema, decrease basal exudate formation, and lower mortality and severe disability:
• Starting dose: 0.4 mg/kg/day IV in divided doses (Stage II/III: may start higher)
• Taper over 4–6 weeks (not abrupt cessation — gradual step-down)
• Switch to oral prednisolone when the child can swallow
Management of hydrocephalus:
• Serial lumbar punctures (weekly, measuring opening pressure) may provide temporary relief in communicating hydrocephalus
• VP shunt insertion is required for hydrocephalus unresponsive to medical management or with progressive deterioration
Supportive care:
• Seizure control (levetiracetam preferred; avoid phenytoin/carbamazepine — enzyme inducers lower ATT levels)
• Nutritional support: high-calorie, protein-rich diet; correct malnutrition if present
• Contact tracing: identify the source case and other household contacts
• Notify under NTEP and initiate contact screening
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
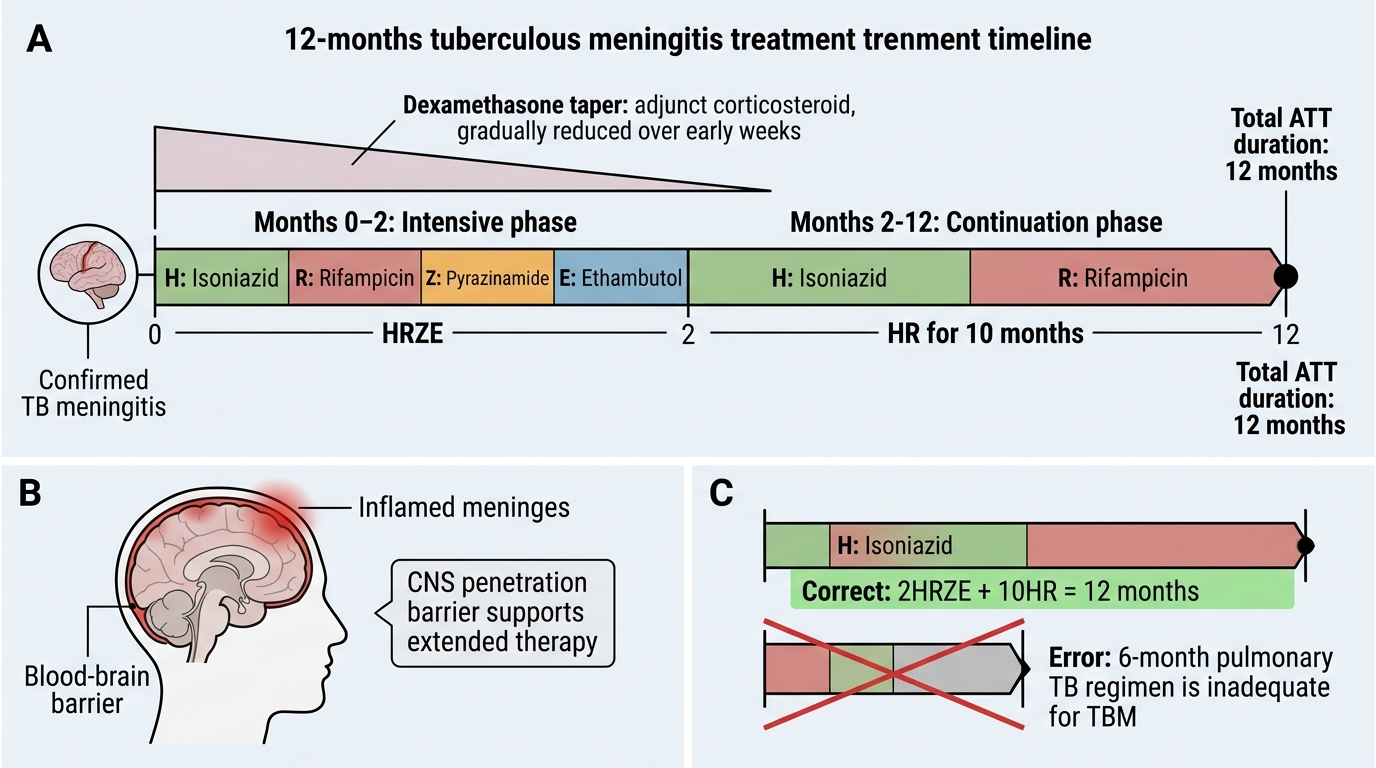
NTEP Treatment Timeline for Tuberculous Meningitis
SELF-CHECK
A child with confirmed TBM is started on ATT. What is the correct total duration of treatment, and what is the continuation phase regimen?
A. 6 months total; continuation = HRZ for 4 months
B. 9 months total; continuation = HR for 7 months
C. 12 months total; continuation = HR for 10 months
D. 18 months total; continuation = HRE for 16 months
Reveal Answer
Answer: C. 12 months total; continuation = HR for 10 months
NTEP recommends a total of 12 months for TBM: 2 months intensive phase (HRZE) + 10 months continuation phase (HR). This extended continuation (10 months vs 4 months for pulmonary TB) reflects the pharmacokinetic barrier of CNS penetration and the need to sterilise the granulomatous sanctuary. Using the standard 6-month pulmonary TB regimen for TBM is a treatment error and risks relapse.
Prevention of TBM
Prevention of TBM operates at the population level through vaccination and at the household level through contact tracing and chemoprophylaxis. Because TBM typically follows haematogenous spread from a primary pulmonary focus acquired in infancy or early childhood, early primary prevention is the most powerful intervention available.
BCG vaccination:
The BCG vaccine (Bacille Calmette-Guerin, live attenuated M. bovis) is given at birth under India's National Immunization Schedule (NIS), as a 0.05 mL intradermal injection into the left deltoid. BCG is the oldest and most widely administered vaccine globally. Its efficacy against pulmonary TB in adults is variable (0–80% across trials), but its protection against disseminated childhood TB — including TBM and miliary TB — is consistently high (60–80%). The mechanism is induction of cell-mediated immunity (CD4+ Th1 response) that limits haematogenous dissemination before meningeal seeding can occur. BCG does not prevent Mycobacterium tuberculosis infection; it prevents progression to severe disseminated disease. Every unvaccinated child presenting with a first episode of meningitis should be assessed for BCG scar.
Contact tracing and chemoprophylaxis:
Children under 5 years who are close household contacts of a confirmed sputum-positive pulmonary TB case have a high risk of primary TB acquisition and progression to disseminated disease including TBM. NTEP recommends:
• Screen all household contacts for symptoms and signs of TB
• For asymptomatic contacts aged <5 years: offer isoniazid preventive therapy (IPT) — isoniazid 10 mg/kg/day (max 300 mg/day) for 6 months
• For contacts who are PLHIV: IPT for 6 months regardless of age
Public health measures:
Adequate ventilation, early diagnosis and treatment of source cases, and nutritional improvement (malnutrition significantly increases TB susceptibility) are the broader preventive pillars.