Page 1 of 12
PE28.1 | Allergic Rhinitis — SDL Guide
Learning Objectives
- Describe the IgE-mediated pathogenesis of allergic rhinitis and the roles of early-phase and late-phase reactions
- Classify allergic rhinitis using the ARIA 2008 grid (intermittent/persistent × mild/moderate-severe)
- Recognise the clinical features of allergic rhinitis in children and differentiate from infectious rhinitis
- Outline a stepwise management plan including allergen avoidance, pharmacotherapy, and prevention strategies
- Enumerate indications and interpret findings of diagnostic tests including skin prick testing and specific IgE measurement
INSTRUCTIONS
Allergic rhinitis is the most common chronic inflammatory disease of the upper airways in children, affecting up to 20–30% of the paediatric population in India. Far from being a trivial 'sneezing illness', it impairs sleep, school performance, and quality of life — and, critically, it is the most powerful single risk factor for the development of childhood asthma. Understanding allergic rhinitis equips you to interrupt the 'allergic march' and manage the most prevalent atopic condition you will encounter in daily paediatric practice.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 16 (Allergic Disorders) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 150 (Allergic Rhinitis) (textbook)
- ARIA Guidelines 2001 (updated 2008, 2016) — Allergic Rhinitis and its Impact on Asthma (guideline)
- Indian Academy of Allergy (IAA) Consensus on Allergic Rhinitis in Indian Children (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya, a 9-year-old girl, presents with a 14-month history of near-daily sneezing, watery nasal discharge, and intense nasal itching that worsens every morning and during the dusty summer months in Chennai. Her mother reports that Priya wakes repeatedly at night, has become irritable, and her grades have dropped. On examination you note pale, bluish, swollen nasal turbinates, allergic shiners (dark infraorbital discolouration), and a transverse nasal crease across the bridge of her nose from repeated upward rubbing — the classic 'allergic salute'. There is no fever, no purulent discharge, and no sore throat. Three months ago she developed a dry nocturnal cough that her GP labelled 'viral'; spirometry now shows mild reversible airflow obstruction. What is unifying Priya's upper and lower airway disease, and what stepwise plan will you offer her family today?
WHY THIS MATTERS
Allergic rhinitis (AR) affects an estimated 20–30% of school-age children in India and is the leading cause of school absenteeism attributable to a chronic non-communicable disease. Its significance extends far beyond nasal symptoms: AR is the single strongest identifiable risk factor for the development of bronchial asthma, with 40–50% of children with AR eventually developing asthma — the 'one airway, one disease' concept. Sinusitis, otitis media with effusion, sleep-disordered breathing, and poor academic performance are well-documented co-morbidities. Correct early classification and stepwise management can substantially reduce the burden on children, families, and the health system. As a final-year student and future practitioner, you will diagnose and initiate management for AR more frequently than almost any other childhood inflammatory disease.
RECALL
Before proceeding, recall from your Year 1 Physiology and Biochemistry:
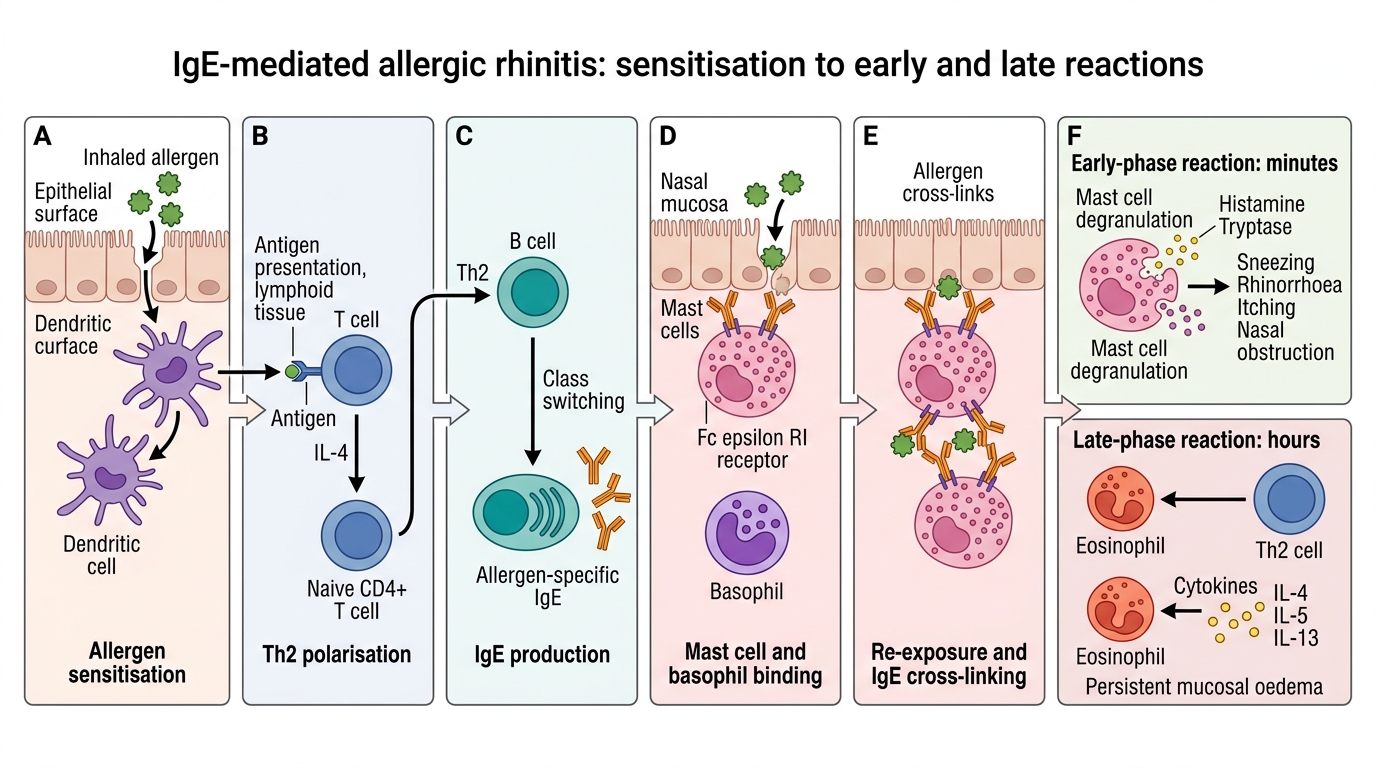
- Type I (immediate) hypersensitivity is an IgE-mediated reaction. On first allergen exposure (sensitisation phase), antigen-presenting cells activate Th2 lymphocytes, which drive B-cell class switching to produce allergen-specific IgE. This IgE binds high-affinity FcεRI receptors on mast cells and basophils. On re-exposure, allergen cross-links surface IgE, triggering rapid degranulation.
- Mast cell granules contain histamine, tryptase, and chymase; new synthesis releases prostaglandin D₂ and leukotriene C₄/D₄/E₄ — the cysteinyl leukotrienes responsible for the late-phase response.
- The nasal mucosa is a highly vascular, ciliated pseudostratified columnar epithelium with abundant mast cells and submucosal glands — ideal territory for an IgE-mediated response.
- The atopic triad (atopic dermatitis → allergic rhinitis → asthma) describes the sequential or simultaneous occurrence of these IgE-mediated diseases; a child with eczema has a substantially elevated risk of AR and asthma.
Clinical Presentation of Allergic Rhinitis in Children
The classic symptom quartet of allergic rhinitis — rhinorrhoea (watery, profuse nasal discharge), nasal pruritus, sneezing (often paroxysmal, particularly on waking), and nasal congestion — arises from the combined effects of histamine on H₁ receptors (itch, sneeze, hypersecretion) and leukotriene-driven oedema of the nasal mucosa (congestion). In children, nasal congestion is often the dominant and most troublesome symptom, causing mouth-breathing, snoring, and sleep disruption that parents frequently fail to associate with the underlying allergic process. Conjunctival symptoms (itching, redness, tearing — allergic conjunctivitis) co-occur in up to 70% of children with AR and should be specifically sought. Itching of the palate, throat, and ears is also common and reflects IgE-mast cell activation at mucous membrane surfaces that share embryological and immunological characteristics with the nasal mucosa.
The characteristic physical signs in children differ importantly from those in adults. The allergic salute — repeated upward rubbing of the nose with the palm — produces a transverse nasal crease across the lower third of the nasal bridge, pathognomonic when present. Allergic shiners (bilateral infraorbital venous congestion producing dark discolouration) result from impaired venous drainage due to nasal mucosal swelling. Nasal salute facies may include mouth-breathing, high-arched palate, and elongated face in chronic severe cases. On anterior rhinoscopy or nasal endoscopy, the inferior turbinates appear pale, bluish-grey, and swollen — in contrast to the red, friable turbinates of infectious rhinitis — and watery secretions are visible in the inferior and middle meatus.
Key co-morbidities to assess in every child with AR include: asthma (auscultate for wheeze; ask about nocturnal/exercise cough), atopic dermatitis (examine skin flexures), allergic conjunctivitis (examine conjunctivae), sinusitis (tenderness over paranasal sinuses; ask about facial pain/pressure), and otitis media with effusion (assess middle-ear pressure and hearing; AR causes eustachian tube dysfunction).
| Feature | Allergic Rhinitis | Infectious (Viral) Rhinitis | Non-Allergic Rhinitis |
|---|---|---|---|
| Discharge | Watery, profuse | Initially watery → mucopurulent | Clear or varied |
| Sneezing | Paroxysmal (often ≥5 in a row) | Occasional | Variable |
| Nasal itch | Prominent | Minimal | Absent |
| Duration | Weeks–months | 7–10 days | Persistent, no allergen link |
| Fever | Absent | Common early | Absent |
| Season/allergen pattern | Yes | No | No |
| Turbinate colour | Pale, blue-grey | Red, inflamed | Varies |
| Eosinophilia | Present (nasal smear/blood) | Absent | Absent (NARES: present) |
Pathophysiology and Aetiology
The immunopathogenesis of allergic rhinitis is a two-phase process rooted in aberrant Th2 immune polarisation. During the sensitisation phase, inhaled allergens penetrate the nasal epithelium and are taken up by dendritic cells, which migrate to regional lymph nodes and present processed peptides to naïve T-cells. In genetically atopic individuals, the cytokine milieu (IL-4, IL-13 from Th2 cells; IL-25, IL-33, TSLP from the epithelium — the 'epithelial cytokine alarm') drives T-cell differentiation towards a Th2 phenotype. Th2 cells produce IL-4, IL-5, and IL-13, which collectively instruct B-cells to undergo class-switch recombination from IgM/IgG to IgE production. Allergen-specific IgE enters the circulation and binds high-affinity FcεRI receptors on mucosal mast cells and circulating basophils — priming the individual for the effector phase without causing symptoms at this stage.
On re-exposure, the same allergen cross-links adjacent membrane-bound IgE molecules, triggering receptor aggregation and within seconds initiating a calcium-dependent signalling cascade that results in mast cell degranulation. The early-phase reaction (0–1 hour after allergen contact) is driven by preformed mediators — primarily histamine (itch, sneeze, hypersecretion via H₁ receptors; vasodilation and increased vascular permeability causing congestion), tryptase (serine protease; marker of mast-cell activation), and prostaglandin D₂. The late-phase reaction (4–8 hours; accounts for persistent congestion between allergen exposures) results from newly synthesised cysteinyl leukotrienes (LTC₄, LTD₄, LTE₄) and cytokine-driven recruitment of eosinophils, basophils, and Th2 cells into the nasal mucosa. Eosinophil-derived major basic protein and eosinophil cationic protein amplify mucosal damage and perpetuate inflammation. Repeated allergen exposure leads to priming — progressive reduction in the threshold for mast cell activation — explaining why symptoms worsen progressively over an allergy season.
Aetiological allergens in the Indian paediatric context fall into two broad categories. Perennial allergens (present year-round) include house-dust mite (Dermatophagoides pteronyssinus and D. farinae — the dominant allergen across Indian urban and semi-urban settings), cockroach (Blattella germanica — high sensitisation rates in warm, humid Indian homes), mould spores (Aspergillus, Cladosporium, Alternaria — prevalent in humid coastal climates), and pet dander (cats > dogs; less common in most Indian households but increasing). Seasonal allergens (pollen season) include grass pollen (most important in India — Bermuda grass/Cynodon dactylon is the single most common Indian allergen), tree pollen (spring), and weed pollen (ragweed-equivalent species). Occupational/domestic exposure (incense smoke, biomass fuel combustion, tobacco smoke — though smoke is non-allergenic, it acts as an adjuvant that upregulates IgE responses and damages the epithelial barrier) acts as an aggravating factor.
Genetic predisposition is polygenic: first-degree relative with atopy increases risk ~2–3-fold; both parents atopic → ~60–70% risk. Filaggrin gene mutations (FLG) that cause impaired epithelial barrier are associated with atopic march severity.
IgE-Mediated Allergic Rhinitis Mechanism
SELF-CHECK
A 7-year-old presents with 8 months of near-daily nasal symptoms that are consistently worse in the morning. On examination you note pale, swollen turbinates and a transverse crease across the nasal bridge. Which ARIA classification best applies?
A. Intermittent, mild
B. Intermittent, moderate-severe
C. Persistent, mild
D. Persistent, moderate-severe
Reveal Answer
Answer: D. Persistent, moderate-severe
ARIA persistent = symptoms >4 days/week AND >4 consecutive weeks. This child has near-daily symptoms for 8 months, satisfying the persistent criterion. Moderate-severe = ≥1 of: sleep disturbance, impaired daily activities, impaired school performance, or troublesome symptoms. Morning worsening with likely sleep disruption makes this moderate-severe. Option A (intermittent, mild) would require symptoms <4 days/week or <4 consecutive weeks. Option C (persistent, mild) would require persistent frequency but NO impact on any quality-of-life domain — inconsistent with the morning predominance and likely sleep disruption.
ARIA Classification and Diagnosis
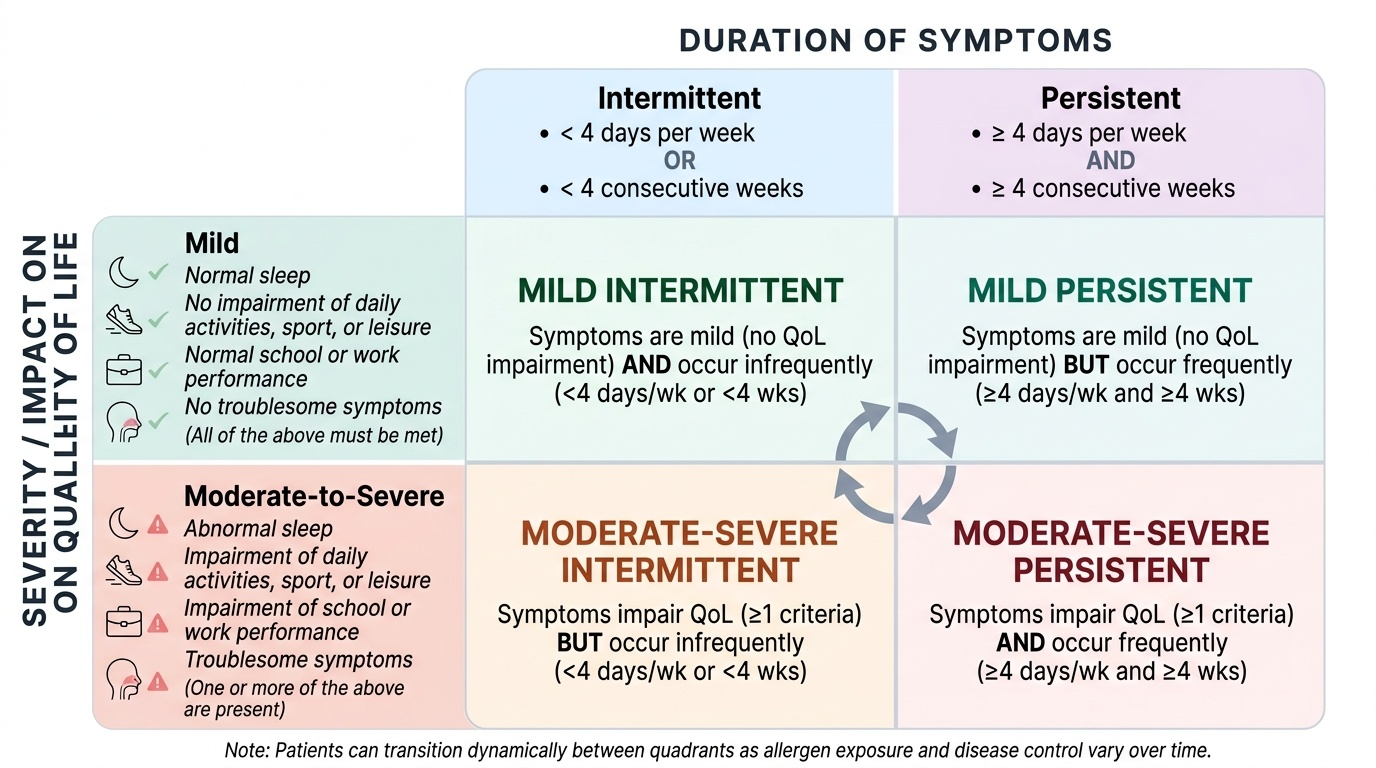
The ARIA (Allergic Rhinitis and its Impact on Asthma) classification, first published in 2001 and updated in 2008 and 2016, replaced the older 'seasonal vs perennial' dichotomy because it better predicts disease burden and guides treatment intensity. The ARIA working group recognised that the prior 'seasonal' and 'perennial' categories did not reflect the natural history of the disease: many patients with 'seasonal' AR have year-round perennial sensitisation as well, and the critical determinant of treatment intensity is not when the allergen is present but how severely it impairs the patient's life. The ARIA grid is therefore a two-dimensional matrix — the first axis describes duration (how often and how long symptoms occur) and the second describes severity impact (whether and how many quality-of-life domains are affected). Crucially, a child can be classified in one of four quadrants at any one time, and the classification can change as allergen exposure and disease control vary across the year. This dynamic, patient-centred framework makes ARIA directly actionable for treatment escalation and de-escalation decisions in the clinic.
Provided image
Duration axis:
- Intermittent AR: symptoms present <4 days/week OR <4 consecutive weeks
- Persistent AR: symptoms present >4 days/week AND >4 consecutive weeks
Severity axis:
- Mild AR: symptoms present but NONE of the following impaired: sleep, daily activities/sport/leisure, school/work performance; AND symptoms not troublesome
- Moderate-severe AR: ≥1 of the following: sleep disturbed, daily activities/sport/leisure impaired, school/work impaired, OR symptoms troublesome
In practice, the four resultant quadrants (intermittent-mild, intermittent moderate-severe, persistent-mild, persistent moderate-severe) map directly onto treatment steps: intermittent-mild → oral antihistamine or INCS; intermittent moderate-severe and persistent-mild → INCS ± oral antihistamine; persistent moderate-severe → INCS as backbone, add antihistamine and/or LTRA, consider immunotherapy.
Diagnostic workup in a child with suspected AR follows a stepwise logic. The diagnosis is primarily clinical in most cases — a history of the symptom quartet (rhinorrhoea, itch, sneeze, congestion) with an allergen-linked pattern, appropriate physical signs (pale turbinates, allergic shiners, nasal crease), and exclusion of infectious or structural causes is sufficient to initiate treatment. Investigations add value in moderate-severe or treatment-resistant cases, in atypical presentations, and to guide allergen-specific immunotherapy.
Allergy skin testing:
Skin prick test (SPT) is the first-line allergy test. A 1-mm lancet is used to introduce a drop of standardised allergen extract through the epidermis of the volar forearm. A wheal of ≥3 mm above the negative saline control at 15–20 minutes is a positive result (the negative control is saline; histamine is the positive control and must show ≥3 mm wheal to confirm skin reactivity). SPT is specific (high positive predictive value when combined with a consistent history), cheap, and immediately interpretable, but must be performed with antihistamines withheld for 3–5 days (antihistamines blunt the response). It is safe in children ≥2–3 years with trained staff and resuscitation available.
Serum-specific IgE (sIgE):
ImmunoCAP or RAST measures allergen-specific IgE in serum (reported in kUA/L; class 0–6 with class ≥2 [0.35 kUA/L] regarded as positive). Unlike SPT, sIgE is unaffected by antihistamines, is safe in patients with severe eczema (difficult SPT site) or history of anaphylaxis, but is more costly and results take days. Total serum IgE is NOT a reliable diagnostic marker alone — it is elevated in parasitic infestations, some immunodeficiencies, and non-atopic conditions, and normal total IgE does not exclude AR.
Nasal cytology: A nasal smear showing >10–20% eosinophils supports allergic rhinitis and differentiates it from infectious rhinitis (neutrophils predominate) and non-allergic rhinitis with eosinophilia syndrome (NARES — eosinophilic but sIgE-negative).
Radiology: Plain sinus X-rays are rarely necessary; mucosal thickening may be seen but is non-specific. CT sinuses is reserved for complications (chronic sinusitis, suspected structural abnormality).
Pulmonary function testing (PFT): All children with moderate-severe or persistent AR should have spirometry to screen for comorbid asthma, particularly when there is exercise intolerance, nocturnal cough, or wheeze (see PE28.4).
CLINICAL PEARL
The 'one airway, one disease' trap: Many practitioners treat allergic rhinitis in isolation without screening for asthma, and vice versa. The same IgE-mediated Th2 inflammation that drives nasal mucosal oedema also primes bronchial mast cells. Studies show that 40% of children with AR have undiagnosed asthma and that treating nasal inflammation with intranasal corticosteroids reduces bronchial hyperreactivity and reduces asthma exacerbation rates. In every child with AR — and every child with asthma — screen for both conditions. A nasal wash (saline irrigation) that clears the nasopharynx reduces the aspiration of nasal mediators into the lower airway and is a zero-cost adjunct to management. The ARIA recommendation is explicit: 'assess the lower airway in any patient with rhinitis, and the upper airway in any patient with asthma.'