Page 2 of 12
PE28.1 | Allergic Rhinitis — SDL Guide (Part 2)
Management: Stepwise Treatment and Prevention
Management of allergic rhinitis in children follows an integrated stepwise approach that spans allergen avoidance (the only disease-modifying non-pharmacological strategy), pharmacotherapy titrated to ARIA severity, and allergen immunotherapy for selected cases. The overarching goal is to restore normal nasal airflow, sleep quality, and school performance while minimising drug adverse effects — critical in a paediatric population where sedation, growth suppression, and systemic effects of corticosteroids require active vigilance.
Provided image
Step 1 — Allergen avoidance and environmental control (all patients; foundational):
Avoiding the causative allergen is the most cost-effective intervention, though often incompletely achievable. For house-dust mite (dominant Indian trigger): use allergen-impermeable mattress and pillow encasings; wash bedding weekly in water ≥60°C; reduce indoor humidity to <50%; remove carpets and stuffed toys from the sleeping area; HEPA air purifiers may help. For cockroach: seal cracks, eliminate food sources, use integrated pest management (not insecticide sprays which worsen respiratory symptoms). For moulds: repair damp walls; avoid damp indoor spaces; dehumidify. For pollen: close windows during high-pollen times (mornings in Indian cities); wear masks outdoors during peak season; shower after outdoor play. Tobacco smoke avoidance is mandatory — parental smoking approximately doubles the risk of AR and asthma exacerbation.
Step 2 — Pharmacotherapy (titrated to ARIA classification):
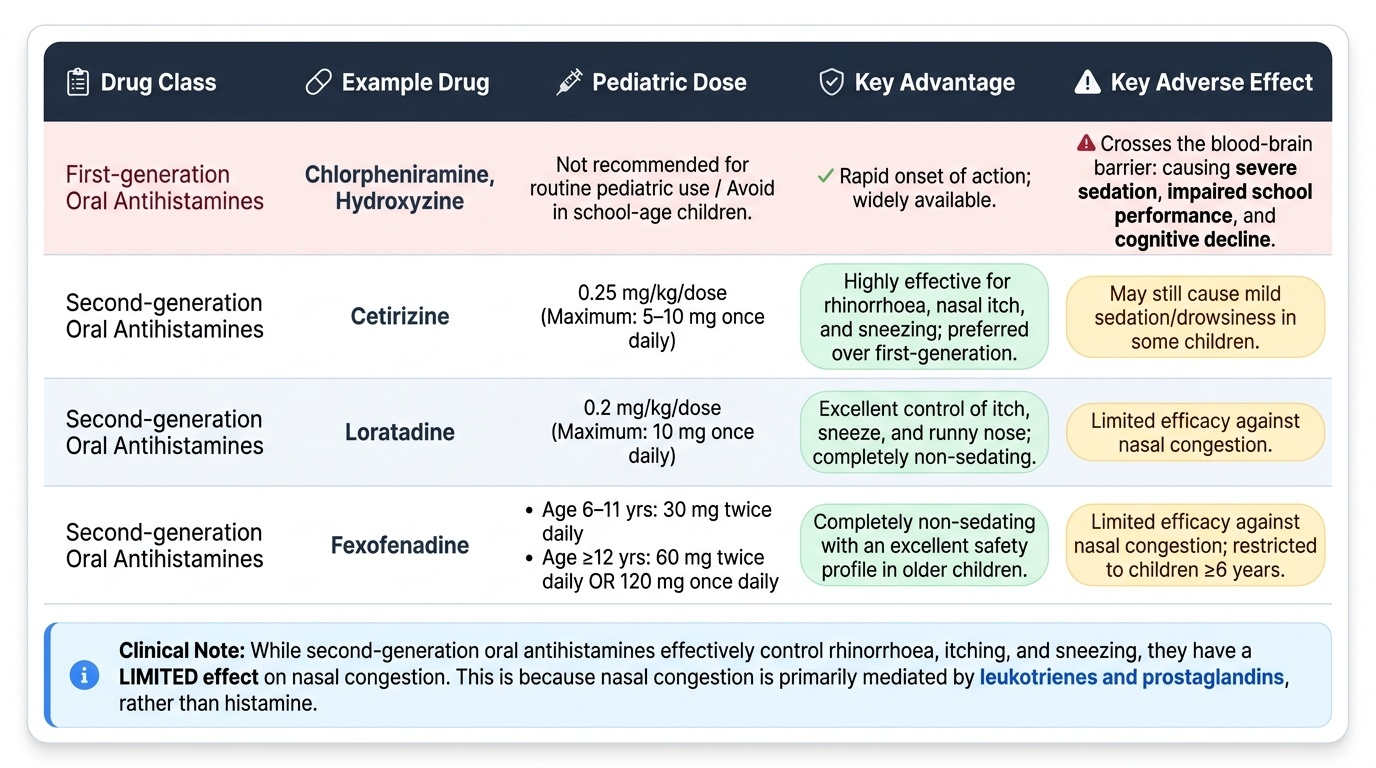
Oral antihistamines (H₁-receptor antagonists): First-generation agents (chlorpheniramine, hydroxyzine) cross the blood–brain barrier, causing sedation that impairs school performance and cognitive function — avoid in school-age children for regular use. Second-generation agents are preferred: cetirizine (0.25 mg/kg/dose, maximum 5–10 mg once daily; may cause mild sedation in some children), loratadine (0.2 mg/kg/dose, maximum 10 mg once daily; non-sedating), fexofenadine (non-sedating; approved ≥6 years at 30 mg twice daily for 6–11 years, 60 mg twice daily or 120 mg once daily for ≥12 years). Antihistamines control rhinorrhoea, itch, and sneezing effectively but have LIMITED effect on nasal congestion (congestion is primarily leukotriene- and prostaglandin-mediated, not histamine-mediated).
Intranasal corticosteroids (INCS): INCS are the most effective single-agent pharmacotherapy for AR and are the first-line treatment for persistent moderate-severe disease. Available agents in India include budesonide (64 µg/spray, 1–2 sprays per nostril once daily), mometasone furoate (50 µg/spray, 1–2 sprays per nostril once daily; lowest bioavailability — preferred in children ≥2–3 years), fluticasone propionate (50 µg/spray), and beclomethasone. INCS suppress both the early and late-phase inflammatory responses. Key counselling points: onset of action is within 6–12 hours of the first dose but maximum effect takes 1–2 weeks of regular use; patients must be told this to ensure adherence. Correct technique (angling the spray toward the outer nasal wall, not the septum) prevents nasal septal perforation (rare but well-documented). Systemic bioavailability is <1% for mometasone and fluticasone; growth suppression is not clinically significant at recommended doses.
Leukotriene receptor antagonists (LTRA): Montelukast (4 mg granules for <5 years; 5 mg chewable for 6–14 years; 10 mg for ≥15 years — given once daily in the evening) blocks CysLT₁ receptors. It has modest efficacy for AR alone but is particularly valuable in the coexistence of AR and asthma where it addresses both upper and lower airway inflammation with a single agent. It is also useful for isolated nasal congestion (its leukotriene mechanism targets congestion more than histamine blockers). NOTE: the FDA (2020) black-box warning on montelukast regarding neuropsychiatric effects (agitation, nightmares, suicidal ideation) — counsel families and monitor, particularly in children with underlying anxiety or depression.
Decongestants (nasal or oral): Topical decongestants (xylometazoline, oxymetazoline) relieve congestion rapidly but cause rebound rhinitis medicamentosa with use beyond 3–5 days — avoid in children for regular use. Oral decongestants (pseudoephedrine) cause CNS stimulation, insomnia, hypertension, and are not recommended in children <12 years (and cautiously only in older adolescents).
Nasal saline irrigation: Isotonic or hypertonic saline rinses (350–400 mOsm/L) remove allergens, crusts, and mediators from the nasal mucosa, improve mucociliary clearance, and reduce symptom scores as an adjunct to pharmacotherapy. Safe and very well-tolerated in children ≥2–3 years who can cooperate; recommend twice-daily irrigation during high-allergen periods.
Step 3 — Allergen Immunotherapy (AIT) for selected patients:
Subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT) are the only disease-modifying treatments for AR — they reprogram the immune response from Th2 toward a regulatory/Th1 phenotype, inducing allergen tolerance. Indications in children: moderate-severe persistent AR with confirmed allergen sensitisation (positive SPT/sIgE), inadequate symptom control on optimal pharmacotherapy, comorbid asthma (SLIT is approved as add-on for mild-moderate asthma in AR patients), or patient/family preference to reduce long-term medication dependence. AIT is generally not initiated before age 5 years. Duration: 3–5 years for sustained benefit. SCIT carries a small risk of anaphylaxis (must be administered in a clinical setting with 30-minute observation and epinephrine available); SLIT has a better safety profile suitable for home administration after initial supervised doses.
Prevention:
Primary prevention of AR (in high-risk atopic infants): exclusive breastfeeding for 6 months (IAP recommendation) reduces the severity of early atopy. Avoiding early introduction of highly allergenic foods is NOT recommended (the LEAP trial paradigm — early peanut introduction reduces sensitisation; early introduction of diverse foods is now favoured). Reducing indoor allergen load in the homes of atopic families (HDM encasements, no pets) reduces sensitisation rate. Secondary prevention (in sensitised children): early, consistent allergen avoidance; early initiation of INCS to reduce the risk of asthma development (emerging evidence from PRESTO and similar trials).
SELF-CHECK
A 10-year-old with persistent moderate-severe allergic rhinitis is unresponsive to cetirizine for 6 weeks. Which is the most appropriate next step?
A. Add oral decongestant (pseudoephedrine) long-term
B. Switch to first-generation antihistamine (chlorpheniramine) for stronger effect
C. Add intranasal corticosteroid (mometasone furoate) as first-line backbone therapy
D. Refer for allergen immunotherapy immediately without further pharmacotherapy
Reveal Answer
Answer: C. Add intranasal corticosteroid (mometasone furoate) as first-line backbone therapy
Intranasal corticosteroids (INCS) are the most effective single pharmacotherapy for AR and are the first-line treatment for persistent moderate-severe disease — cetirizine (antihistamine) alone addresses itch/sneeze/rhinorrhoea but not the dominant eosinophilic inflammation and congestion of persistent disease. Mometasone furoate has the lowest systemic bioavailability and is safe in children from ≥2–3 years. Option A is incorrect: topical decongestants cause rhinitis medicamentosa after >5 days; oral decongestants are not recommended in children <12 years. Option B is incorrect: first-generation antihistamines sedate and impair school performance — never preferred in school-age children. Option D is premature: allergen immunotherapy is indicated only after optimal pharmacotherapy has been tried and confirmed inadequate, in children ≥5 years with confirmed sensitisation.
Self-Assessment and Key Take-Aways
Allergic rhinitis is a chronic inflammatory disease of the upper airway driven by IgE-mediated Type I hypersensitivity and Th2 polarisation. Its correct recognition, classification, and treatment reduces the risk of asthma development and restores quality of life. The essential take-aways from this module are:
Classification: Apply the ARIA grid — duration (intermittent vs persistent) and severity impact (mild vs moderate-severe) — as the clinical decision framework. Do not use the older seasonal/perennial dichotomy for management decisions.
Mechanism: Distinguish early-phase (histamine, tryptase — itch, sneeze, secretion within minutes) from late-phase (leukotrienes, eosinophils — congestion, persisting 4–8 hours and beyond). Both phases are suppressed by INCS; antihistamines primarily address the early phase.
Diagnosis: Primarily clinical. SPT (wheal ≥3 mm above negative control = positive) or serum-specific IgE (ImmunoCAP class ≥2 = positive) confirm sensitisation. Total serum IgE alone is NOT diagnostic. All moderate-severe AR in children warrants spirometry to screen for comorbid asthma.
Management priority: INCS (mometasone, budesonide, fluticasone) are the first-line backbone for persistent moderate-severe AR. Second-generation antihistamines (cetirizine mg/kg, loratadine, fexofenadine) address itch/sneeze/rhinorrhoea. Montelukast (LTRA) is particularly valuable when AR coexists with asthma. Avoid first-generation sedating antihistamines and decongestants in children.
Prevention and the allergic march: Allergen avoidance + early INCS + tobacco smoke elimination are the pillars of preventing progression to asthma. 'One airway, one disease' — always assess both upper and lower airways.
Key dosing (weight-based — always):
- Cetirizine: 0.25 mg/kg/dose once daily (max 5–10 mg)
- Loratadine: 0.2 mg/kg/dose once daily (max 10 mg)
- Montelukast: 4 mg (<5 yr), 5 mg (6–14 yr), 10 mg (≥15 yr) — once nightly
- INCS: 1–2 sprays per nostril once daily (dose per spray varies by formulation)