Page 8 of 14
PE29.5 | Klinefelter Syndrome — SDL Guide (Part 2)
Management, Complications, and Genetic Counselling
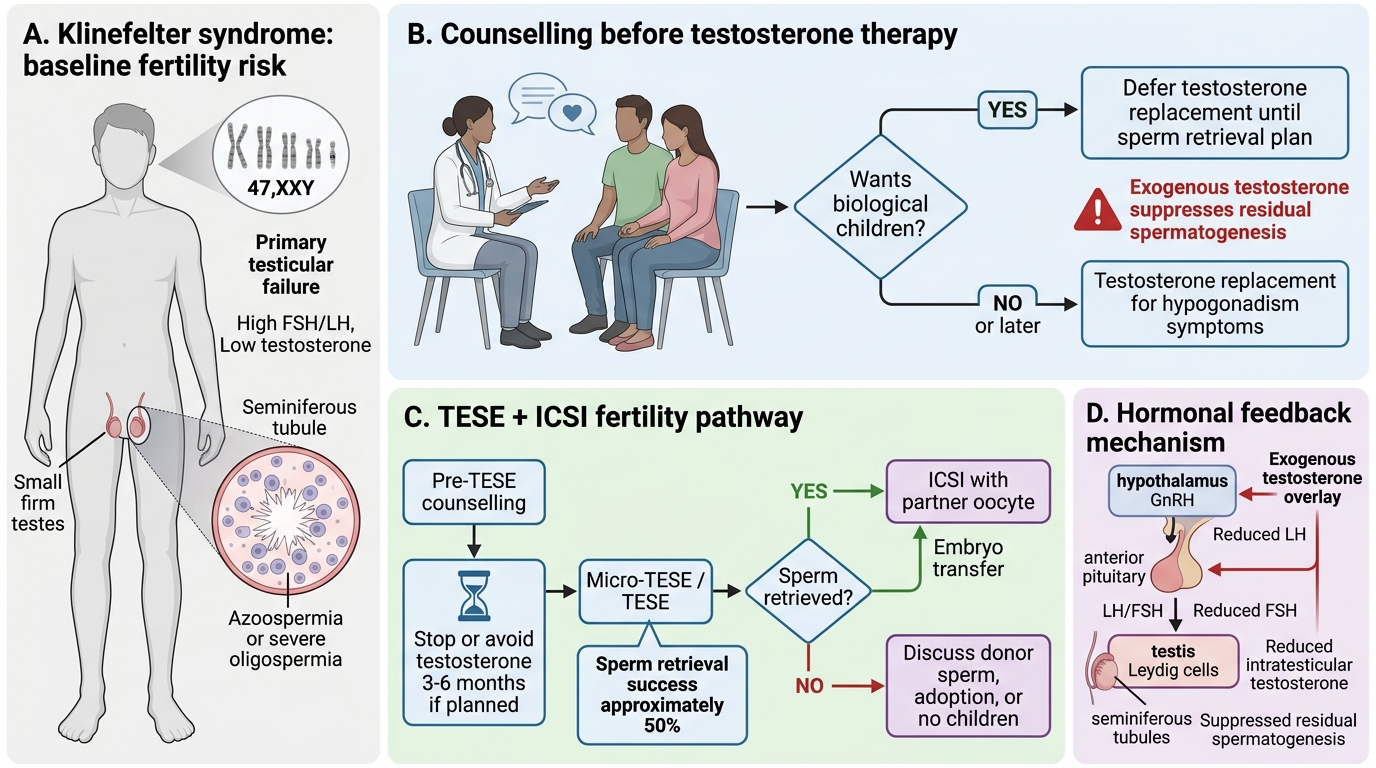
Management of Klinefelter syndrome addresses testosterone deficiency, gynaecomastia, fertility, and surveillance for systemic complications. Like Turner syndrome, the interventions are time-sensitive in some domains — testosterone replacement should ideally begin at the onset of puberty to prevent androgen deficiency sequelae, and testicular sperm extraction for fertility purposes is more successful when attempted before further tubular hyalinisation progresses. The paediatrician initiates the process and coordinates the transition to adult endocrine and reproductive medicine services. An important and frequently-tested clinical principle is that testosterone replacement and fertility preservation are mutually exclusive goals if not carefully sequenced: exogenous testosterone suppresses the HPG axis and reduces residual spermatogenesis, so any plan for TESE must be discussed and either performed or banked before long-term testosterone therapy is established. Getting this sequence right is among the most practically consequential skills a clinician managing Klinefelter syndrome can acquire.
Testosterone replacement therapy:
• Indication: All boys with confirmed Klinefelter syndrome and evidence of androgen deficiency or incomplete virilisation.
• Timing: Initiated at early puberty (~11–12 years of age) with intramuscular testosterone esters (testosterone enantate or cypionate) or transdermal testosterone gel. Starting at puberty age allows physiological virilisation (voice change, beard growth, penile growth, body composition).
• Target: Mid-normal adult male testosterone range (12–35 nmol/L). Monitor with testosterone trough levels, haematocrit, and lipids.
• Long-term benefits: Improved energy, libido, muscle mass, bone density, and cognitive function. Does not reverse azoospermia.
• Important limitation: Testosterone replacement alone does NOT restore fertility — this is a common misconception. Exogenous testosterone actually suppresses the hypothalamic-pituitary-gonadal axis and may reduce residual sperm production if TESE is planned; therefore, fertility planning must precede or be concurrent with testosterone initiation.
Gynaecomastia:
• Mild gynaecomastia may regress with testosterone replacement. Persistent or significant gynaecomastia (cosmetically or psychologically distressing) requires surgical reduction (mastectomy).
• Psychological impact of gynaecomastia in adolescence can be significant; early management reduces social morbidity.
Fertility management:
• Testicular sperm extraction (TESE) + intracytoplasmic sperm injection (ICSI): Despite azoospermia in the ejaculate, focal areas of residual spermatogenesis exist in approximately 50% of 47,XXY men. TESE retrieves sperm directly from testicular tissue; ICSI injects a single sperm into an egg; live birth rates are ~30–40% per cycle with retrieved sperm.
• Timing: TESE is ideally performed in adolescence or early adulthood (before progressive tubular hyalinisation destroys remaining foci). Testosterone replacement must be stopped 3–6 months before TESE to avoid axis suppression.
• Offspring risk: Offspring conceived via TESE-ICSI from a 47,XXY father are not at significantly increased risk of Klinefelter syndrome — the sperm retrieved are primarily haploid (23,X or 23,Y), not aneuploid. However, antenatal genetic testing is offered to all couples.
Systemic complications — surveillance:
• Osteoporosis: From androgen deficiency; DEXA scan at diagnosis and periodically; adequate testosterone and calcium/vitamin D intake.
• Metabolic syndrome: Increased risk of type 2 diabetes, hypertension, dyslipidaemia; annual fasting glucose, lipid profile, blood pressure.
• Autoimmune conditions: Increased risk of systemic lupus erythematosus and Sjögren's syndrome; keep in the differential if appropriate symptoms.
• Breast cancer: Slightly elevated risk (~20× above general male population) due to gynaecomastia and oestrogen exposure; annual examination.
Genetic counselling:
• Recurrence risk: Klinefelter syndrome is sporadic; the recurrence risk in future pregnancies is not significantly elevated above background. Parental karyotypes are normal.
• Prenatal diagnosis (cfDNA or amniocentesis) should be offered in future pregnancies.
• Psychosocial support for the adolescent (identity, puberty, infertility) should be provided through appropriate counselling services.
Fertility Management in Klinefelter Syndrome
SELF-CHECK
A 19-year-old man with Klinefelter syndrome (47,XXY) is planning to start testosterone replacement therapy. His partner wants to have children. What is the most important counselling point regarding testosterone and fertility?
A. Testosterone replacement will restore spermatogenesis and natural conception may be possible within 6 months
B. Testosterone replacement must be deferred until after TESE is performed, as exogenous testosterone suppresses residual spermatogenesis
C. TESE is not possible in Klinefelter syndrome because all seminiferous tubules are destroyed
D. Testosterone replacement has no effect on fertility — TESE can be performed at any time regardless of testosterone use
Reveal Answer
Answer: B. Testosterone replacement must be deferred until after TESE is performed, as exogenous testosterone suppresses residual spermatogenesis
Exogenous testosterone suppresses the hypothalamic-pituitary-gonadal axis via negative feedback, reducing LH stimulation of Leydig cells and FSH stimulation of residual spermatogenesis. If TESE is planned, testosterone replacement should either be deferred until after sperm retrieval or discontinued for at least 3–6 months before TESE to allow recovery of residual spermatogenesis. TESE is indeed possible in 47,XXY males — approximately 50% have focal residual spermatogenesis. Testosterone replacement does not restore spermatogenesis or allow natural conception, as the tubular damage is structural and irreversible in the ejaculate.
Self-Assessment
Use these questions to assess your readiness to diagnose, investigate, and manage a male patient with Klinefelter syndrome. Klinefelter syndrome is frequently under-diagnosed — and the cost of a missed diagnosis is lost testosterone-replacement opportunity, uncontrolled androgen deficiency, progressive bone loss, and a fertility window that closes irreversibly as tubular hyalinisation advances. The questions below are designed to test your ability to apply the genetic, endocrinological, and counselling knowledge from this module in realistic clinical scenarios, including distinguishing Klinefelter syndrome from other causes of delayed puberty and from other sex-chromosome aneuploidies. A complete, unprompted answer to each question below demonstrates competency at the level required for PE29.5 in the MBBS examination. Work through them carefully before your next clinical posting.
Structured self-check questions:
- What is the karyotype of classic Klinefelter syndrome? By what mechanism does the extra X arise, and does maternal age increase the risk?
- A 15-year-old with small firm testes and gynaecomastia has markedly elevated FSH and LH with low testosterone. Localise the defect to the correct level of the hypothalamic-pituitary-gonadal axis and name the expected hormonal pattern.
- Explain why testosterone replacement does NOT restore fertility in Klinefelter syndrome, and what fertility option is available instead.
- At what age would you start testosterone replacement in a boy with confirmed Klinefelter syndrome, and what are the long-term goals of this therapy?
- Distinguish Klinefelter syndrome from constitutional delayed puberty on physical examination and investigations.
- A couple asks about the recurrence risk of Klinefelter syndrome in future pregnancies. What do you tell them?
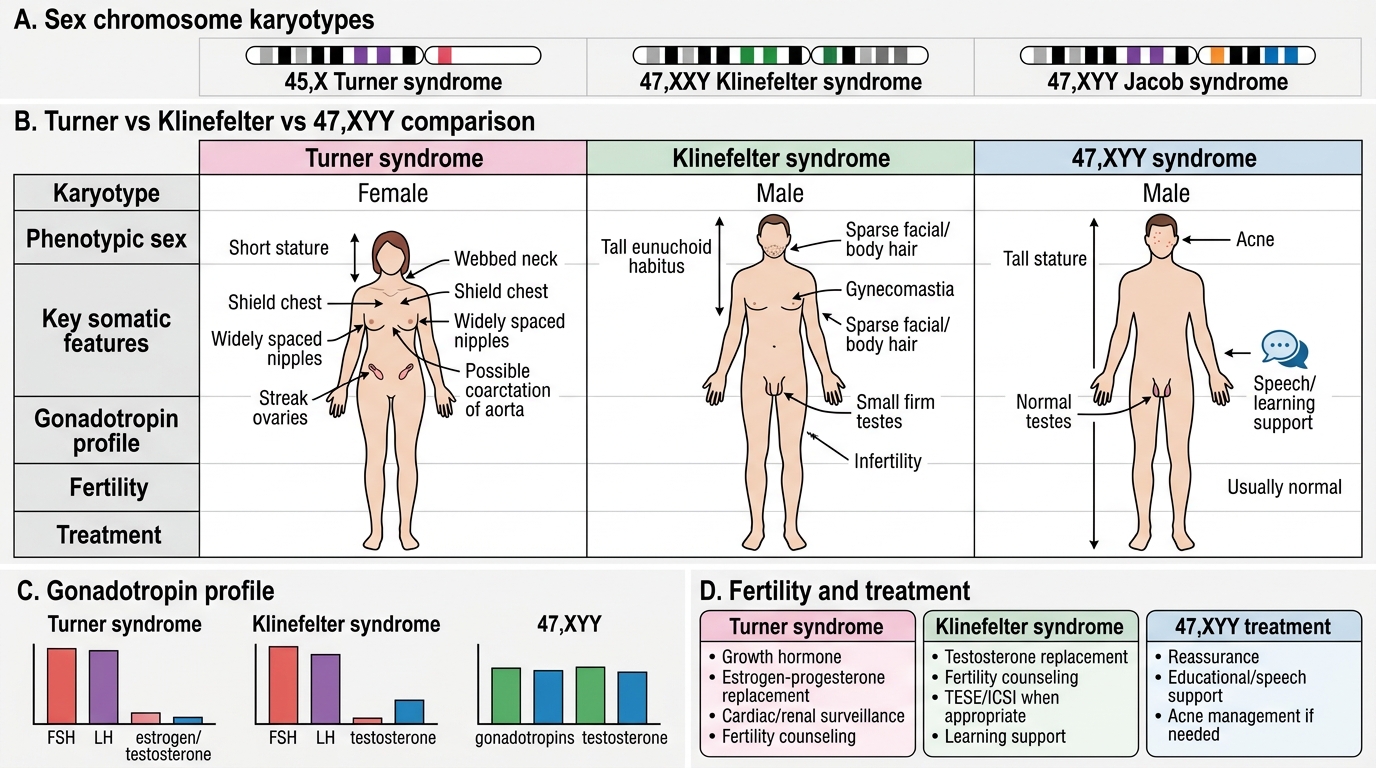
Turner vs Klinefelter vs 47,XYY Syndrome