Page 16 of 32
PE31.11 | Diphtheria Pertussis Tetanus — SDL Guide
Learning Objectives
- Recognise the clinical presentations of diphtheria (pseudomembrane, bull-neck), pertussis (paroxysmal whoop, apnoea), and tetanus (trismus, risus sardonicus, opisthotonus) including their distinct prodromal phases
- Explain the bacterial toxin mechanisms underlying the pathognomonic features of each disease
- Identify the serious complications of each — diphtheria myocarditis and neuropathy, pertussis apnoea in infants, tetanus autonomic instability
- Describe specific management: diphtheria antitoxin + penicillin; pertussis macrolide; tetanus TIG + metronidazole + diazepam; and prevention through the National Immunization Schedule
INSTRUCTIONS
Diphtheria, pertussis, and tetanus are three historically devastating childhood infections that are now vaccine-preventable yet still occur in under-immunised communities. Together they illustrate how bacterial toxins can cause clinical pictures entirely distinct from the infection site itself — a throat infection causing heart block, a cough illness causing lymphocytosis, a minor wound causing generalised spasticity. Mastering the clinical recognition and toxin-specific treatment of each disease is essential for any paediatrician practising in India.
References
- Ghai Essential Pediatrics, 9th ed, Ch 10 — Bacterial Infections (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 204-207 (textbook)
- IAP Standard Treatment Guidelines — Diphtheria, Pertussis, Tetanus (guideline)
- National Immunization Schedule, Ministry of Health & Family Welfare, India 2023 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three children arrive in your district hospital emergency department on the same day. The first is an 8-year-old with a grey membrane in his throat, a muffled voice, and a neck so swollen his mother says he looks like a bull. The second is a 4-month-old who has been coughing in violent, uncontrollable bursts for three weeks — each burst ending with a desperate, high-pitched whoop and sometimes turning blue. The third is a 10-day-old neonate who was delivered at home; over the past day he has stopped feeding, his jaw is clenched shut, and his whole body goes rigid when you touch him. Three different bacteria, three different toxins, three life-threatening emergencies. All three were preventable with a single course of pentavalent vaccine.
WHY THIS MATTERS
Despite being among the oldest vaccine-preventable diseases in paediatric history, diphtheria, pertussis, and tetanus continue to cause preventable deaths in India — particularly in communities with vaccination gaps or low coverage. Pertussis has resurged even in high-income countries due to waning vaccine immunity. Neonatal tetanus, though dramatically reduced by universal immunisation programmes, remains a cause of neonatal mortality in home deliveries where cord-hygiene practices are inadequate. The clinician who recognises these diseases early — before the characteristic signs are fully evolved — can initiate antitoxin or antibiotics before irreversible toxin-mediated damage occurs. These diseases also exemplify the public health imperative of achieving high vaccination coverage.
RECALL
Before proceeding, activate your prior knowledge: from Microbiology, recall that Corynebacterium diphtheriae is a gram-positive, non-sporing rod; Bordetella pertussis is a gram-negative coccobacillus; Clostridium tetani is an anaerobic, gram-positive, spore-forming rod. From Physiology, recall that glycine and GABA are inhibitory neurotransmitters in the spinal cord — their blockade produces unopposed motor excitation. From the National Immunization Schedule, recall that the pentavalent vaccine (DPT + hepatitis B + Hib) is given at 6, 10, and 14 weeks of age in India, with a DPT booster at 16–24 months and again at 5–6 years. From prior learning, recall that a toxoid is a chemically inactivated toxin used in vaccines to induce immunity without causing disease.
Clinical Presentation of Diphtheria, Pertussis, and Tetanus
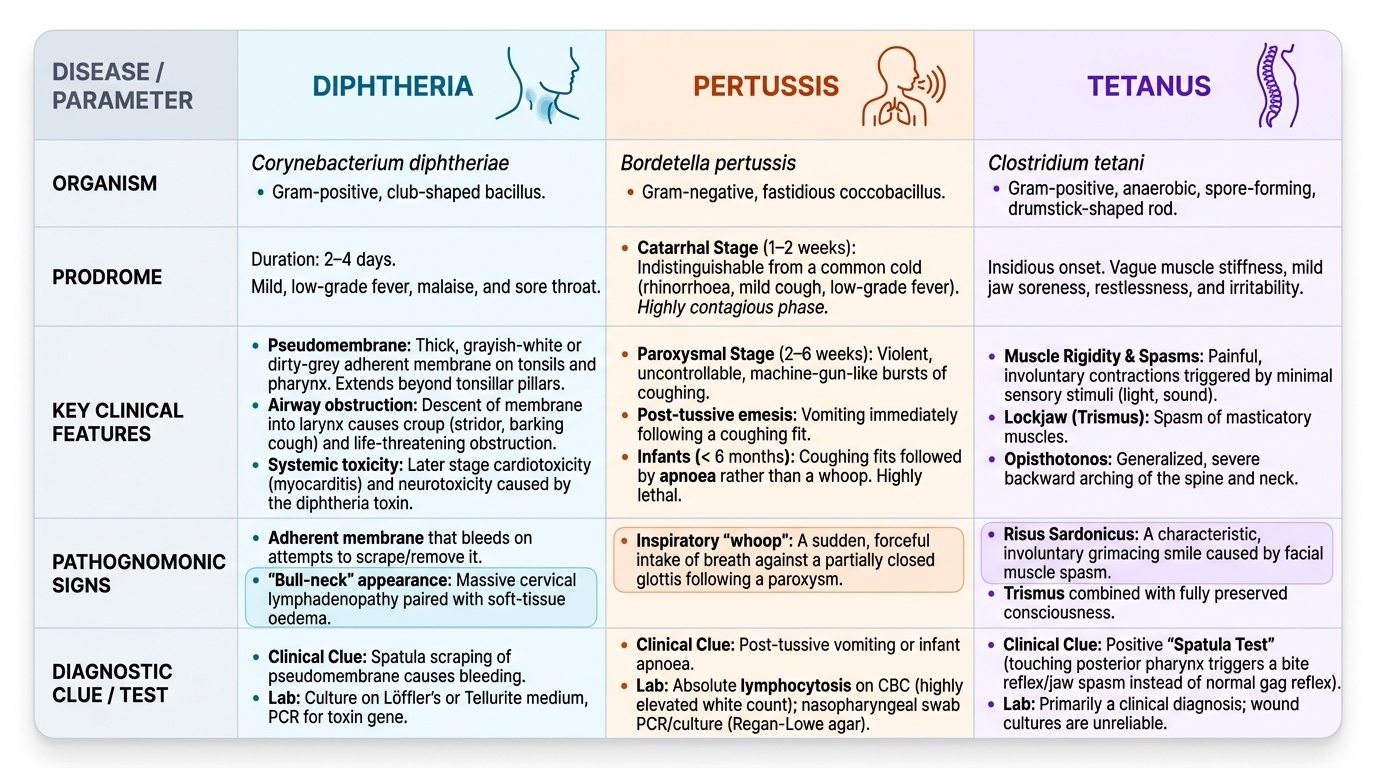
Each of the three diseases has a distinctive clinical signature shaped by the specific toxin or pathogen mechanism at work — recognising these signatures early is the key to preventing irreversible complications.
Provided image
Diphtheria presents with a 2–4-day prodrome of low-grade fever, malaise, and sore throat. The hallmark finding is a pseudomembrane — a thick, grayish-white or dirty-grey adherent membrane on the tonsils and posterior pharynx that extends beyond the tonsillar pillars (unlike the membrane of tonsillitis, which stays within the pillars). When you try to remove the membrane with a spatula, it bleeds — this adherence and bleeding-on-removal distinguishes it from streptococcal exudates. The voice becomes muffled or has a characteristic 'hot potato' quality. Extension of the membrane downward into the larynx causes croup (barking cough, stridor) and life-threatening airway obstruction; extension into the nose causes a blood-stained nasal discharge. Massive cervical lymphadenopathy combined with soft-tissue oedema produces the bull-neck appearance — a sign of severe pharyngeal diphtheria. The child is typically not as severely systemically unwell as you would expect from the alarming local findings, until toxin-mediated systemic effects (cardiac, neurological) supervene.
Pertussis (whooping cough) passes through three distinct phases. The catarrhal stage (1–2 weeks) is indistinguishable from a common cold — low-grade fever, rhinorrhoea, mild cough — during which the child is most contagious. The paroxysmal stage (2–6 weeks) is diagnostic: violent, uncontrollable, machine-gun bursts of coughing (a 'paroxysm') followed by a sudden, forceful inspiratory effort against a partially closed glottis, producing the characteristic high-pitched 'whoop'. The child may turn cyanotic or blue during the paroxysm and often vomits at the end. In infants under 6 months — who lack the muscular strength and airway geometry to generate the whoop — the presentation is subtly different: paroxysmal coughing followed by apnoea rather than a whoop. This is the highest-risk group, with apnoea as the leading cause of death. A lymphocytosis on blood count (often >15,000 lymphocytes/µL, sometimes >50,000/µL) is a characteristic but non-specific finding. The convalescent stage (weeks to months) sees gradually diminishing cough severity.
Tetanus presents with a variable incubation period (3 days to 3 weeks, average 8 days) from the time of injury. The shorter the incubation, the more severe the disease. Trismus (lockjaw) — inability to open the mouth due to masseter spasm — is usually the first sign, followed by risus sardonicus (a fixed, sardonic grin from facial muscle spasm). As toxin spreads, generalised spasms occur: the patient arches into opisthotonus (hyperextension of the back, with neck and back rigidly arched) triggered by any sensory stimulus — touch, light, noise. Between spasms, consciousness is fully preserved — the patient is aware and terrified. Autonomic instability (tachycardia, hypertension, sweating, hyperthermia) develops in severe cases. Neonatal tetanus affects the neonate from day 3 to day 28 of life (the WHO case definition requires the neonate to have cried and suckled normally at birth, then developed rigidity and inability to feed); it results from contaminated cord cutting or dressing in a baby of a non-immunised mother.
SELF-CHECK
A 3-month-old infant presents with 2 weeks of paroxysmal coughing without a whoop. The blood count shows WBC 28,000/µL with 80% lymphocytes. Which diagnosis is MOST likely, and why is the whoop absent?
A. Diphtheria — the membrane is obstructing airflow
B. Pertussis — young infants lack the muscular strength and airway geometry to generate a whoop; they present with apnoea instead
C. Viral croup — lymphocytosis is characteristic
D. Tuberculosis — lymphocytosis is the key finding
Reveal Answer
Answer: B. Pertussis — young infants lack the muscular strength and airway geometry to generate a whoop; they present with apnoea instead
Pertussis in infants under 6 months typically does NOT produce the classic whoop — they lack the respiratory muscle strength and the airway geometry required to generate the forceful inspiratory manoeuvre that creates the sound. Instead, they present with paroxysmal coughing followed by apnoea, which is the leading cause of death in this age group. The marked lymphocytosis (lymphocyte count often >15,000/µL, here 22,400/µL) is highly characteristic of pertussis — the pertussis toxin blocks lymphocyte recirculation. A 3-month-old with paroxysmal cough + lymphocytosis must be presumed to have pertussis until proven otherwise.
Pathogenesis and Aetiology
The pathogenesis of each disease is driven by a specific toxin or virulence factor, and understanding the mechanism directly predicts the clinical features and explains why antitoxin — not just antibiotics — is the cornerstone of treatment for both diphtheria and tetanus.
Diphtheria toxin is encoded by a bacteriophage (beta-phage) that infects Corynebacterium diphtheriae; toxigenic strains that carry this phage cause disease while non-toxigenic strains do not. The toxin consists of two fragments: the B (binding) fragment attaches to cell-surface receptors and facilitates entry; the A (active) fragment enters the cytoplasm and catalyses the ADP-ribosylation of elongation factor-2 (EF-2), irreversibly halting protein synthesis. This causes cell death — explaining the necrosis that forms the pseudomembrane, and the myocarditis and neuropathy seen later. The pseudomembrane itself is a coagulum of fibrin, dead cells, bacteria, and inflammatory debris — its adherence makes physical removal dangerous (it bleeds and can dislodge into the airway). Toxin absorbed into the bloodstream affects two distant organs: the heart (myocarditis — onset 1–2 weeks post-disease) and peripheral nerves (demyelinating neuropathy — onset weeks to months post-disease).
Pertussis toxin (PT) is Bordetella pertussis's master virulence factor. PT inhibits adenylyl cyclase pathway signalling in phagocytes, impairing neutrophil and macrophage function and preventing bacterial killing. PT also blocks lymphocyte traffic from lymph nodes into the bloodstream by inhibiting chemokine receptors — this is the molecular basis of the striking lymphocytosis in pertussis. Additional virulence factors include filamentous haemagglutinin (adhesin for attachment to respiratory cilia), tracheal cytotoxin (destroys ciliated epithelium, impairing mucociliary clearance), and adenylate cyclase toxin (impairs macrophage function). The combination of ciliary destruction, mucus accumulation, and heightened bronchial reactivity drives the violent coughing paroxysms that persist long after the organism is cleared — hence the persistent cough in the convalescent stage even after antibiotic treatment.
Tetanospasmin (tetanus toxin) is produced by Clostridium tetani in anaerobic conditions (deep wounds, contaminated cords). The toxin travels retrogradely along motor nerve axons from the wound site to the spinal cord and brainstem, where it is taken up by inhibitory interneurons (Renshaw cells). Tetanospasmin cleaves synaptobrevin (a SNARE protein), blocking the release of glycine and GABA — the inhibitory neurotransmitters of the ventral horn. With inhibitory control removed, alpha-motor neurons fire unopposed in response to any afferent stimulus, producing the characteristic generalised rigidity and spasms. The autonomic nervous system is also affected — sympathetic hyperactivity causes the tachycardia, hypertension, and sweating that may prove fatal in severe tetanus.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
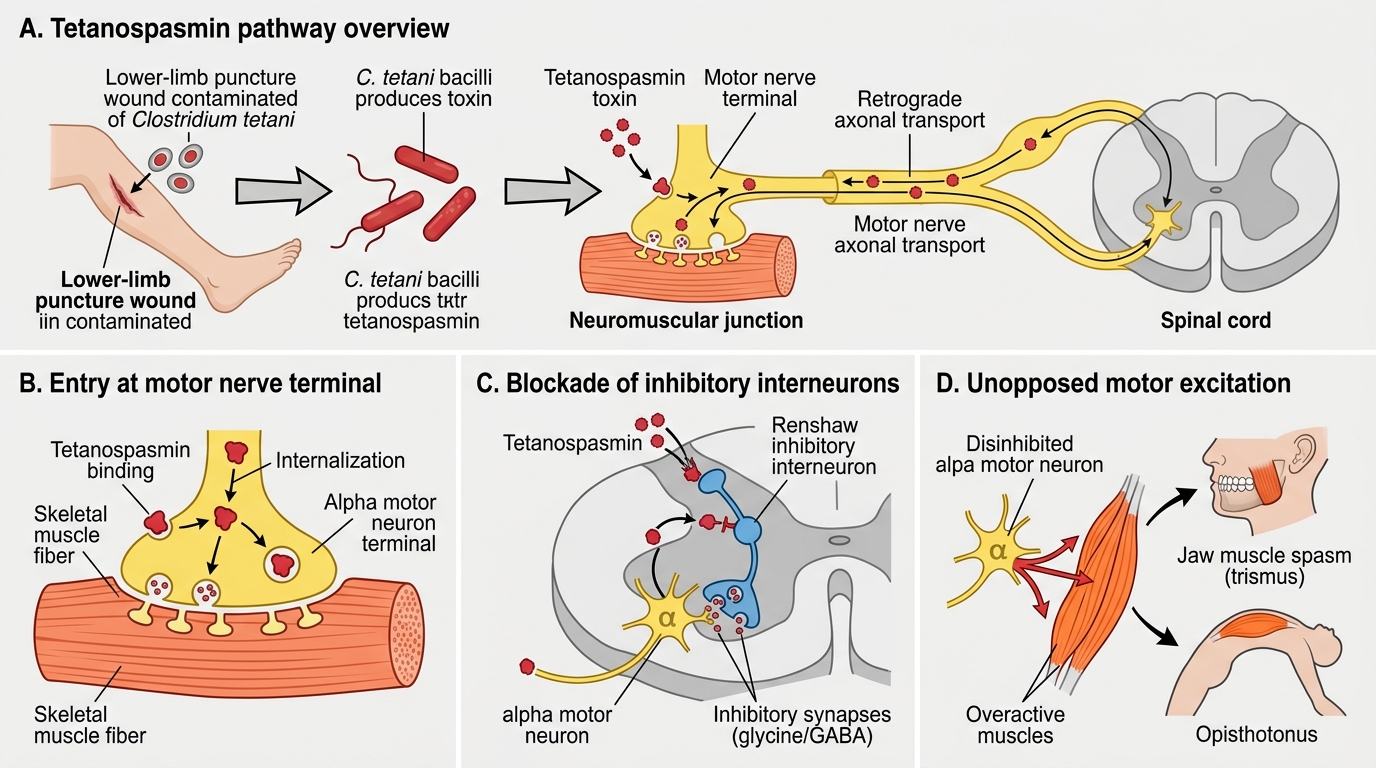
Tetanospasmin Pathway in Tetanus
Diagnosis and Investigation
All three diseases are primarily clinical diagnoses — the speed and severity of these illnesses means treatment must begin on clinical grounds without waiting for laboratory confirmation. Investigations serve to confirm the diagnosis for public health purposes, identify complications, and guide management.
Diphtheria is diagnosed clinically by the finding of an adherent grayish pseudomembrane beyond the tonsillar pillars, with or without bull-neck appearance, in an incompletely vaccinated child. Throat and nasopharyngeal swabs for culture on Loeffler's serum slope or tellurite agar (selective media that produce black colonies from diphtheria) provide bacteriological confirmation. Toxigenicity is confirmed by the Elek test (immunodiffusion to demonstrate toxin production) or PCR for the diphtheria toxin gene (tox gene). Crucially, antitoxin must be given on clinical grounds without waiting for culture results — delay is lethal. An ECG should be performed to detect early myocarditis (prolonged PR interval, ST changes, heart block).
Pertussis is diagnosed clinically in the paroxysmal stage by the characteristic cough + whoop (or apnoea in infants). Laboratory confirmation uses:
- Nasopharyngeal culture on Bordet-Gengou medium or Regan-Lowe medium — most sensitive in the catarrhal and early paroxysmal stage; sensitivity drops sharply after 3 weeks of illness or antibiotic exposure
- PCR of nasopharyngeal aspirate — more sensitive than culture, positive for longer into the illness
- Blood count: absolute lymphocytosis (often >15,000/µL, can reach 50,000–100,000/µL in severe infant disease) is highly characteristic
- Serology (anti-pertussis toxin IgG): used for epidemiological confirmation in older patients
Tetanus is a clinical diagnosis — there is no diagnostic laboratory test. The diagnosis rests on:
- Finding trismus + risus sardonicus + opisthotonus in a patient with a history of a wound (or a neonate with home delivery and contaminated cord)
- Preserved consciousness between spasms (distinguishing tetanus from seizure disorders)
- Absence of vaccination history or uncertain immunisation status
- The spatula test — touching the posterior pharynx with a tongue depressor; in tetanus the patient reflexively bites the spatula (involuntary masseter contraction) rather than gagging; reported high sensitivity/specificity in resource-limited settings
- Blood counts and metabolic tests are normal (tetanus toxin causes neurological, not systemic inflammatory disease)