Page 17 of 32
PE31.11 | Diphtheria Pertussis Tetanus — SDL Guide (Part 2)
Complications
The complications of diphtheria, pertussis, and tetanus are toxin-driven rather than directly caused by the bacteria themselves — making it possible to predict and monitor for them systematically once the diagnosis is made. Each disease has a distinct complication timeline that guides follow-up intensity and determines which investigations must be ordered proactively rather than reactively. In diphtheria, the risk of myocarditis and neuropathy persists weeks after the local throat infection has resolved, demanding prolonged monitoring even when the child appears to have recovered. In pertussis, the greatest danger is in the youngest infants who cannot signal distress by generating a whoop, but who silently stop breathing during a paroxysm. In tetanus, the risk of fatal respiratory failure from laryngospasm and the unpredictable sympathetic-parasympathetic surges of autonomic instability demand continuous ICU vigilance. Anticipating these complications — not just treating them when they arrive — is the standard of care for all three diseases.
Diphtheria complications arise from toxin spread to distant organs:
- Myocarditis — occurs in 10–25% of pharyngeal diphtheria cases, typically at 1–2 weeks after disease onset. Manifests as arrhythmias (heart block, bundle branch block, ventricular arrhythmia), cardiac failure, and sudden death. It is the most common cause of death in diphtheria. Monitoring requires serial ECGs and cardiac enzymes. The risk is higher with severe pharyngeal or laryngeal disease
- Neuropathy — delayed complication at weeks to months post-disease. Early neuropathy: palatal palsy (nasal voice, regurgitation through nose) at 2–3 weeks; ciliary palsy causing blurred vision (loss of accommodation) at 4–5 weeks; facial nerve palsy. Late neuropathy: peripheral motor neuropathy (Guillain-Barré-like) at 5–8 weeks post-disease, causing limb weakness
- Airway obstruction — pseudomembrane extending into the larynx and trachea can cause respiratory distress and asphyxia; emergent airway management (intubation or tracheotomy) may be needed
- Septicaemia and secondary bacterial infections — rare
Pertussis complications are most severe and most common in infants under 6 months:
- Apnoea — the most feared complication in young infants; may be the only presentation without the cough paroxysm, requiring monitoring in hospital
- Pneumonia — secondary bacterial (Staphylococcus, Streptococcus) or primary pertussis pneumonia; most common cause of death in older children
- Encephalopathy — rare but serious; manifests with seizures and altered consciousness, possibly from hypoxia or toxin effect
- Subconjunctival haemorrhage, epistaxis, hernias — from the pressure generated during violent coughing paroxysms
- Malnutrition — from persistent vomiting after coughing and poor intake
- Secondary Staphylococcal otitis media
Tetanus complications are predominantly from uncontrolled spasms and autonomic instability:
- Respiratory failure — laryngospasm or sustained opisthotonus causing asphyxia; the primary cause of death in unventilated patients
- Autonomic instability — sympathetic surges causing tachycardia, hypertension, diaphoresis, hyperthermia; parasympathetic bursts causing bradycardia and hypotension; extremely difficult to manage and carries high mortality
- Aspiration pneumonia — from inability to swallow and impaired airway protection
- Rhabdomyolysis and vertebral fractures — from violent sustained muscle spasms
- Pressure sores and DVT — from prolonged immobility in the ICU
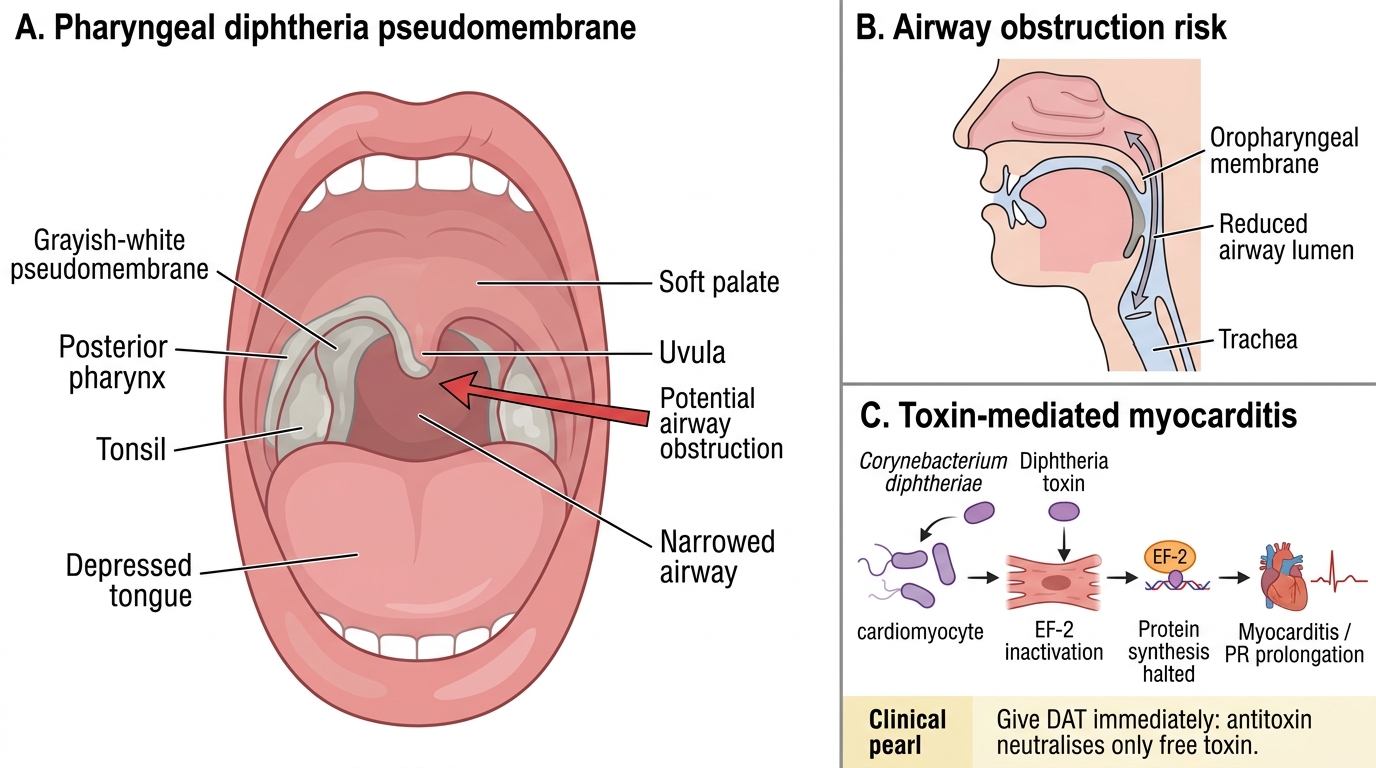
Diphtheria Pseudomembrane and Major Complications
CLINICAL PEARL
In diphtheria, do NOT wait for culture results before giving antitoxin — clinical diagnosis is sufficient and delay is lethal. The diphtheria antitoxin (DAT) neutralises only free (unbound) toxin; once toxin has bound to cell receptors in the heart or nervous system, antitoxin has no effect. The earlier antitoxin is given, the more toxin it can neutralise. Additionally, always do a skin test for horse-serum hypersensitivity before giving DAT (it is an equine-derived product) — if positive, desensitisation is required. Similarly, in tetanus, tetanus immunoglobulin (TIG) must be given at diagnosis, not after spasms escalate.
SELF-CHECK
A 7-year-old with pharyngeal diphtheria (confirmed pseudomembrane, bull-neck) develops a prolonged PR interval on ECG on day 10 of illness. What complication has occurred, and which specific mechanism caused it?
A. Hypokalaemia from vomiting causing ECG changes
B. Diphtheria myocarditis from toxin-mediated ADP-ribosylation of EF-2 in cardiomyocytes, halting protein synthesis
C. Viral myocarditis as a coincidental infection
D. Autoimmune pericarditis from immune complex deposition
Reveal Answer
Answer: B. Diphtheria myocarditis from toxin-mediated ADP-ribosylation of EF-2 in cardiomyocytes, halting protein synthesis
Diphtheria myocarditis occurs in 10–25% of pharyngeal diphtheria cases, typically at 1–2 weeks post-disease onset. The diphtheria toxin's A fragment ADP-ribosylates elongation factor-2 (EF-2), irreversibly blocking protein synthesis in cardiomyocytes. This causes myocardial cell death, manifesting as arrhythmias (prolonged PR, bundle branch block, ventricular arrhythmia), and is the most common cause of death in diphtheria. ECG monitoring should be initiated from diagnosis and continued for several weeks. Treatment is largely supportive — antitoxin given early can prevent cardiac toxin binding, but once myocarditis is established, management is supportive.
Management and Prevention
Management of each disease requires rapid initiation of toxin-neutralising therapy (antitoxin or immunoglobulin) alongside antibiotics to eliminate the organism and supportive care to manage complications. The three diseases demand different specific treatments and illustrate three distinct therapeutic principles: antitoxin before culture confirmation (diphtheria), antibiotic for infectivity reduction (pertussis), and immunoglobulin plus anti-spasmodic plus antibiotic (tetanus). A critical shared principle across diphtheria and tetanus is that the antitoxin or immunoglobulin must be given as early as possible — these agents neutralise only free, circulating toxin, and once toxin has bound to cardiac or neural tissue, no amount of antitoxin can reverse the damage. This makes clinical recognition the rate-limiting step in saving the child's life: the laboratory exists to confirm, not to permit treatment. In pertussis, by contrast, antibiotics given early (catarrhal stage) can prevent the paroxysmal illness entirely, but given in the paroxysmal stage, they only reduce infectivity — the bronchial hyperreactivity driving the cough is already established and will resolve only over weeks to months. Understanding this therapeutic timing logic for each disease is as important as knowing the correct drug and dose.
Diphtheria management:
Step 1 — Diphtheria Antitoxin (DAT): Administer immediately on clinical suspicion — do NOT wait for culture.
- Dose depends on severity, site, and duration of membrane:
- Tonsillar: 20,000–40,000 IU
- Pharyngeal/laryngeal: 40,000–60,000 IU
- Combined nasopharyngeal: 80,000–100,000 IU
- Late presentation (>3 days) or severe disease: up to 100,000 IU
- Route: IV preferred for severe disease; IM for mild/moderate
- Always perform a skin/conjunctival sensitivity test (horse serum) before giving; if positive, desensitise
Step 2 — Antibiotics: To eliminate the organism (reduces communicability; does NOT replace antitoxin)
- Procaine penicillin G 25,000–50,000 IU/kg/day IM for 14 days, OR
- Erythromycin 40–50 mg/kg/day orally for 14 days (for penicillin-allergic patients)
Step 3 — Supportive care: Airway monitoring (nurse in ICU if laryngeal involvement), cardiac monitoring (serial ECG), bed rest for 4–6 weeks if myocarditis develops, treatment of arrhythmias.
Step 4 — Isolation: Respiratory isolation; contacts receive prophylactic erythromycin or penicillin; close contacts with uncertain vaccination status receive booster dose.
Pertussis management:
Antibiotics (reduce infectivity, not cough duration once paroxysmal stage established):
- Azithromycin 10 mg/kg/day (max 500 mg) for 5 days — preferred for infants and children
- Clarithromycin 15 mg/kg/day in 2 divided doses for 7 days (alternative)
- Erythromycin 40–50 mg/kg/day for 14 days (older alternative, less tolerated)
- Trimethoprim-sulfamethoxazole for macrolide-intolerant patients
Supportive care:
- Infants under 6 months: admit for monitoring (apnoea risk); oxygen, suction, minimal stimulation to reduce paroxysm triggering
- Nutritional support (small, frequent feeds after coughing paroxysms to reduce vomiting)
- Humidified oxygen for hypoxic episodes
- Avoid cough suppressants (not effective, may suppress vital reflex)
Contacts: post-exposure prophylaxis with azithromycin for household contacts, especially infants and pregnant women in third trimester.
Tetanus management:
Step 1 — Wound care: Debride the wound thoroughly; remove dead tissue and foreign bodies to eliminate anaerobic conditions; hydrogen peroxide irrigation.
Step 2 — Tetanus Immunoglobulin (TIG):
- Human TIG (preferred): 3,000–10,000 IU IM at diagnosis
- Infiltrate part of the dose around the wound
- If human TIG unavailable: equine antitetanus serum 10,000–20,000 IU after skin sensitivity testing
Step 3 — Antibiotics: To eliminate C. tetani from the wound
- Metronidazole 30 mg/kg/day (max 4 g/day) in 4 divided doses for 7–10 days — preferred
- Penicillin G 100,000 IU/kg/day (alternative)
Step 4 — Anti-spasmodics: To control muscle spasms
- Diazepam 0.1–0.3 mg/kg IV per spasm episode (PRN) and/or scheduled dosing for background control
- Severe cases: baclofen (intrathecal), magnesium sulphate, neuromuscular blockade with mechanical ventilation in ICU
- Minimise sensory stimuli (quiet, dark room)
Step 5 — Supportive ICU care: Mechanical ventilation for respiratory failure or severe spasms; management of autonomic instability (labetalol, morphine for sympathetic surges; atropine for bradycardia).
Vaccination after recovery: Tetanus does NOT confer immunity — survivors must complete the vaccination course, as disease levels of toxin are insufficient to generate protective immunity.
Prevention — National Immunization Schedule (India):
- Pentavalent vaccine (DPT + HepB + Hib): at 6, 10, and 14 weeks of age
- DPT booster: at 16–24 months and again at 5–6 years
- TT (tetanus toxoid) for pregnant women: 2 doses in pregnancy (TT-1 as early as possible; TT-2 at least 4 weeks later; if previously immunised, booster TT)
- Three doses of DPT provide >95% protection against diphtheria and tetanus; protection against pertussis wanes after 4–12 years, explaining resurgence
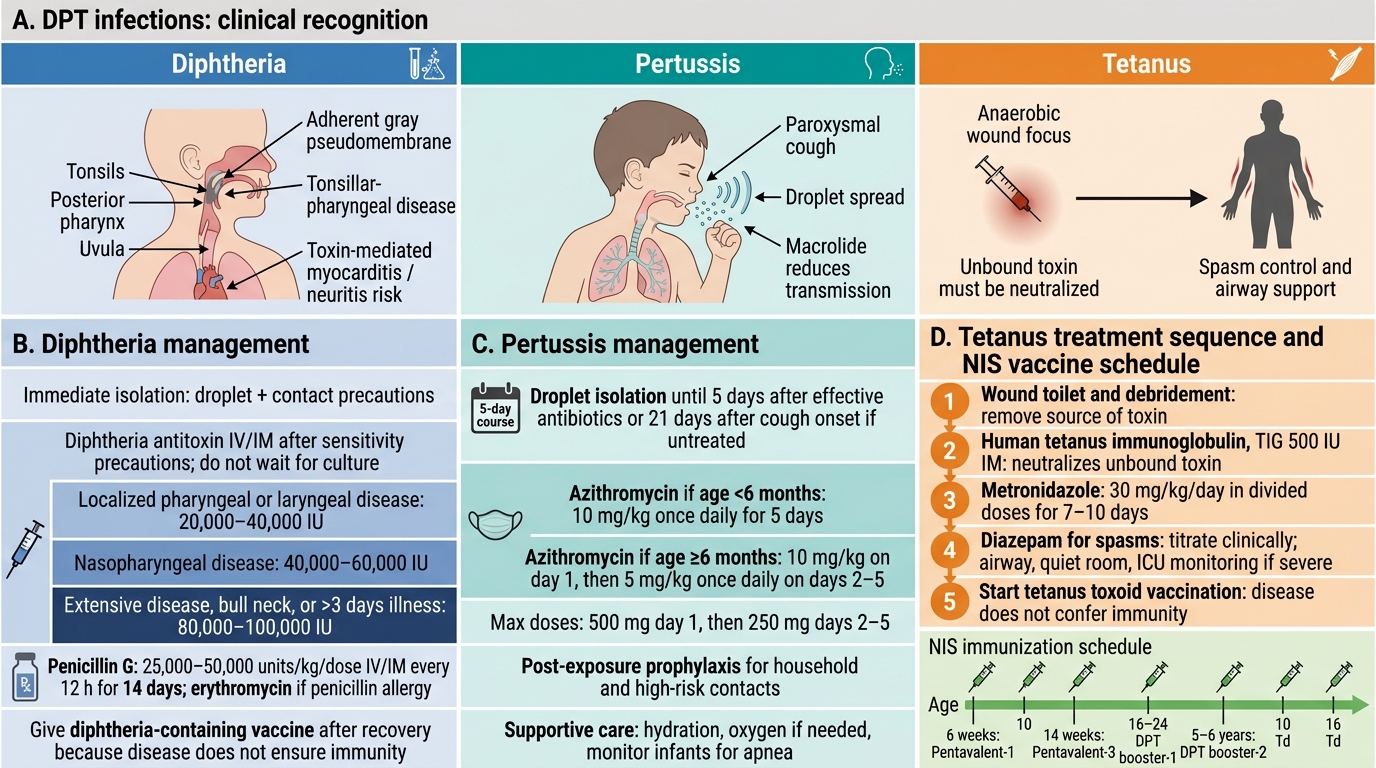
Management of Diphtheria, Pertussis, Tetanus and DPT Immunization Schedule
Self-Assessment — DPT Infections
The following clinical scenarios require you to integrate your knowledge across the three diseases covered in this module. For each case, focus not only on naming the diagnosis but on the specific management steps — doses, timing, and the reasoning behind each decision. Effective management of these diseases demands not just knowing the correct drug but understanding why each element of the treatment protocol exists and what the consequences of delay or omission are. In diphtheria, the antitoxin dose varies with disease severity and site; in pertussis, the antibiotic choice differs by age and allergies; in tetanus, the sequence — wound care, then immunoglobulin, then antibiotics, then spasm control — reflects the pathophysiological logic of stopping toxin at its source before addressing its systemic effects. Work through each case as you would in a real clinical encounter: identify the disease, recall its mechanism, choose the specific intervention, and justify the timing.
Case 1: A 6-year-old unvaccinated boy presents with a 3-day history of low-grade fever, sore throat, and hoarseness. Examination shows a grayish membrane covering both tonsils and extending to the posterior pharynx and uvula; attempting to remove it causes bleeding. His neck is swollen bilaterally.
Questions:
- What is the diagnosis, and what is the clinical term for the neck finding?
- Should you wait for culture results before giving diphtheria antitoxin? Justify your answer.
- What is the most likely cause of death in this child if not treated urgently?
Case 2: A 6-week-old infant is brought in with 3 weeks of paroxysmal coughing. The coughs occur in bursts and are followed by a period of not breathing (apnoea), without any whoop. Blood count shows WBC 35,000/µL, 85% lymphocytes. He is not vaccinated as his first vaccine was due next week.
Questions:
- What is the most likely diagnosis, and what is the first-line antibiotic and dose?
- Why does this infant have apnoea instead of the classic whoop?
- What monitoring is required during hospitalisation?
Case 3: A 12-day-old neonate delivered at home presents with difficulty feeding for 1 day, and now has a clenched jaw and body stiffness triggered by touch. The mother has had no antenatal care and her vaccination status is unknown.
Questions:
- What is the diagnosis? What is the portal of entry for the toxin?
- List the specific management steps in order of priority.
- What measure during antenatal care would have prevented this condition?
SELF-CHECK
A child with tetanus is receiving diazepam for spasms. His heart rate suddenly rises to 160/min with blood pressure 180/110 mmHg and profuse sweating. What is the most likely explanation for this change?
A. Diazepam overdose causing paradoxical sympathetic activation
B. Autonomic instability — sympathetic hyperactivity from tetanospasmin affecting the autonomic nervous system
C. Secondary bacterial septicaemia from the original wound
D. Anaphylaxis to the tetanus immunoglobulin given earlier
Reveal Answer
Answer: B. Autonomic instability — sympathetic hyperactivity from tetanospasmin affecting the autonomic nervous system
Autonomic instability is one of the most dangerous complications of severe tetanus, occurring as tetanospasmin affects the autonomic nervous system in addition to the somatic motor system. Sympathetic surges produce tachycardia, hypertension, profuse sweating, and hyperthermia — alternating with parasympathetic surges causing bradycardia and hypotension. This autonomic lability is a major cause of death in ICU-managed tetanus patients. Management includes morphine, labetalol, or magnesium sulphate to blunt sympathetic surges, and atropine for bradycardic episodes. It is important to distinguish these surges from sepsis or anaphylaxis.