Page 25 of 32
PE31.14 | Parasitic Infections — SDL Guide
Learning Objectives
- Enumerate the common parasitic infections causing fever and gastrointestinal illness in children
- Describe the etiopathogenesis, clinical features, and complications of soil-transmitted helminths (Ascaris, hookworm, Enterobius, Trichuris), intestinal protozoa (Giardia, Entamoeba histolytica), visceral leishmaniasis, lymphatic filariasis, and neurocysticercosis
- Select appropriate diagnostic investigations for each parasitic infection
- Outline management including correct albendazole dosing by age, the dual-agent protocol for amoebiasis, and public health measures including the National Deworming Day programme
INSTRUCTIONS
Parasitic infections collectively account for a substantial burden of childhood morbidity in India, causing chronic malnutrition, anaemia, growth faltering, and — in the case of neurocysticercosis — epilepsy. Most infections are preventable through WASH (water, sanitation, hygiene) improvements and periodic deworming. As a final-year student, you are expected not only to recognise the clinical picture but also to counsel families, prescribe weight-based treatment correctly, and situate individual case management within India's national control programmes.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 11 — Parasitic Infections (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Sections on Intestinal Parasites and Leishmaniasis (textbook)
- WHO Guidelines for Preventive Chemotherapy in Human Helminthiasis, 2023 (guideline)
- India National Deworming Day (NDD) Programme Guidelines, MoHFW 2022 (programme)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old boy from a rural district in Bihar is brought by his mother with a 3-month history of poor weight gain, intermittent loose stools, and pallor. She reports he eats mud occasionally (pica). His haemoglobin is 7.2 g/dL with microcytic-hypochromic pattern. Stool examination reveals hookworm ova. Meanwhile, his 5-year-old sister is brought in the same visit complaining of intense perianal itching at night; you ask for a cellophane-tape test. The district health officer has just launched the National Deworming Day campaign — you wonder whether the family missed it. What organisms are you dealing with, how do they differ in mechanism of harm, and what is the correct treatment for each child?
WHY THIS MATTERS
India carries one of the highest global burdens of soil-transmitted helminthiasis (STH), with an estimated 220 million children at risk. Parasitic infections are a leading cause of nutritional anaemia, stunting, and cognitive impairment in school-age children — consequences that are invisible on a single clinical encounter but devastating across childhood. Diseases like kala-azar (visceral leishmaniasis) are targeted under the National Vector Borne Disease Control Programme (NVBDCP) for elimination, yet remain endemic in Bihar, Jharkhand, West Bengal, and Eastern UP. Neurocysticercosis (NCC) is the most common cause of acquired epilepsy in South Asia. Mastering this topic means you can prevent irreversible sequelae, prescribe the correct drug at the correct dose, and contribute to national elimination goals — all in a 10-minute outpatient consultation.
RECALL
Before proceeding, consolidate the following from Year 1 and early Year 3:
- Life cycles: most helminths have a faeco-oral transmission chain; hookworm additionally penetrates skin. Soil-contaminated environments are the vector for STH.
- Iron physiology: dietary iron absorption in the duodenum (non-haem iron reduced to Fe²⁺ by gastric acid); hookworm causes both malabsorption of iron and direct intestinal blood loss → microcytic-hypochromic iron-deficiency anaemia.
- Immune response to helminths: Th2 polarisation with IL-4, IL-5, IL-13; IgE-mediated mast-cell/eosinophil recruitment; peripheral blood eosinophilia (>500 cells/µL) is the hallmark of invasive helminthic disease — not protozoa (which cause eosinopenia or normal eosinophil counts).
- Malnutrition criteria (SAM): weight-for-height < −3 SD, MUAC <11.5 cm in 6–59-month-olds, or bilateral pedal oedema — parasitic infections both worsen and are worsened by malnutrition.
Clinical Presentation of Parasitic Infections
Parasitic infections in children encompass a heterogeneous group of diseases ranging from asymptomatic carriage to life-threatening systemic illness, and the clinician must recognise distinct presentation patterns to guide appropriate investigation. The broad clinical syndromes cluster around four organ systems: the gastrointestinal tract, the haematopoietic system, the lymphatics, and the central nervous system.
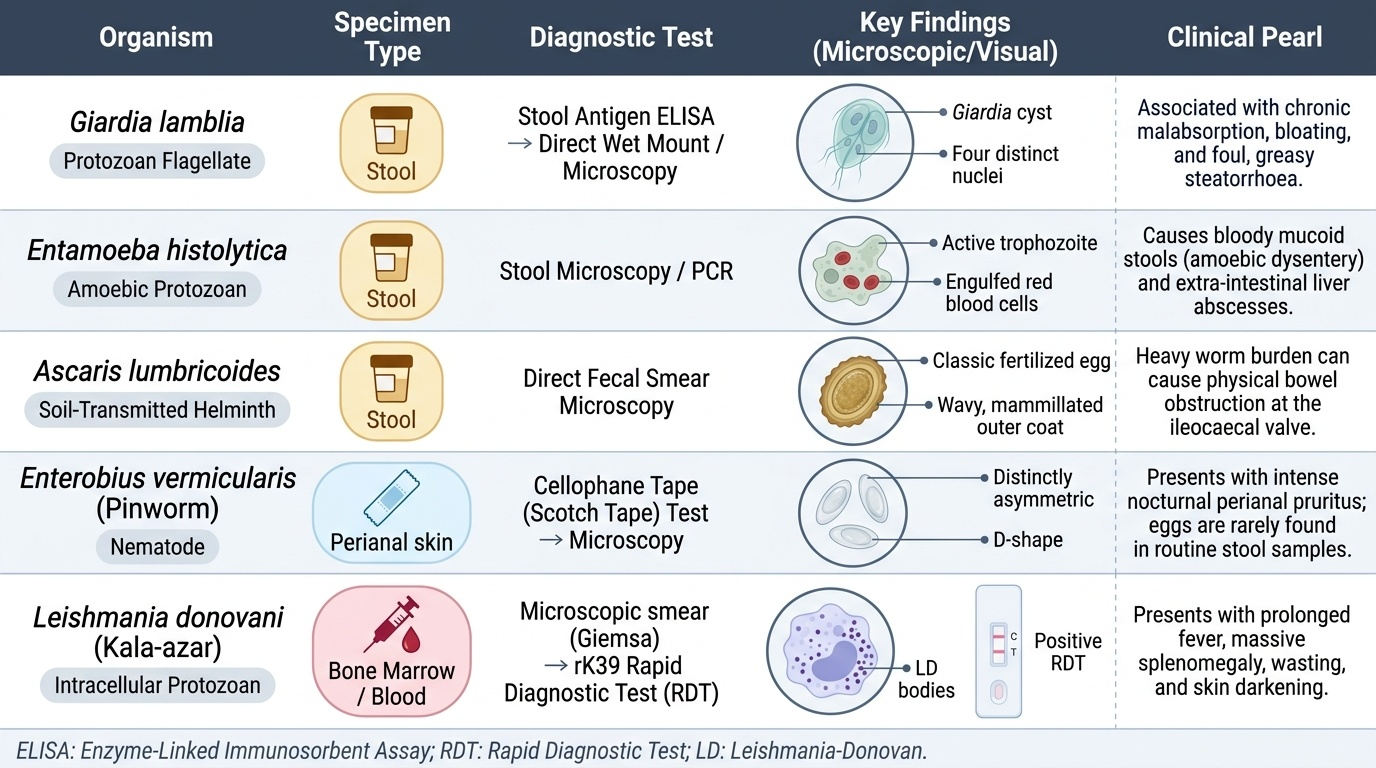
Provided image
Gastrointestinal presentations are the most common entry point. Ascaris lumbricoides infestation is often asymptomatic in light loads, but heavy worm burdens cause colicky abdominal pain, nausea, and — most dangerously — bolus obstruction at the ileocaecal valve, presenting as acute intestinal obstruction with distension and bilious vomiting in a child whose X-ray shows coiled worms. Giardia lamblia produces a characteristic syndrome of chronic malabsorption: foul-smelling, greasy, pale bulky stools (steatorrhoea), bloating, and weight loss without frank dysentery or fever. Entamoeba histolytica classically causes amoebic dysentery — bloody mucoid stools with tenesmus, usually without the high-fever pattern seen in bacterial dysentery (Shigella). Extra-intestinal amoebiasis manifests as amoebic liver abscess — fever, right hypochondrial pain, and tender hepatomegaly; perforation into the pleural or peritoneal space is a surgical emergency. Trichuris trichiura (whipworm) causes bloody diarrhoea and — in heavy infection — rectal prolapse in young children.
Haematological and nutritional presentations: Hookworm infection produces the most clinically significant anaemia of all STH — a progressive microcytic-hypochromic iron-deficiency anaemia from both mucosal blood loss (adult worms bite mucosa and inject anticoagulant) and reduced iron absorption. The child may present with pallor, fatigue, pica (eating clay/soil), and cardiac decompensation in severe cases. Ancylostoma duodenale causes greater blood loss per worm than Necator americanus.
Systemic/febrile presentations: Leishmania donovani (visceral leishmaniasis/kala-azar) presents with prolonged fever (>2 weeks), progressive massive splenomegaly (the spleen may reach the pelvis), hepatomegaly, wasting, and paradoxical skin darkening ("kala-azar" = black fever in Hindi). It is fatal without treatment. Lymphatic filariasis (Wuchereria bancrofti) presents acutely with filarial fever and lymphangitis, and chronically as lymphoedema progressing to elephantiasis of the limbs or genitalia.
Neurological presentations: Taenia solium cysticercosis in the brain (neurocysticercosis, NCC) is the most common cause of acquired epilepsy in India and South Asia. Children present with new-onset focal or generalised seizures; raised intracranial pressure may cause headache, vomiting, and papilloedema when cysts obstruct CSF flow.
IMPORTANT: Pulmonary migration of Ascaris larvae causes Loeffler syndrome (transient pulmonary eosinophilia) — dry cough, low-grade fever, and transient migratory pulmonary infiltrates 4–16 days after infection. This presentation may be confused with pneumonia; the key clue is concurrent eosinophilia and resolution without antibiotics.
| Parasite | Transmission | Key clinical syndrome | Diagnostic clue |
|---|---|---|---|
| Ascaris lumbricoides | Faeco-oral (ova in soil) | Pulmonary migration → Loeffler; intestinal obstruction | Stool microscopy — fertilised ova; X-ray worms |
| Hookworm (Ancylostoma/Necator) | Percutaneous (larval) | Microcytic anaemia, pica, ground-itch | Stool microscopy — ova; low serum ferritin |
| Enterobius vermicularis | Faeco-oral; auto-infection | Perianal itch (nocturnal) | Cellophane-tape test |
| Trichuris trichiura | Faeco-oral | Bloody diarrhoea; rectal prolapse | Barrel-shaped ova in stool |
| Giardia lamblia | Faeco-oral (cysts in water) | Malabsorption, greasy stools | Stool antigen ELISA or microscopy — cysts/trophozoites |
| Entamoeba histolytica | Faeco-oral | Bloody mucoid stools; liver abscess | Erythrophagocytic trophozoites; USG liver |
| Leishmania donovani | Sandfly (Phlebotomus) bite | Prolonged fever + splenomegaly + wasting | rK39 RDT; bone marrow LD bodies |
| Wuchereria bancrofti | Culex mosquito | Filarial fever → lymphoedema | Nocturnal microfilariae in blood |
| Taenia solium (NCC) | Faeco-oral (cysticerci in pork/ova) | Epilepsy; raised ICP | CT head — ring-enhancing cysts; serology |
Pathophysiology and Aetiology
Understanding the life cycle of each parasite is inseparable from understanding how it harms the host; each step in the life cycle corresponds to a distinct pathological mechanism and a potential point of intervention.
Provided image
Ascaris lumbricoides — the great mimic: Infection begins with ingestion of embryonated eggs from soil or contaminated food. In the duodenum, larvae hatch and penetrate the gut wall to enter the portal circulation, travel to the liver, and then the right heart before reaching the pulmonary capillaries. Here they break into the alveoli (the lung-migration phase), ascend the bronchial tree, are swallowed, and mature into adult worms in the jejunum. The lung-migration phase triggers an IgE-mediated hypersensitivity reaction — Loeffler syndrome — characterised by transient migratory infiltrates, eosinophilia, and cough, resolving in 1–2 weeks as larvae depart. Adult worms (15–35 cm long) compete for ingested nutrients and, in heavy infestation, form a worm bolus that obstructs the ileum. Female worms lay 200,000 eggs/day, which are excreted in stool and embryonate in warm moist soil.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
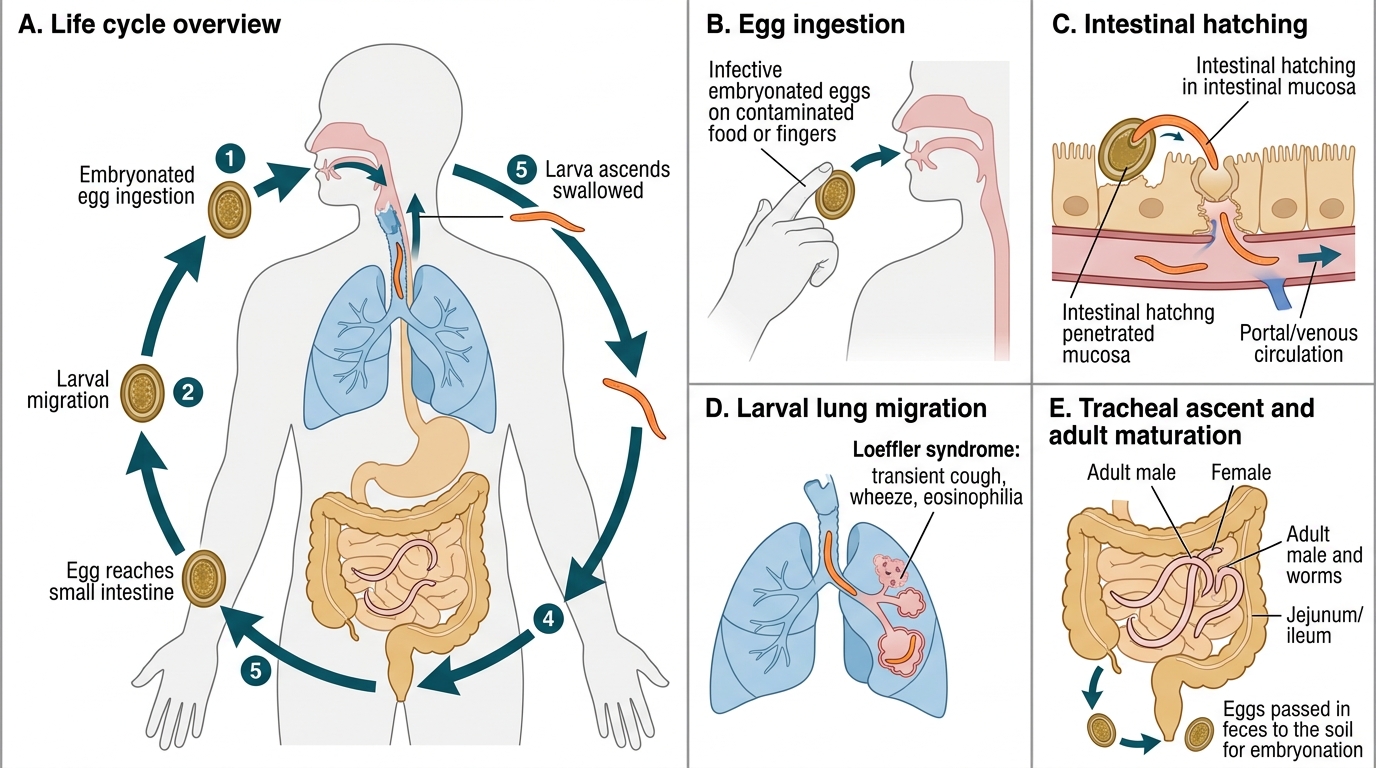
Life Cycle of Ascaris lumbricoides
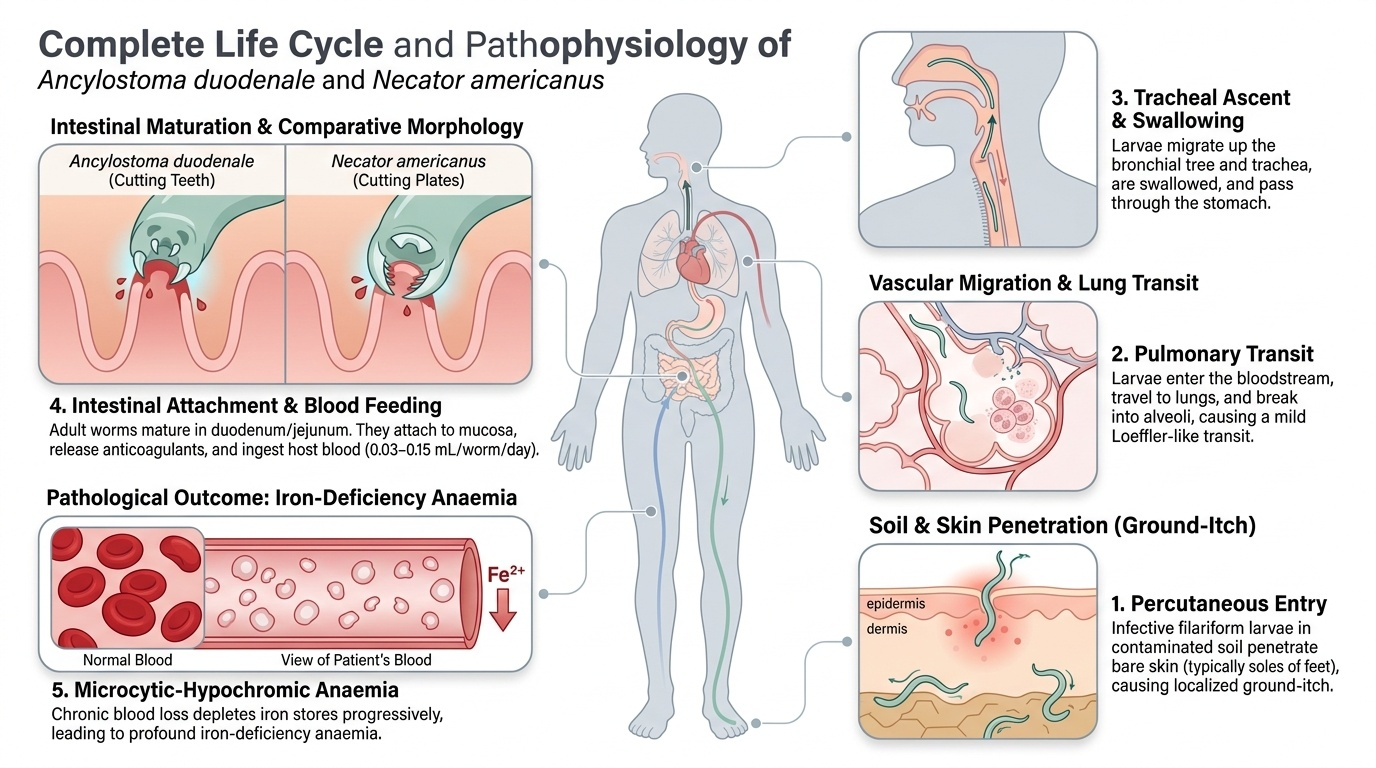
Hookworm — percutaneous and pernicious: Ancylostoma duodenale and Necator americanus larvae live in contaminated soil. Infective filariform larvae penetrate bare skin (typically the soles of the feet), causing a localised ground-itch rash. They enter dermal blood vessels, travel to the lungs (a milder Loeffler-like transit), ascend and are swallowed, and mature in the duodenum and jejunum. Adult worms attach to mucosa with a cutting plate (Ancylostoma) or cutting teeth (Necator), releasing anticoagulants and ingesting 0.03–0.15 mL blood/worm/day. Chronic blood loss exceeds 3 mL/day in heavy infection, depleting iron stores progressively. The combination of blood loss and malabsorption of dietary iron produces profound microcytic-hypochromic iron-deficiency anaemia — the most nutritionally significant consequence of STH globally.
Enterobius vermicularis — nocturnal migratory: The entire life cycle of the pinworm occurs within the human gastrointestinal tract and perianal skin; there is no soil stage. Gravid females migrate at night from the caecum to the perianal skin and deposit eggs, causing intense nocturnal perianal pruritus. Scratching transfers eggs to fingernails, leading to autoinfection and household spread. The eggs are infective within hours of deposition. School-age children are most commonly affected, and entire families often need simultaneous treatment.
Giardia lamblia — the malabsorber: Cysts ingested from contaminated water or food excyst in the duodenum into trophozoites that colonise the small bowel mucosa using a ventral adhesive disc. They do NOT invade the mucosa (hence no blood in stool, no fever) but cause brush-border enzyme deficiency, reduced bile-salt absorption, and villous blunting — producing malabsorption syndrome with fat and fat-soluble-vitamin deficiency, D-xylose malabsorption, and failure to thrive. The pathognomonic clinical picture is chronic pale, bulky, foul-smelling stools with bloating and flatulence.
Entamoeba histolytica — invasion and dissemination: The infective cyst form is ingested faeco-orally. In the caecum and ascending colon, trophozoites emerge and invade the colonic mucosa using proteolytic enzymes (cysteine proteases, amoebapores), producing flask-shaped ulcers that bleed — causing the classic bloody mucoid dysentery. Trophozoites reaching the portal venules travel to the liver, where they liquefy hepatic parenchyma via the same enzymes, producing a single, right-lobe, anchovy-sauce pus amoebic liver abscess. The abscess pus is actually lysed hepatocytes, not true pus. Only ~10% of infected individuals develop invasive disease; the majority are asymptomatic cyst passers.
Leishmania donovani — intracellular parasite of the reticuloendothelial system: The promastigote form is injected by the female sandfly (Phlebotomus argentipes in India). After phagocytosis by macrophages, promastigotes transform into amastigotes (Leishman-Donovan bodies, LD bodies) that multiply within cells of the reticuloendothelial system — spleen, liver, bone marrow, lymph nodes. Splenomegaly results from macrophage hyperplasia and accumulation of parasitised cells; bone marrow replacement causes pancytopenia. Immune suppression from macrophage dysfunction predisposes to secondary infections (TB, pneumonia) which are a frequent cause of death.
Neurocysticercosis (NCC) — Taenia solium: Humans become definitive hosts (tapeworm in intestine) after eating undercooked infected pork. Humans become accidental intermediate hosts (cysticercosis in tissues) after ingesting T. solium eggs from faecally contaminated food or — critically — from an intestinal tapeworm carrier in the household (autoinfection or heteroinfection). Eggs hatch in the intestine, larvae penetrate the gut wall, and are carried haematogenously to the brain (most common), eye, muscle, and subcutaneous tissue. In the brain, living cysts suppress local immunity and may be asymptomatic for years. Death or calcification of cysts triggers an intense inflammatory response that causes seizures and raised ICP. NCC is classified by CT/MRI into stages (vesicular → colloidal → granular-nodular → calcified).
SELF-CHECK
A 6-year-old presents with intermittent cough, low-grade fever, and peripheral eosinophilia of 1800 cells/µL. Chest X-ray shows fleeting bilateral infiltrates that were not present 3 weeks ago. Stool microscopy reveals no ova. What is the most likely explanation?
A. Community-acquired pneumonia due to Streptococcus pneumoniae
B. Loeffler syndrome due to pulmonary larval migration of Ascaris lumbricoides
C. Pulmonary tuberculosis
D. Allergic asthma with eosinophilia
Reveal Answer
Answer: B. Loeffler syndrome due to pulmonary larval migration of Ascaris lumbricoides
Loeffler syndrome is caused by larval migration of Ascaris through the lungs during the second week of infection. Stool may be negative at this stage because adult worms have not yet matured to produce eggs. The triad of transient migratory infiltrates, peripheral eosinophilia, and a child from an endemic area points to this diagnosis. Bacterial pneumonia causes neutrophilia; asthma causes variable airways obstruction without migratory infiltrates; TB rarely causes eosinophilia.
Diagnosis and Investigation
Accurate diagnosis of parasitic infections requires matching the clinical syndrome with the appropriate specimen type and test; the most common error is sending the wrong specimen or missing the optimal timing.
Stool examination is the cornerstone for intestinal helminths and protozoa. A fresh stool sample (processed within 30–60 minutes for protozoa, or preserved in formalin) is examined for: ova (Ascaris — fertilised/unfertilised; hookworm — thin-shelled ova; Trichuris — barrel-shaped bipolar-plugged ova), cysts and trophozoites (Giardia — pear-shaped trophozoites with two nuclei, four flagella, and a ventral disc; cysts with four nuclei), and erythrophagocytic trophozoites (Entamoeba histolytica — pathognomonic finding is a trophozoite actively engulfing red blood cells; E. dispar is morphologically identical but non-pathogenic and does NOT ingest RBCs). A minimum of three stool specimens on alternate days improves sensitivity for intermittent shedders (Giardia). Giardia stool antigen ELISA/rapid test is more sensitive than microscopy and is now preferred in resource-adequate settings.
The cellophane-tape test is the specific diagnostic method for Enterobius vermicularis. A strip of transparent adhesive tape is applied to the perianal skin in the morning BEFORE bathing or defecation, then transferred to a glass slide and examined microscopically for the asymmetrically oval, flat-sided Enterobius ova. Stool examination is insensitive for pinworm because females deposit eggs perianally, not intraluminally.
Blood investigations for systemic parasites:
- Peripheral blood film (thick and thin smears): for malaria (Plasmodium) and nocturnal microfilariae of Wuchereria bancrofti (blood collected at 10 PM–2 AM for highest yield, coinciding with India's Culex mosquito peak-biting time).
- Eosinophilia on CBC: peripheral eosinophilia >500 cells/µL or >5% is characteristic of invasive helminthic infection (tissue-migrating larval phase), particularly Ascaris (Loeffler), hookworm, Toxocara, and filariasis. Protozoa (Giardia, Entamoeba, Leishmania) do NOT cause significant eosinophilia.
- rK39 RDT (rapid card test): a recombinant kinesin antigen immunochromatographic strip test — the first-line field diagnostic for visceral leishmaniasis (kala-azar). Sensitivity ~93–98%, specificity ~97% in India. WHO-endorsed for diagnosis without invasive bone marrow biopsy in endemic areas.
- Bone marrow aspiration from the iliac crest (or splenic aspirate — higher yield but risk): Giemsa stain shows intracellular LD bodies (amastigotes of Leishmania) within macrophages — the definitive morphological diagnosis of kala-azar.
Imaging:
- Ultrasound abdomen: right-lobe, well-defined, hypoechoic lesion ± internal echoes/debris = amoebic liver abscess; free fluid confirms rupture. For Ascaris — worms seen in biliary tree on USG ("four-line sign") in hepatobiliary ascariasis.
- CT head without contrast → with contrast: for NCC, CT shows cysts (hypodense) with ring-enhancing lesion on contrast (colloidal stage, when the cyst wall is degenerating and peri-cyst oedema is present), or calcified punctate lesions (end-stage). MRI is superior for brainstem and small cysts. A perilesional oedema pattern around a solitary ring-enhancing lesion in an Indian child with first seizure strongly suggests NCC.
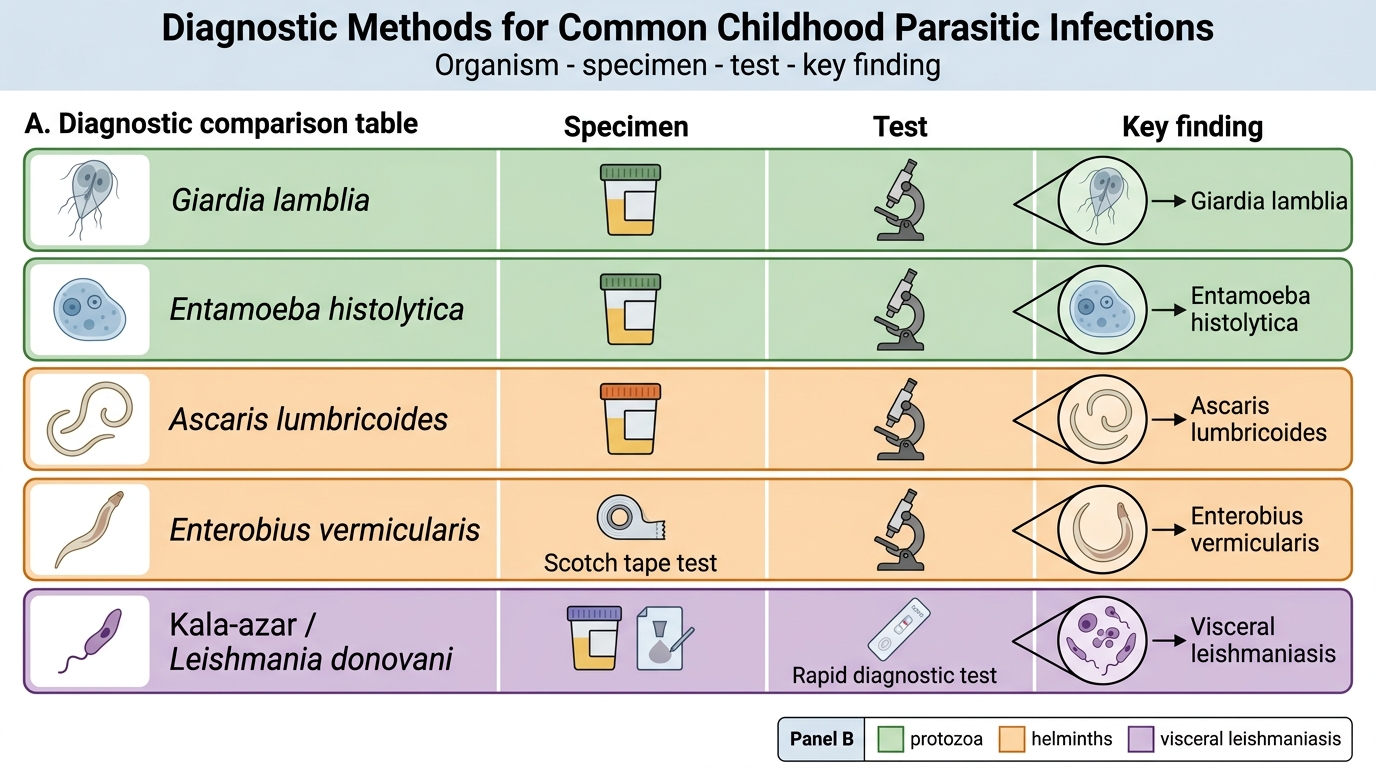
Diagnostic Methods for Childhood Parasitic Infections
Serological tests: Anti-amoebic antibodies (indirect haemagglutination, ELISA) are useful when stool microscopy is negative in suspected amoebic liver abscess (positive in >90% of cases). NCC serology (ELISA or Western blot) using T. solium cysticercus antigen is supportive but not required when CT findings are classic.
CLINICAL PEARL
The erythrophagocytic trophozoite test: In a fresh warm stool specimen from a child with bloody diarrhoea, the sight of actively moving amoebic trophozoites engulfing red blood cells under the microscope is pathognomonic for Entamoeba histolytica and mandates immediate treatment — both a tissue amoebiocide (metronidazole) AND a luminal agent (diloxanide furoate or paromomycin). Metronidazole alone reaches the intestinal wall but has poor activity against luminal cysts; skipping the luminal agent leaves a reservoir that causes relapse or ongoing cyst excretion to household contacts. This two-drug rule is one of the most-examined facts in paediatric infectious disease exams.