Page 26 of 32
PE31.14 | Parasitic Infections — SDL Guide (Part 2)
Management and Prevention
Treatment of parasitic infections follows a parasite-specific approach, and two overarching principles govern prescribing in children: first, that drugs must be selected based on the organism and its tissue compartment (luminal vs invasive trophozoite vs systemic vs CNS), because the same drug class does not reach all compartments with equal efficacy; second, that paediatric dosing is invariably weight-based and age-dependent, and adult fixed doses must never be extrapolated to children. Beyond individual case management, each major parasitic infection in India is addressed by a dedicated national programme — the National Deworming Day (NDD) for STH, the NVBDCP for kala-azar and filariasis — and the clinician must understand these programmes to counsel patients correctly about what has already been administered at the community level and what therapeutic doses are still required.
Soil-transmitted helminths (Ascaris, hookworm, Enterobius, Trichuris) — albendazole: The mainstay of treatment for all major STH is albendazole, a benzimidazole anthelmintic that inhibits tubulin polymerisation, disrupting microtubule-dependent glucose uptake in the worm.
- Children ≥2 years: 400 mg single oral dose (chewed or crushed with food).
- Children 1 to <2 years: 200 mg single oral dose (lower dose to match safety data; the WHO/NDD programme targets this age group).
- Children <1 year: albendazole is not routinely recommended; seek specialist guidance.
Albendazole is equally effective against Ascaris, hookworm, and Trichuris in a single dose, though a 3-day course (400 mg/day) improves cure rates against heavy Trichuris burdens. For pinworm (Enterobius), the dose is the same (400 mg single dose), with a repeat dose at 2 weeks to eliminate worms from autoinfected eggs deposited between the first and second doses. All household members should be treated simultaneously for Enterobius given high household transmission.
For iron-deficiency anaemia secondary to hookworm, concurrent oral iron supplementation (3–6 mg/kg/day of elemental iron) is mandatory — albendazole kills the worms but does not replenish iron stores.
National Deworming Day (NDD): India's NDD programme (launched 2015 by MoHFW) delivers biannual single-dose albendazole to all children aged 1–19 years in February and August through schools and Anganwadi centres, regardless of stool examination results. The programme is one of the largest preventive chemotherapy initiatives globally, reaching ~240 million children annually. A child found to have STH on clinical examination who has recently received the NDD dose should still receive a therapeutic dose if symptomatic (the programme dose treats but does not guarantee cure of heavy burdens). The correct age range 1–19 years (not 1–14 or 1–12) is frequently tested.
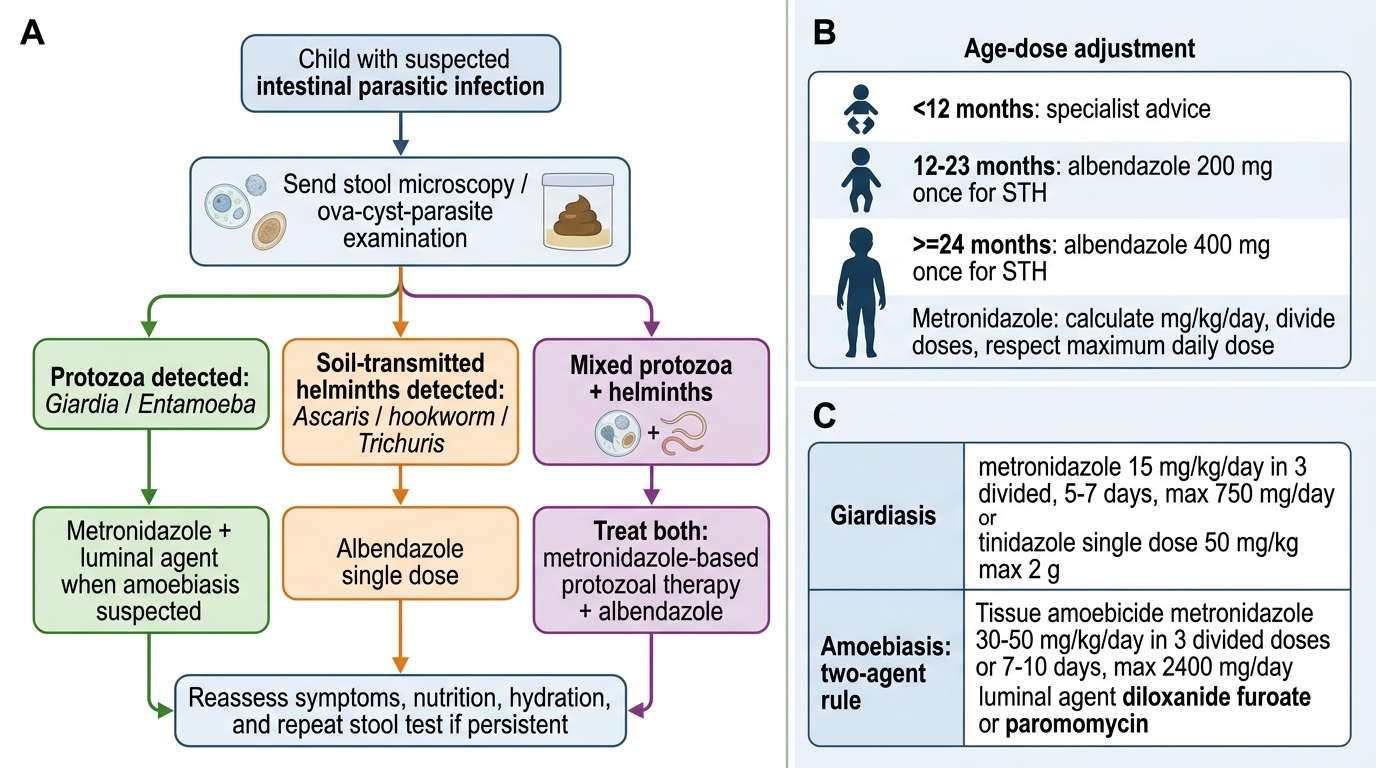
Algorithm for Suspected Intestinal Parasitic Infection in Children
Giardiasis: First-line treatment is metronidazole 15 mg/kg/day in 3 divided doses for 5–7 days (max 750 mg/day). Tinidazole (single dose 50 mg/kg, max 2 g) is an alternative with better compliance. Nitazoxanide is an effective alternative in metronidazole-resistant cases. Nutritional support is essential given the malabsorption component; formula-feeding infants should switch temporarily to lactose-free formula.
Amoebiasis — the two-agent rule: Treatment of invasive intestinal amoebiasis and amoebic liver abscess requires a tissue amoebiocide followed by a luminal agent:
1. Tissue amoebiocide: Metronidazole 30–50 mg/kg/day in 3 divided doses for 7–10 days (max 2400 mg/day). This kills tissue-invasive trophozoites in the gut wall and liver.
2. Luminal agent (to eliminate intraluminal cysts and prevent relapse): Diloxanide furoate 20 mg/kg/day in 3 divided doses for 10 days, OR Paromomycin 25–35 mg/kg/day in 3 divided doses for 7 days. Paromomycin is preferred in pregnancy and in young children if diloxanide is unavailable.
Amoebic liver abscess: the majority respond to metronidazole alone without aspiration. Aspiration is indicated if the abscess is large (>5 cm), threatens rupture, does not resolve in 72 h of therapy, or is in the left lobe (risk of pericardial extension).
Visceral leishmaniasis (kala-azar): The treatment of choice in India is liposomal amphotericin B (L-AmB) — a single infusion of 10 mg/kg or a short-course regimen (total 15–21 mg/kg over several infusions), available free under the NVBDCP elimination programme. Miltefosine (oral, weight-based: 2.5 mg/kg/day for 28 days; available for children ≥2 yr and >12 kg) is the WHO-recommended oral alternative. Sodium stibogluconate (antimonials) is no longer first-line in India due to resistance (>50% failure rates in Bihar). Post-kala-azar dermal leishmaniasis (PKDL) — a skin manifestation appearing months after treatment — requires prolonged miltefosine therapy.
Neurocysticercosis (NCC): Management is individualised based on CT stage and symptom burden:
- Anticonvulsants (phenobarbitone or carbamazepine/levetiracetam per current IAP epilepsy guidelines) are the primary treatment for seizure control.
- Cysticidal therapy (albendazole 15 mg/kg/day in 2 divided doses for 15–28 days, or praziquantel) accelerates radiological resolution and may reduce seizure recurrence in active (colloidal/vesicular) cysts. Cysticidal therapy should NOT be given in ocular or spinal NCC without specialist supervision; it is generally not given for calcified cysts.
- Corticosteroids (dexamethasone or prednisolone) are given concurrently with cysticidal therapy to reduce the perilesional inflammatory oedema triggered by dying cysts.
- Surgical VP shunt for obstructive hydrocephalus.
Lymphatic filariasis: Treatment with diethylcarbamazine (DEC) 6 mg/kg/day for 12 days kills microfilariae and has some macrofilaricidal activity; ivermectin 150 µg/kg single dose is an alternative. The NVBDCP's Mass Drug Administration (MDA) delivers annual DEC + albendazole (or DEC + albendazole + ivermectin in high-burden districts) to all residents ≥2 years, aiming for elimination by 2030.
Prevention and public health:
- WASH: Handwashing with soap, use of latrines, safe water supply — addresses all faeco-orally transmitted parasites.
- Footwear: reduces hookworm larval penetration.
- NDD (National Deworming Day): biannual albendazole for 1–19 yr.
- Food safety: thorough cooking of pork (to prevent Taenia/cysticercosis) and food washing.
- Vector control: insecticide-treated bed nets and sandfly control for kala-azar; Culex mosquito control for filariasis.
SELF-CHECK
An 8-year-old girl from Bihar presents with 6 weeks of fever, progressively enlarging abdomen, pallor, and a splenic tip at the umbilicus. rK39 rapid diagnostic test is positive. Which is the MOST appropriate first-line treatment in India today?
A. Sodium stibogluconate (SSG) 20 mg/kg/day intramuscularly for 30 days
B. Oral miltefosine 2.5 mg/kg/day for 28 days
C. Chloroquine 10 mg/kg/day for 3 days
D. Liposomal amphotericin B as per NVBDCP protocol
Reveal Answer
Answer: D. Liposomal amphotericin B as per NVBDCP protocol
Liposomal amphotericin B (L-AmB) is the first-line treatment for visceral leishmaniasis (kala-azar) in India under the NVBDCP elimination programme. Sodium stibogluconate (antimonials) is no longer recommended in India due to >50% resistance rates in Bihar. Miltefosine is the recommended oral alternative for children ≥2 yr and >12 kg, but L-AmB is the programme's preferred first-line in India. Chloroquine is an antimalarial with no activity against Leishmania. Note: Some protocols may accept miltefosine as an answer if L-AmB is unavailable — understand that L-AmB is the current national preference.
SELF-CHECK
A 5-year-old boy is treated for amoebic dysentery with metronidazole for 7 days and recovers from diarrhoea. His repeat stool examination 2 weeks later shows Entamoeba histolytica cysts. What went wrong with the initial management?
A. The dose of metronidazole was too low
B. Metronidazole should have been given for 14 days instead of 7 days
C. A luminal agent (diloxanide furoate or paromomycin) was not added after metronidazole
D. Tinidazole should have been used instead of metronidazole
Reveal Answer
Answer: C. A luminal agent (diloxanide furoate or paromomycin) was not added after metronidazole
Metronidazole is a tissue amoebiocide with poor luminal activity. It clears invasive trophozoites from the intestinal wall and liver but does not reliably eliminate cysts in the intestinal lumen. Persistent luminal cysts cause relapse (as in this case) and continue to infect household contacts. The correct protocol is metronidazole for 7–10 days FOLLOWED by a luminal agent — either diloxanide furoate 20 mg/kg/day for 10 days or paromomycin 25–35 mg/kg/day for 7 days. Extending metronidazole duration does not substitute for luminal agent activity.
Self-Assessment
Test your understanding with the following case-based questions and self-check prompts before attending your clinical posting.
Case 1: A 4-year-old girl from Uttar Pradesh complains of perianal itching, worse at night, for 3 weeks. Her mother reports that she scratches herself in her sleep and has been irritable. Physical examination is normal; stool examination shows no ova or cysts. What is the most appropriate next diagnostic step and the correct treatment including dose?
Self-check: The answer involves the cellophane-tape test (NOT stool examination, which is insensitive for Enterobius), a positive finding of flat-sided oval ova, and albendazole 400 mg single dose with a repeat at 2 weeks, plus treatment of all household members.
Case 2: A 9-year-old boy from a rural area presents with a first episode of generalised tonic-clonic seizure. He is neurologically intact between episodes. CT head with contrast shows a solitary 1.5 cm ring-enhancing lesion in the right parietal lobe with perilesional oedema. Family keeps pigs and the household toilet is an outdoor pit. What is the likely diagnosis, and what two pharmacological treatment categories are required?
Self-check: Neurocysticercosis (NCC). Treatment requires (1) antiepileptics for seizure control and (2) cysticidal therapy (albendazole 15 mg/kg/day for 15–28 days) with concurrent corticosteroids (dexamethasone) to manage the inflammatory response to dying cysts. The household exposure to pigs and poor sanitation supports Taenia solium transmission.
Viva-style prompts:
1. What is the National Deworming Day programme? State the age group targeted, the drug used, and the frequency.
2. A child has hookworm infection confirmed on stool examination and haemoglobin of 7.8 g/dL. Albendazole is prescribed. Is this sufficient? Justify.
3. Differentiate the clinical presentations of Giardia lamblia and Entamoeba histolytica diarrhoea on three parameters.
4. Why is a luminal agent always added after metronidazole in amoebic liver abscess treatment?
Answers for self-check:
1. NDD: launched 2015; targets 1–19 yr; albendazole 400 mg (≥2 yr)/200 mg (1–<2 yr) single dose; biannual (February + August).
2. No — albendazole alone kills the worms but does not replenish iron stores. Concurrent oral iron supplementation (3–6 mg/kg/day elemental iron) for 3 months is mandatory to correct the anaemia.
3. Giardia: no blood/mucus in stool, no fever, chronic malabsorption/greasy stools; Entamoeba: bloody mucoid stools, tenesmus, may have fever, may have liver abscess.
4. Metronidazole is a tissue amoebiocide with poor intraluminal activity; luminal cysts survive and cause relapse or ongoing household transmission. Luminal agents (diloxanide/paromomycin) eradicate the cyst reservoir.