Page 4 of 32
PE31.{2,5-8} | Tuberculosis Diagnosis Workflow — SDL Guide
Learning Objectives
- Elicit, document, and present a history of TB contact in every child encounter
- Identify a BCG scar and perform and interpret the Mantoux tuberculin skin test
- Select and describe the appropriate microbiological sample collection technique for a child unable to expectorate sputum
- Interpret blood tests — CBC, ESR, CRP, and ADA — in the context of suspected TB
- Explain the principle, indications, specimen requirements, and interpretation of CBNAAT/GeneXpert and BACTEC culture
- Apply the WHO/IAP diagnostic algorithm to categorise a child as confirmed, probable, or possible TB
INSTRUCTIONS
Diagnosing tuberculosis in children is among the most clinically challenging tasks in paediatric practice. Children are paucibacillary — they harbour too few organisms for smear microscopy — and they cannot expectorate sputum. The clinician must therefore combine a systematic contact history, skilled Mantoux testing, careful radiological interpretation, and appropriate sample collection to build a diagnostic case. This module takes you through each step as a practical skill, culminating in applying the integrated WHO/IAP algorithm. Mastery of this workflow is the clinical skill most directly responsible for reducing the unacceptable diagnostic delay that costs children their lives and neurological function.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 10 — Tuberculosis (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 254 — Tuberculosis (textbook)
- IAP Consensus Statement on Childhood Tuberculosis, 2020 (guideline)
- NTEP (National Tuberculosis Elimination Programme) — Paediatric TB Module, 2022 (guideline)
- WHO Operational Handbook on Tuberculosis, Module 5, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are in the paediatric OPD. A mother brings her 4-year-old daughter with 5 weeks of low-grade evening fever and poor weight gain. The father completed TB treatment 8 months ago. The child does not cough much, and when she does, she cannot produce sputum. Her BCG scar is present on the left arm. You want to confirm or exclude tuberculosis — but which tests do you order, and in what sequence? How do you collect a sputum sample from a child who cannot expectorate? What does a positive Mantoux really mean in this context? This module gives you the clinical decision framework to answer all three questions.
WHY THIS MATTERS
The gap between infection and confirmed diagnosis is where children with TB suffer avoidable damage. A child with tuberculous meningitis who receives treatment at Stage I survives neurologically intact; the same child treated at Stage III is left with hydrocephalus, deafness, or hemiplegia. The entire difference is speed of diagnosis. Yet childhood TB is systematically under-diagnosed because clinicians do not know how to collect samples from non-expectorating children, misinterpret Mantoux thresholds, or do not know when to apply CBNAAT. This module equips you with the complete diagnostic skill set mandated by NTEP and IAP — the competencies that shorten the diagnostic interval and save paediatric lives.
RECALL
Activate the following prior knowledge before proceeding:
• The primary complex (Ghon focus + hilar lymphadenopathy) is the defining paediatric TB lesion; children are paucibacillary — recall from pe24-tb-clinical.
• Cell-mediated immunity — CD4+ T-lymphocytes respond to M. tuberculosis antigens by releasing IFN-γ; this is the biological basis of both the TST and IGRA.
• AFB microscopy (Ziehl-Neelsen stain) requires ~10,000 bacilli/mL to be positive; children rarely reach this concentration — recall from Microbiology.
• Mantoux test uses PPD (Purified Protein Derivative), 5 tuberculin units (TU) in 0.1 mL, injected intradermally on the volar aspect of the forearm; the induration (not redness) is measured 48–72 hours later.
• BCG vaccine — given at birth (NIS), creates a scar on the left deltoid, and can cause a mild Mantoux reaction (usually ≤10 mm); does NOT cause IGRA to be positive.
Clinical Indication: When to Investigate for TB
The first clinical skill in TB diagnosis is recognising which children require a systematic TB workup. In an endemic country like India, the threshold for investigation must be low, because TB in children is paucibacillary and progresses silently until complications occur. The contact history is the single most important entry point: every child presenting with unexplained fever, weight loss, cough, lymphadenopathy, or neurological deterioration should be asked — as the very first step — about household contact with an adult TB case, particularly a smear-positive pulmonary TB case. This contact history must be documented meticulously in every new patient encounter and every follow-up note as a non-negotiable clinical habit, because a missed contact history is the most common reason childhood TB goes undetected until complications occur.
Indications for a TB diagnostic workup (IAP/NTEP criteria):
• Unexplained fever lasting ≥2 weeks not responding to antibiotics or antimalarials
• Unexplained weight loss or failure to thrive lasting ≥4 weeks
• Cough lasting ≥2 weeks (especially with hilar lymphadenopathy on CXR)
• Household or close contact with a smear-positive or culture-confirmed TB case
• Unexplained lymphadenopathy, ascites, or back pain/gibbus in an endemic setting
• Meningitis that is lymphocytic, subacute in onset, or unresponsive to antibiotics
• Any child with HIV and any new unexplained symptom
High-risk groups that require a lower threshold and more aggressive workup:
• Age <5 years (immature CMI, risk of miliary/TBM)
• Children with SAM (MUAC <11.5 cm, weight-for-height <−3 SD)
• HIV-infected children
• Children with previous TB or incomplete treatment
The BCG scar must be identified and documented as part of every TB contact assessment. It is typically located on the left deltoid, appears as a round or oval depressed scar 5–8 mm in diameter, and its presence confirms vaccination at birth. Its absence in a child from a high-risk family suggests either missed vaccination or an immune deficiency that prevented scar formation — both of which heighten TB risk. PE31.5 competency requires the clinician to elicit and document contact history, identify the BCG scar, and record both systematically.
Tuberculin Skin Test (Mantoux) and BCG Scar
The Mantoux tuberculin skin test (TST) is the standard immunological screening tool for TB infection in children. It detects prior sensitisation of T-lymphocytes to M. tuberculosis antigens via a delayed-type hypersensitivity (DTH) reaction. Understanding its technique, interpretation thresholds, and limitations is a core clinical skill.
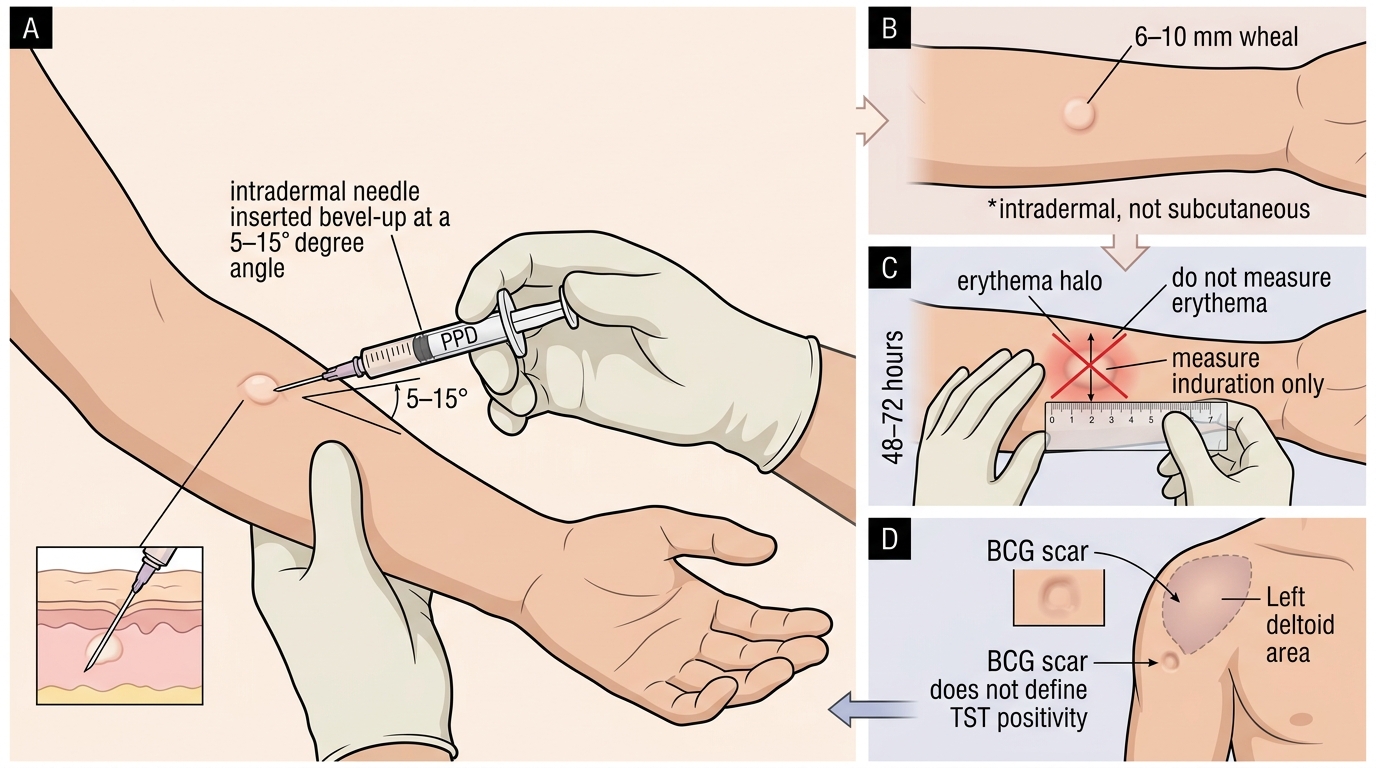
Technique (PE31.5): The Mantoux test must be performed carefully and read at the correct time interval — errors at either step are the most common cause of misinterpretation. The technique is standardised by the WHO and NTEP, and should be practised until it is reproducible. The key principle is intradermal injection — the needle tip must be partially visible through the skin, and the wheal must form immediately to confirm correct placement. Reading must be done at exactly 48–72 hours, because reactions that are read too early (before maximum induration) or too late (after induration starts to resolve) give inaccurate results.
- Inject 0.1 mL of PPD (5 TU) intradermally on the volar (anterior) aspect of the forearm using a 26-gauge needle, bevel upward, at a shallow angle (~15°)
- A raised pale wheal of 6–10 mm confirms correct intradermal placement; if no wheal forms (subcutaneous injection), repeat on the other arm
- Read at 48–72 hours — measure the transverse diameter of the induration (palpable hardness) with a ruler in millimetres; do NOT measure erythema (redness)
- Document the measurement, date, and lot number of PPD
Interpretation thresholds:
| Induration | Interpretation Context |
|---|---|
| ≥10 mm | Positive in immunocompetent children (regardless of BCG status in India) |
| ≥5 mm | Positive in: HIV-infected children, severe malnutrition (SAM), immunosuppressed (steroids >1 month), recent household contact with smear-positive TB |
| <5 mm | Negative (does NOT rule out TB — see limitations) |
In India, because BCG is given universally at birth and the TB prevalence is high, a reaction of ≥10 mm is considered positive in immunocompetent children even with a BCG scar. The BCG reaction typically causes ≤15 mm, but in a high-risk contact, ≥10 mm is treated as positive regardless.
False-negative TST (anergy): The TST can be negative despite active TB in: miliary TB, TBM (anergy due to immune exhaustion), severe malnutrition, HIV, measles, recent TB infection (<8 weeks — pre-sensitisation window), or very young age (<6 months — immature CMI). A negative TST does NOT exclude TB in a child with strong epidemiological and clinical evidence.
IGRA (Interferon-Gamma Release Assay): An in-vitro alternative (QuantiFERON-TB Gold, T-SPOT.TB) that measures IFN-γ released by sensitised T-cells in response to ESAT-6 and CFP-10 (antigens absent from BCG and most non-tuberculous mycobacteria). IGRA is NOT affected by BCG vaccination — it is more specific than TST in BCG-vaccinated populations. However, it is expensive and not routinely available in most Indian centres; it is used when TST interpretation is confounded by BCG.
Mantoux TST Technique and BCG Scar
SELF-CHECK
A 3-year-old child with HIV infection and a household TB contact has a Mantoux induration of 6 mm at 72 hours. How should this result be interpreted?
A. Negative — below the standard 10 mm threshold; no further action needed
B. Positive — the threshold is ≥5 mm in HIV-infected children; investigate further
C. Indeterminate — requires IGRA confirmation
D. BCG reaction — disregard as the child was vaccinated
Reveal Answer
Answer: B. Positive — the threshold is ≥5 mm in HIV-infected children; investigate further
In HIV-infected children (and those with severe malnutrition, immunosuppression, or close smear-positive contact), the Mantoux threshold for positivity is ≥5 mm, not ≥10 mm. A 6 mm induration in an HIV-positive child with household TB contact is therefore a positive test, and a full TB diagnostic workup — CXR, blood tests, and appropriate sample collection — should proceed. IGRA may not add much in resource-limited settings and does not replace the workup. BCG does not cause a positive IGRA, but here we are interpreting TST, not IGRA.
Microbiological Sampling Techniques
Microbiological confirmation of TB in children is challenging because children are paucibacillary and cannot expectorate sputum. Nevertheless, targeted sample collection is essential, especially when CBNAAT or culture confirmation is needed for drug-resistance assessment or definitive diagnosis. Understanding the correct sample for each clinical form of childhood TB — and the rationale for choosing it — is a key knowledge skill (PE31.7) that directly determines whether the laboratory receives a viable, high-yield specimen or an uninterpretable one.
Gastric aspirate (gold-standard microbiological sample in children <10 years):
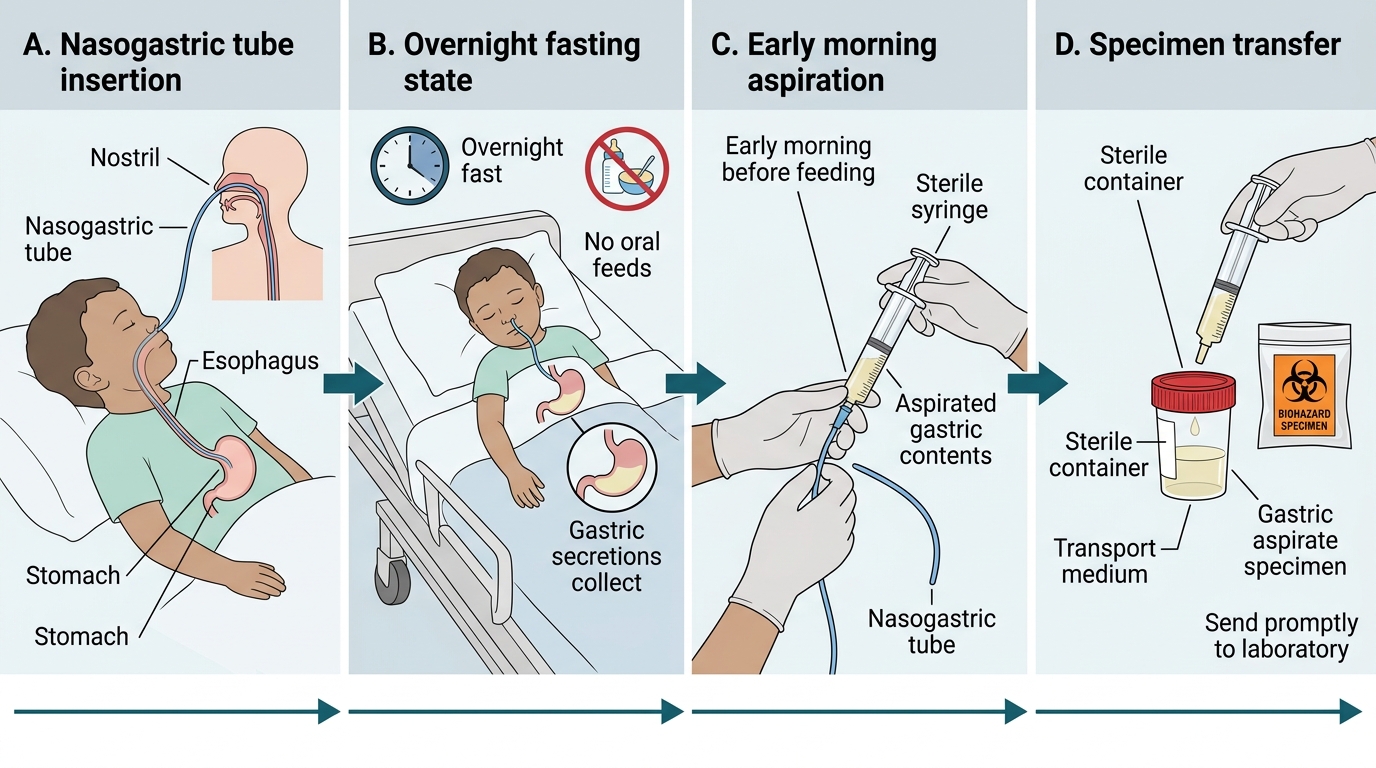
When a child cannot expectorate, swallowed respiratory secretions pool in the stomach during sleep. Early morning gastric aspiration (before the child rises or eats) retrieves these pooled secretions, which contain the highest bacterial load. The procedure:
1. Child fasts overnight (no feeds after midnight for infants, ≥4 h for older children)
2. Insert a nasogastric tube (NGT) in the morning before the child gets up
3. Aspirate stomach contents (5–10 mL); if inadequate, instil 5–10 mL sterile distilled water and re-aspirate
4. Transfer immediately to a neutralising transport medium (sodium carbonate) because gastric acid is bactericidal to M. tuberculosis
5. Repeat on 3 consecutive mornings to maximise yield (bacteriological yield ~30–40% in culture-confirmed cases)
Induced sputum: Used in children ≥5 years who cannot spontaneously expectorate. Following nebulisation with 3% hypertonic saline (bronchodilator pre-treatment with salbutamol), the child coughs up sputum, which is collected. Sensitivity is comparable to gastric aspirate and less invasive in older children.
Bronchoalveolar lavage (BAL): Performed under general anaesthesia via bronchoscope; the highest bacteriological yield (~50% culture positivity) but reserved for cases where gastric aspirate/induced sputum are negative and diagnosis is critical. Particularly useful in miliary TB and HIV-infected children.
Fine-needle aspiration cytology (FNAC): For peripheral TB lymphadenitis — insert a 22-gauge needle into the node and aspirate; material sent for cytology (caseous necrosis, epithelioid granulomas, Langhans cells) and AFB staining/culture. Yield ~60–70% in lymph-node TB.
CSF: For presumed TBM — performed after fundoscopy and neuroimaging; send for cell count, protein, glucose, AFB smear, CBNAAT, and culture. Volume ≥3–5 mL improves CBNAAT sensitivity.
Other samples by site: pleural fluid (thoracocentesis — ADA, AFB smear, CBNAAT, culture), peritoneal fluid (ascites tap), bone biopsy (Pott's), urine (renal TB — early morning mid-stream urine ×3).
Stepwise Gastric Aspirate Collection in a Child