Page 5 of 32
PE31.{2,5-8} | Tuberculosis Diagnosis Workflow — SDL Guide (Part 2)
Rapid Molecular Diagnostics: CBNAAT/GeneXpert
CBNAAT (Cartridge-Based Nucleic Acid Amplification Test), commercially known as GeneXpert MTB/RIF, is the WHO-recommended rapid molecular diagnostic test for tuberculosis and is now the first-line rapid test within the NTEP in India. It represents a major advance in paediatric TB diagnosis because it detects M. tuberculosis DNA (not live organisms) and simultaneously identifies rifampicin resistance (by detecting mutations in the rpoB gene), achieving results in under 2 hours.
How CBNAAT works: A liquefied and decontaminated specimen is loaded into a sealed disposable cartridge. The cartridge automatically performs DNA extraction and real-time PCR amplification of a specific M. tuberculosis genomic sequence. The instrument reports: (1) MTB detected/not detected and, if detected, (2) rifampicin resistance detected/indeterminate/not detected. The entire process is cartridge-sealed, minimising contamination risk and enabling use in district-level laboratories.
Specimen types for CBNAAT (PE31.8 — indications):
• Respiratory: gastric aspirate (preferred in children), induced sputum, BAL
• Non-respiratory: CSF (TBM), lymph-node aspirate (TBLN), pleural fluid, pus from cold abscess
• Any extra-pulmonary specimen from a site clinically suspicious for TB
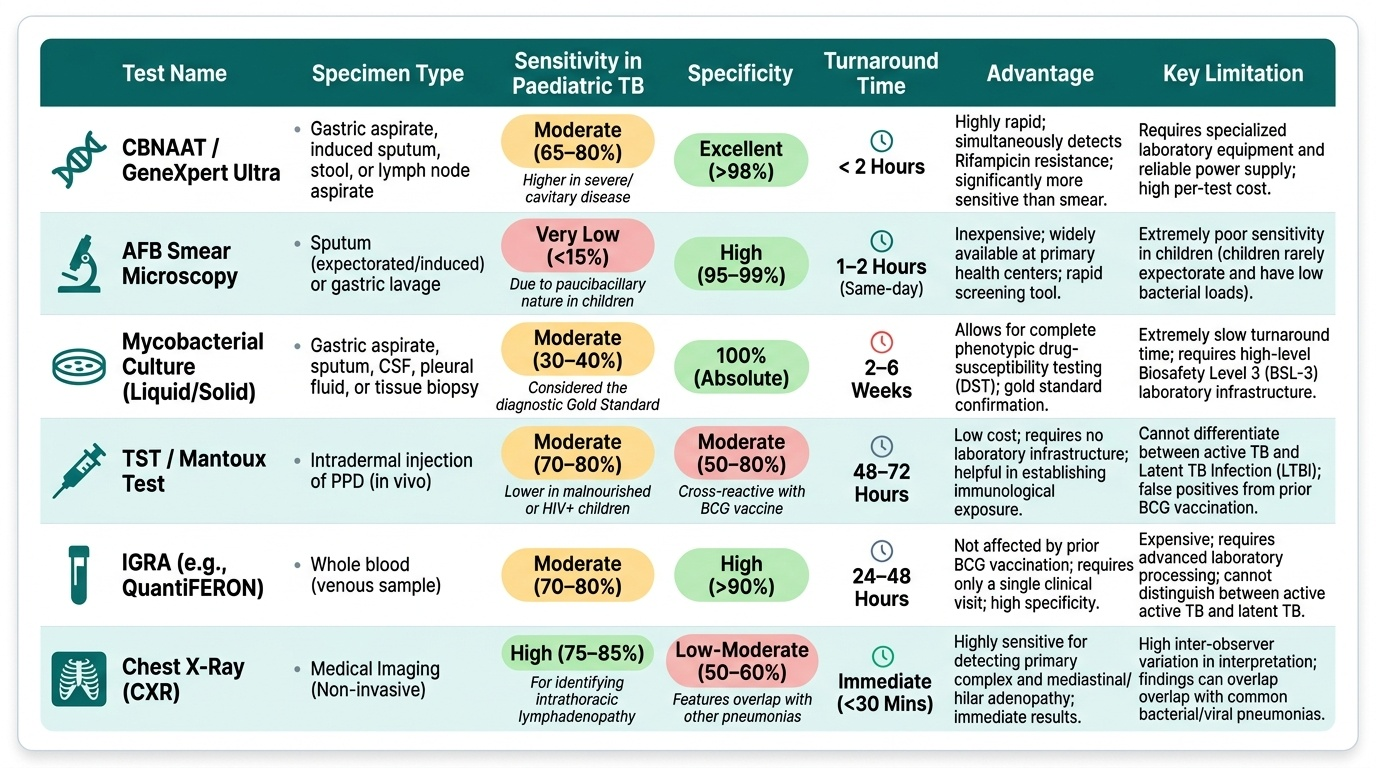
Sensitivity limitations in children: CBNAAT sensitivity in children is ~70–80% in pulmonary TB when gastric aspirate is used (vs ~95% in smear-positive adults). Sensitivity is lower in paucibacillary samples — a negative CBNAAT does NOT exclude TB in a child with strong clinical and radiological evidence.
Rifampicin resistance detected on CBNAAT should prompt immediate referral for Drug-Resistant TB (DR-TB) workup including Line Probe Assay (LPA) and second-line drug susceptibility testing (DST). Rifampicin resistance is a strong proxy for MDR-TB.
BACTEC MGIT (Mycobacterium Growth Indicator Tube) liquid culture: The gold standard for M. tuberculosis confirmation and full drug susceptibility testing. Growth detected by fluorescence change (oxygen consumption) in 1–3 weeks vs 4–8 weeks for solid Löwenstein-Jensen (LJ) medium. Used when CBNAAT is negative but TB is strongly suspected, or when DST is needed. Requires biosafety level 2 laboratory and 2–6 weeks for results — not suitable for acute management decisions.
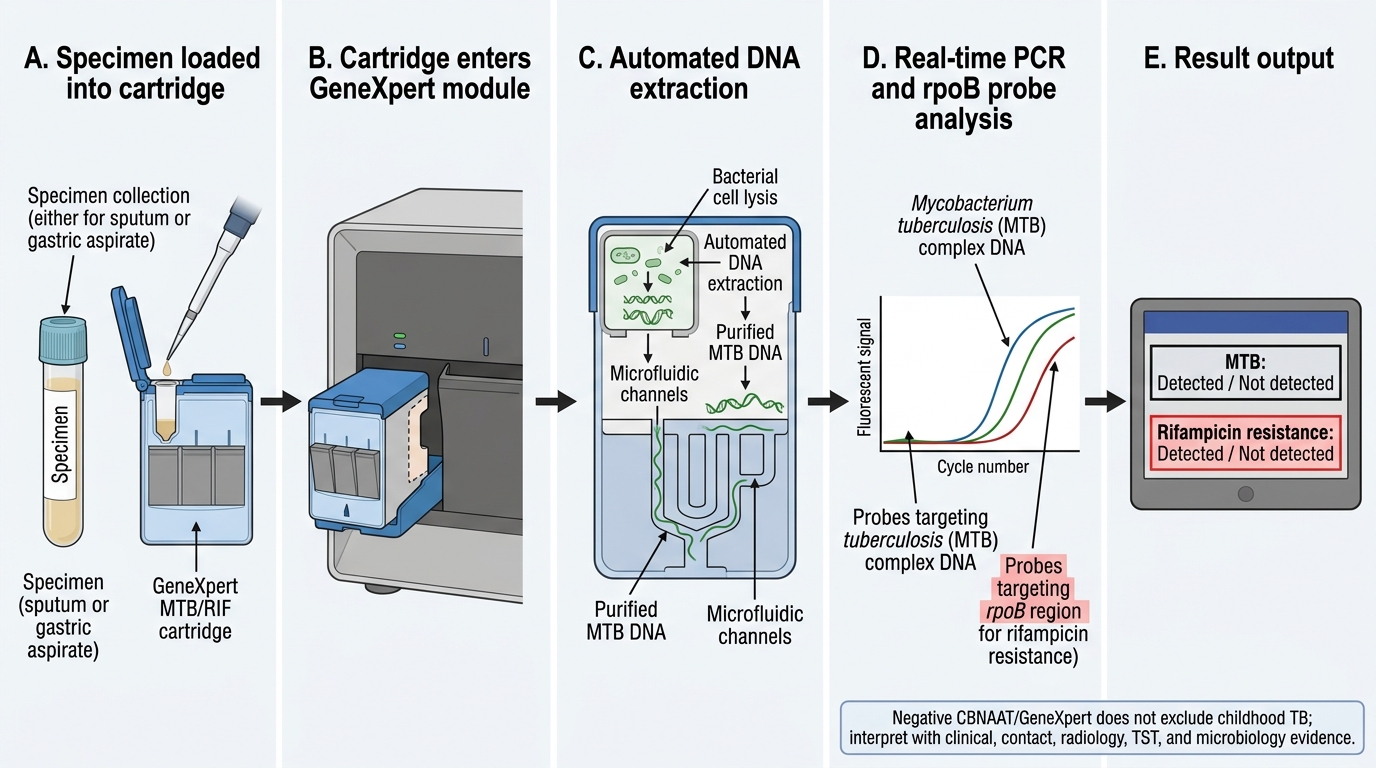
GeneXpert MTB/RIF Workflow
CLINICAL PEARL
The paucibacillary trap: In children, no single test rules in OR rules out TB. A negative Mantoux in a malnourished child does not exclude TB (anergy). A negative CBNAAT on gastric aspirate does not exclude TB (sensitivity ~70%). A normal CXR does not exclude extrapulmonary TB. The IAP/WHO diagnostic approach therefore uses a SCORING SYSTEM combining epidemiological (contact history), clinical (symptoms, malnutrition), immunological (TST), radiological (CXR), and microbiological (sample results) evidence — a child can be diagnosed as 'probable TB' without microbiological confirmation if the composite score is high enough. Never dismiss TB because one test is negative; the weight of combined evidence determines the diagnosis.
Interpreting Blood Tests and Radiology
Blood tests in childhood TB are non-specific but contribute supportive evidence when interpreted alongside clinical and microbiological findings. No single blood test is diagnostic; their value is in building the composite case and monitoring for complications (PE31.6). The clinician must interpret each result in its clinical context — an elevated ESR in a malnourished child with a TB contact and hilar lymphadenopathy on CXR carries very different diagnostic weight from the same ESR value in an otherwise healthy child with a viral upper respiratory tract infection. This contextualised interpretation is what distinguishes a competent clinician from one who orders tests without a framework for reading them. Blood tests also serve a monitoring role: baseline liver function is recorded before starting rifampicin-containing regimens because drug-induced hepatitis is an important adverse effect that requires early detection.
Blood test findings in childhood TB:
| Test | Typical Finding in TB | Clinical Significance | Limitation |
|---|---|---|---|
| CBC | Mild anaemia (normocytic), lymphocytosis | Non-specific; anaemia worsens with malnutrition | Also in viral, other infections |
| ESR | Elevated (>20–40 mm/1h in children) | Supports active infection/inflammation | Highly non-specific |
| CRP | Elevated | Active inflammation | Non-specific |
| ADA (CSF) | >10 U/L in TBM | Supports TB when culture pending | False positive in malignancies |
| ADA (pleural fluid) | >40 U/L | High sensitivity/specificity for TB pleuritis | Not 100% specific |
| LFT | May be abnormal with hepatic TB or rifampicin | Baseline before treatment | Drug-induced hepatitis monitoring |
Radiological interpretation (CXR): The chest X-ray is the single most important investigation in suspected pulmonary TB in children. Key findings to recognise:
• Hilar/mediastinal lymphadenopathy — widened mediastinum or lobulated hilar shadow; the hallmark of primary TB in children
• Primary complex — hilar lymphadenopathy + ipsilateral parenchymal opacity (Ghon focus)
• Segmental collapse/consolidation — due to bronchial compression by lymph nodes; persistent for >2 weeks, not responding to antibiotics
• Miliary pattern — bilateral, uniformly distributed 1–2 mm nodules; bilateral and symmetrical
• Pleural effusion — unilateral, with moderate-to-large effusion; lymphocyte-dominant exudate
• Cavitation — uncommon in children <10 years; more typical in adolescents with adult-type TB
A normal CXR does NOT exclude TB, especially extrapulmonary forms (TBM, TBLN, abdominal, osteoarticular).
SELF-CHECK
A 5-year-old child with presumed tuberculous meningitis has a gastric aspirate sent for CBNAAT. The result comes back: 'MTB not detected.' What is the MOST appropriate next step?
A. Exclude TB meningitis — CBNAAT is the gold-standard test
B. Send CSF for CBNAAT, culture, cell count, protein, and glucose — clinical suspicion drives management
C. Repeat gastric aspirate next morning and defer lumbar puncture
D. Start antifungal treatment — negative TB test makes cryptococcal meningitis more likely
Reveal Answer
Answer: B. Send CSF for CBNAAT, culture, cell count, protein, and glucose — clinical suspicion drives management
CBNAAT sensitivity from gastric aspirate in paediatric TB is ~70–80%, meaning a negative result does NOT exclude TB. In suspected TBM, the appropriate sample for CBNAAT is CSF — not gastric aspirate. The CSF should be sent for CBNAAT, AFB smear, culture, cell count (lymphocytic pleocytosis), protein (elevated), and glucose (low relative to blood). Clinical suspicion of TBM — insidious fever, headache, neck rigidity, CSF lymphocytosis — is sufficient to start anti-TB therapy while awaiting results. Never wait for a positive microbiological result before treating suspected TBM.
Applied Diagnostic Practice: Integrating Findings
The final and most demanding skill in TB diagnosis is integrating multiple imperfect data sources into a coherent clinical decision. In adult TB, a positive sputum smear or CBNAAT often settles the diagnosis; in childhood TB, no single test is both sensitive and specific enough to do so. The WHO and IAP therefore recommend a composite scoring or algorithmic approach that combines five domains of evidence — epidemiological (contact history), clinical (symptoms, duration, weight loss), immunological (TST/IGRA), radiological (CXR pattern), and microbiological (sample results) — and uses the weight of that combined evidence to categorise the child into one of three diagnostic groups, each with clearly defined and different management implications that determine whether treatment is started, deferred, or escalated to a drug-resistance workup.
Provided image
Three diagnostic categories (NTEP/IAP framework):
• Confirmed TB: Microbiological confirmation by culture, CBNAAT, or AFB smear from an appropriate specimen — regardless of clinical picture
• Probable (clinically diagnosed) TB: Clinical + epidemiological + radiological/immunological evidence consistent with TB, but no microbiological confirmation; requires two of: (1) TST ≥10 mm or IGRA positive, (2) CXR consistent with TB, (3) compatible clinical features + contact history — treated as TB
• Possible TB: Clinical suspicion but inadequate evidence in either category above; re-evaluate after a trial of antibiotics to exclude bacterial pneumonia
The WHO symptom-based screening tool for children: Any child with: (1) contact with a TB case, (2) weight loss or failure to gain weight, (3) cough ≥2 weeks, or (4) fever ≥2 weeks should be investigated further for TB. This 4-item screen has high sensitivity (>96%) for TB in children in high-burden countries.
Practical diagnostic algorithm:
1. Elicit contact history + document BCG scar → if contact present, proceed to step 2
2. CXR → if hilar adenopathy/primary complex present, strongly supports TB
3. Mantoux TST → interpret with correct threshold (≥10 mm standard; ≥5 mm if immunocompromised/SAM)
4. Send appropriate sample for CBNAAT (gastric aspirate × 3, or site-specific sample)
5. Blood tests (CBC, ESR, CRP, ADA if pleural/CSF) — supportive evidence
6. Categorise → confirmed, probable, possible → treat or refer accordingly
7. Check for HIV — all children with TB should have HIV testing
When to refer for Drug-Resistant TB workup:
Any child with: CBNAAT showing rifampicin resistance; failure to respond to standard first-line therapy at 2 months; history of prior TB treatment; contact with a known MDR-TB case → refer to DR-TB centre for LPA and DST.
SELF-CHECK
In the NTEP/IAP diagnostic framework, a 4-year-old with a household TB contact, positive Mantoux (14 mm), CXR showing right hilar lymphadenopathy, and negative CBNAAT on gastric aspirate should be classified as:
A. Confirmed TB — start treatment immediately
B. Probable (clinically diagnosed) TB — treat as TB based on clinical-epidemiological evidence
C. Possible TB — observe and repeat investigation in 4 weeks
D. Not TB — CBNAAT negative excludes the diagnosis
Reveal Answer
Answer: B. Probable (clinically diagnosed) TB — treat as TB based on clinical-epidemiological evidence
This child meets criteria for probable (clinically diagnosed) TB: household contact with TB + positive Mantoux (≥10 mm) + CXR consistent with primary complex. The negative CBNAAT does not exclude TB — sensitivity in paediatric gastric aspirate is ~70–80%. Under the NTEP/IAP framework, a child with strong epidemiological evidence + positive TST + consistent CXR is treated as TB ('probable TB category') without waiting for microbiological confirmation. Starting treatment promptly is the correct and potentially life-saving decision.
Self-Assessment
The following scenario-based and skills-recall questions consolidate the TB diagnostic workflow. These questions are designed at the NMC competency level for PE31.2, PE31.5, PE31.6, PE31.7, and PE31.8 — they test both factual knowledge of thresholds and procedures, and the integration skill required to synthesise clinical, immunological, radiological, and microbiological findings into a diagnostic category. Work through each question before looking at the answer, and use the structured framework: identify the indication, choose the appropriate test, apply the correct interpretation threshold, and classify the diagnostic category. Remember that in childhood TB, the weight of composite evidence — not a single test — determines the diagnosis, and a negative result is never sufficient grounds alone to exclude TB in a high-risk child.
- You are teaching a medical student how to perform a Mantoux test. List the steps of the procedure in order and explain why induration — not erythema — is measured.
- A 2-year-old child with HIV and a TB contact has severe malnutrition (MUAC 10.5 cm). Her Mantoux is 4 mm at 72 hours. Her CXR shows bilateral miliary nodules. Classify her TST result and state your next diagnostic step.
- Explain why gastric aspirate is used instead of sputum in children under 10 years for TB bacteriology. Describe the technique step by step.
- A CBNAAT result on a lymph-node aspirate from a child with matted cervical lymph nodes shows: 'MTB detected, rifampicin resistance indeterminate.' What are the implications of this result, and what is your next step?
- Construct a diagnostic summary for a 6-year-old with a 4-week history of fever, hilar lymphadenopathy on CXR, positive Mantoux (11 mm), and negative gastric aspirate CBNAAT. Classify as confirmed/probable/possible TB and justify your classification.