Page 7 of 17
PE4.1 | Attention Deficit Hyperactivity Disorder — SDL Guide
Learning Objectives
- Describe the clinical features of ADHD across the three DSM-5 presentations (inattentive, hyperactive-impulsive, combined)
- Explain the neurobiological and genetic aetiology of ADHD and relevant environmental risk factors
- Apply the DSM-5 diagnostic criteria for ADHD and distinguish it from common differential diagnoses
- Outline the multimodal management of ADHD including psychoeducation, behavioural therapy, pharmacotherapy, and school accommodations
INSTRUCTIONS
Attention Deficit Hyperactivity Disorder (ADHD) is the most common neurodevelopmental disorder of childhood, affecting approximately 5–7% of school-age children globally and an estimated 5–11% in India. It is also one of the most misunderstood: many children with ADHD are labelled as 'naughty,' 'lazy,' or 'not trying hard enough,' and may go years without diagnosis while falling behind academically and socially. As a clinician, you will encounter ADHD in every outpatient setting — from a school health camp to a paediatric OPD. Understanding its clinical features, diagnostic criteria, and evidence-based management will allow you to make a life-changing difference for these children and their families.
References
- Ghai Essential Pediatrics, 9th ed., Ch 18 (Neurodevelopmental Disorders — ADHD) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 49 (Attention-Deficit/Hyperactivity Disorder) (textbook)
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5), 2013 — ADHD criteria (classification)
- IAP Guidelines on Attention Deficit Hyperactivity Disorder, 2019 (guideline)
- American Academy of Pediatrics (AAP) Clinical Practice Guideline for ADHD, 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rohan is an 8-year-old boy brought to your outpatient clinic by his frustrated mother. His teacher has sent three notes home this term: 'Rohan does not listen, cannot stay in his seat, and disrupts the class constantly.' At home, his mother says he forgets his homework, loses things every day, and cannot finish any task — 'It's like his mind is always somewhere else.' His parents are bewildered because Rohan can sit for hours playing video games without a break. 'He's just being difficult,' his father says. Is Rohan 'naughty' — or is something else going on?
WHY THIS MATTERS
ADHD is the most common neurodevelopmental disorder of childhood worldwide. In India, studies report prevalence rates of 5–11% in school-age children, meaning in a typical class of 40, two to four children may have ADHD. The disorder is not outgrown in most cases — approximately 60–80% of children with ADHD continue to have clinically significant symptoms into adolescence, and 30–50% into adulthood. The consequences of missed or delayed diagnosis are substantial: academic underperformance, school dropout, low self-esteem, substance misuse in adolescence, and occupational difficulties in adulthood. Yet ADHD responds well to treatment — both behavioural and pharmacological — making early recognition and management one of the highest-impact interventions you can offer a struggling child.
RECALL
Before studying ADHD, recall the relevant background knowledge:
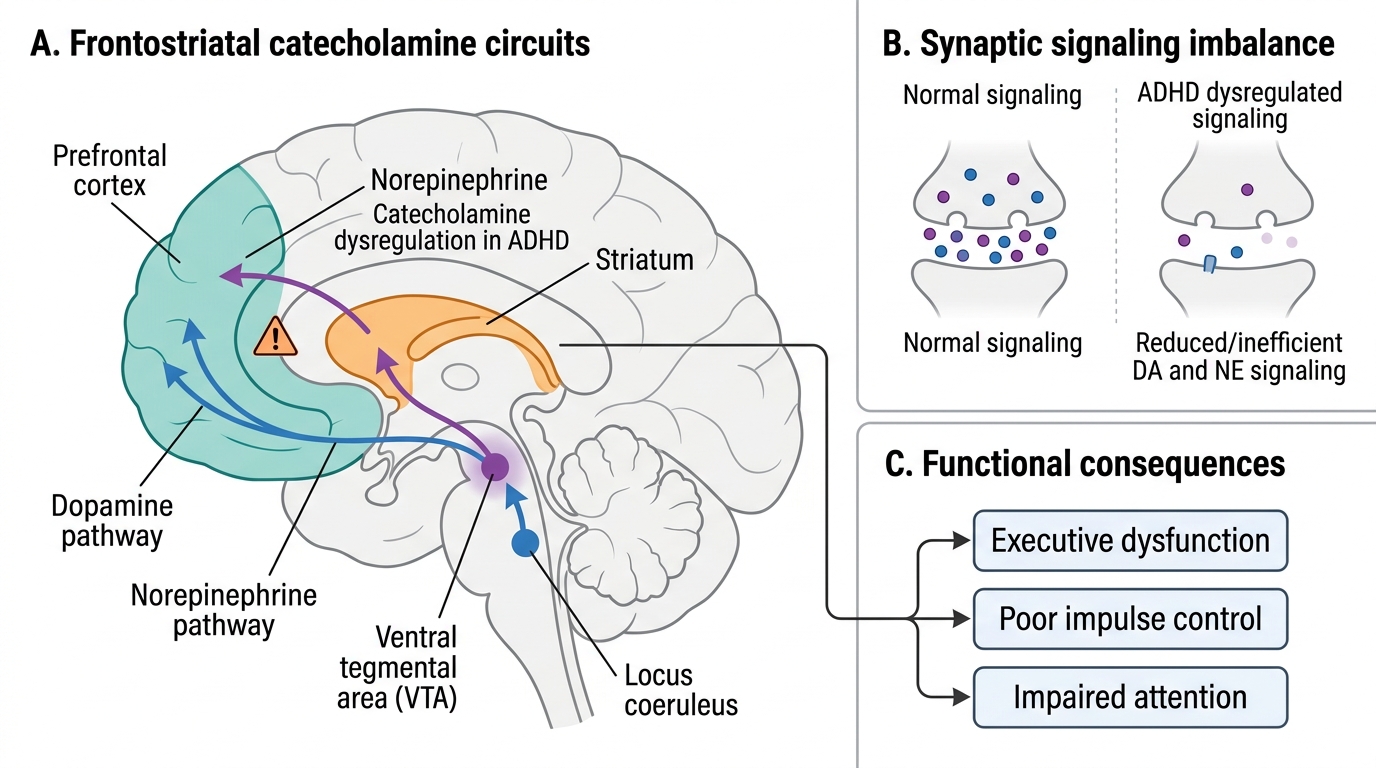
• Prefrontal cortex (PFC): the brain region responsible for executive functions — working memory, impulse control, sustained attention, planning, and inhibition of inappropriate responses. The PFC matures slowly, reaching full development in early adulthood.
• Dopamine and norepinephrine: the two key neurotransmitters in the PFC and striatum that regulate attention and impulse control. Drugs that increase these (stimulants) are the cornerstone of ADHD pharmacotherapy.
• Normal childhood behaviour: all young children are active, distractible, and impulsive to some degree. The distinction is one of degree, pervasiveness (home AND school), persistence (≥6 months), and functional impairment — not occasional inattention or restlessness.
• Developmental milestones: by age 5, children are expected to follow multi-step instructions, maintain attention for ~10–15 minutes in structured play, and inhibit impulsive actions in social situations.
Clinical Presentation of ADHD
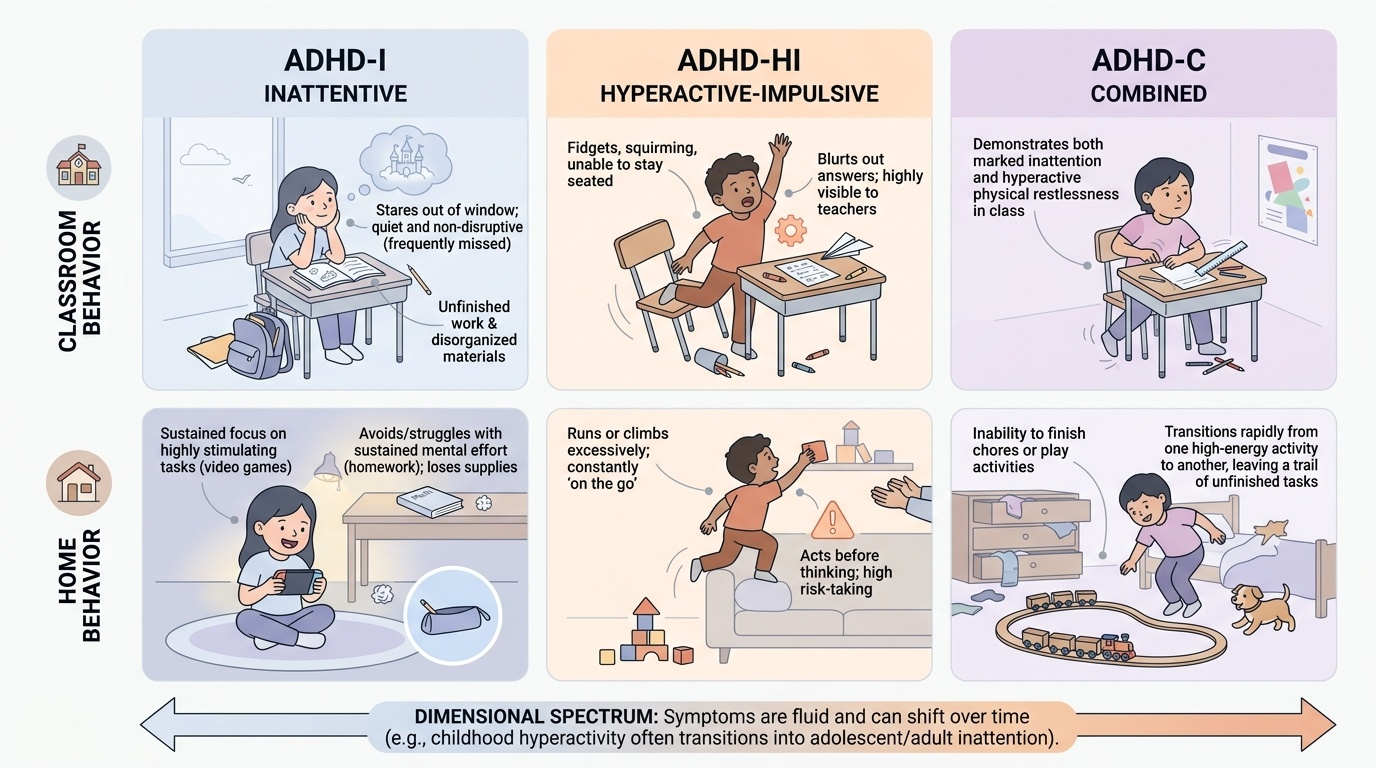
Attention Deficit Hyperactivity Disorder (ADHD) is characterised by a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with development and functioning. The DSM-5 recognises three clinical presentations based on the predominant symptom domain, and understanding these presentations is essential for clinical recognition because the same disorder looks very different across children — one child may be the classroom disrupter who cannot sit still, while another is the quiet girl who stares out of the window and never finishes her work. Both have ADHD; only one will be referred. The clinical presentations must be understood not as rigid categories but as the predominant end of a dimensional spectrum, and a given child's presentation may shift over time — for instance, hyperactivity often decreases in adolescence while inattention persists, so a child who was combined in childhood may appear inattentive-only as a teenager.
Provided image
Predominantly Inattentive Presentation (ADHD-I): The child appears 'dreamy,' forgetful, and easily distracted but is NOT typically disruptive. This presentation is the most frequently missed, particularly in girls, because the child does not cause classroom disturbance. Core features include:
• Fails to give close attention to details; makes careless errors in schoolwork
• Difficulty sustaining attention in tasks or play (but CAN focus on highly stimulating activities such as video games)
• Appears not to listen when spoken to directly ('in their own world')
• Does not follow through on instructions; fails to finish tasks
• Difficulty organising tasks and activities
• Avoids or dislikes tasks requiring sustained mental effort (homework, reading)
• Loses things necessary for tasks (pencils, books, school supplies)
• Easily distracted by extraneous stimuli
• Forgetful in daily activities
Predominantly Hyperactive-Impulsive Presentation (ADHD-HI): The child is 'always on the go,' cannot stay seated, and acts before thinking. This presentation is more visible and more often referred for assessment. Core features include:
• Fidgets with hands/feet; squirms in seat
• Leaves seat in classroom when expected to remain seated
• Runs or climbs excessively in situations where it is inappropriate
• Unable to play quietly
• Acts as if 'driven by a motor'
• Talks excessively
• Blurts out answers before questions are complete
• Difficulty waiting for their turn
• Interrupts or intrudes on others
Combined Presentation (ADHD-C): Both inattention and hyperactivity-impulsivity criteria are met. This is the most common presentation seen in clinic.
A key clinical point: ADHD symptoms must occur in more than one setting. A child who is inattentive only at school (perhaps due to an uninteresting curriculum or a hearing problem) but functions normally at home does NOT meet ADHD criteria. The pervasiveness of symptoms is a diagnostic requirement.
Pathophysiology and Aetiology of ADHD
ADHD is a neurobiological disorder with a strong genetic basis, arising from dysfunction in dopaminergic and noradrenergic circuitry in the prefrontal cortex and its connections to the striatum, cerebellum, and limbic system. Understanding the biological underpinning is important because it legitimises the disorder for sceptical families, justifies pharmacotherapy, and guides the clinician toward identifying modifiable risk factors.
Neurobiological basis:
Neuroimaging studies consistently show that children with ADHD have reduced volume and delayed maturation of the prefrontal cortex (PFC) — particularly the right dorsolateral PFC and the caudate nucleus. The PFC is the seat of executive functions: working memory, response inhibition, sustained attention, and the ability to defer reward. Deficient dopaminergic and noradrenergic transmission in the PFC-striatal circuit impairs these executive functions, producing the clinical syndrome of inattention, hyperactivity, and impulsivity. Stimulant medications (methylphenidate) work precisely by increasing synaptic dopamine and norepinephrine in these circuits, restoring more normal PFC function.
Genetic aetiology:
Heritability of ADHD is approximately 76–80% — one of the highest heritability estimates for any psychiatric condition. First-degree relatives of children with ADHD have a 5-fold increased risk. Candidate genes include those encoding dopamine receptors (DRD4, DRD5), dopamine transporter (DAT1/SLC6A3), and norepinephrine transporter (NET1/SLC6A2). No single gene causes ADHD; it is a polygenic disorder.
Environmental risk factors (non-genetic contributors):
- Prenatal exposures: Maternal smoking during pregnancy doubles the risk of ADHD in offspring. Prenatal alcohol exposure, particularly fetal alcohol spectrum disorder, causes ADHD-like symptoms. Prenatal lead exposure is a well-established risk factor; blood lead level even in the 5–10 µg/dL range correlates with attention and impulse control deficits.
- Prematurity and low birth weight: Premature infants have higher rates of ADHD, likely due to periventricular white matter injury affecting frontostriatal circuits.
- Perinatal adversity: Birth asphyxia and severe neonatal hypoglycaemia are associated with ADHD.
- Psychosocial factors: Severe early deprivation, institutional care, and high family adversity can produce ADHD-like behaviours, though whether these cause biological ADHD or a phenocopy is debated.
IMPORTANT: ADHD is NOT caused by sugar intake, watching television, bad parenting, or lack of discipline — these are common misconceptions that should be proactively addressed when counselling families.
Neurobiological Basis of ADHD
SELF-CHECK
The DSM-5 age of onset criterion for ADHD states that several symptoms must be present before which age?
A. Age 5 years
B. Age 7 years
C. Age 12 years
D. Age 16 years
Reveal Answer
Answer: C. Age 12 years
DSM-5 requires that several inattentive or hyperactive-impulsive symptoms were present before age 12 years. This was a change from DSM-IV, which required onset before age 7. The change acknowledges that the predominantly inattentive presentation often goes unrecognised until late childhood or early adolescence, particularly in girls. Onset must be established retrospectively if the child presents after age 12.
Diagnosis of ADHD
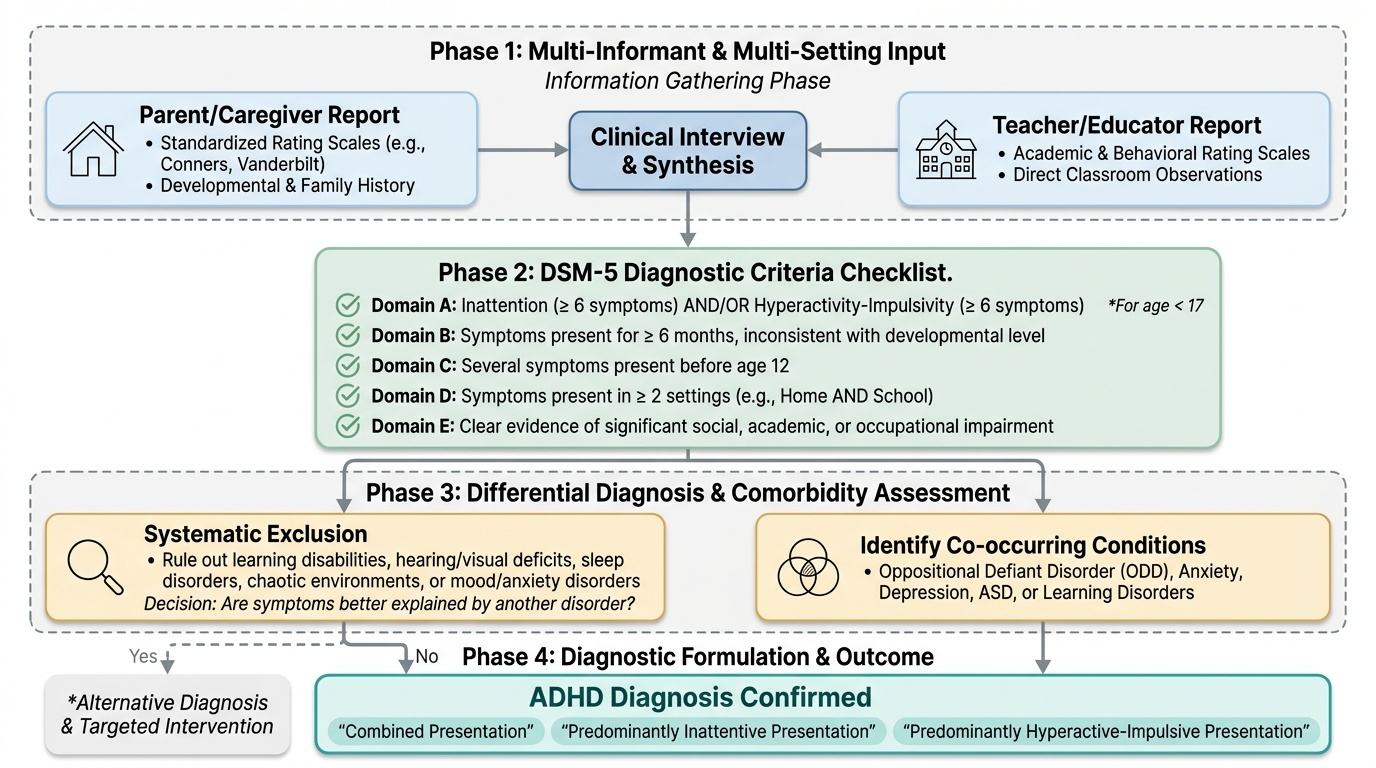
ADHD is a clinical diagnosis — there is no blood test, brain scan, or single instrument that confirms it. The diagnosis rests on careful history-taking, direct behavioural observation, standardised rating scales completed by multiple informants, and the systematic exclusion of alternative diagnoses. Clinicians who rely on a single informant (e.g. only the teacher's report) or fail to assess functioning across settings will both over- and under-diagnose. The diagnostic process demands information from at least two settings because the DSM-5 pervasiveness criterion is fundamental — a child who is inattentive only in school may have a learning disability, hearing problem, or a poorly structured classroom rather than ADHD. Conversely, a child who only appears hyperactive at home may be responding to a chaotic home environment rather than expressing a neurodevelopmental disorder. Gathering data from both parents and teachers using validated rating scales, and then applying the full DSM-5 criteria systematically, is the minimum standard for responsible ADHD diagnosis.
Provided image
DSM-5 Diagnostic Criteria (summarised):
1. Domain A — Symptom threshold: ≥6 inattention symptoms AND/OR ≥6 hyperactivity-impulsivity symptoms (each symptom must occur often), for children under 17 years; ≥5 for age ≥17.
2. Domain B — Duration: Symptoms present for ≥6 months, to a degree inconsistent with developmental level.
3. Domain C — Onset: Several symptoms present before age 12.
4. Domain D — Pervasiveness: Symptoms present in ≥2 settings (e.g., home AND school).
5. Domain E — Impairment: Clear evidence of significant impairment in social, academic, or occupational functioning.
6. Domain F — Exclusion: Symptoms not better explained by another mental disorder (psychosis, anxiety, depression, ASD, intellectual disability, learning disorder).
Multi-informant approach:
Rating scales must be completed by both parents/caregivers and teachers. Validated tools include:
- Conners' Rating Scales (Conners-3): separate parent and teacher forms; widely used in India.
- Vanderbilt ADHD Diagnostic Rating Scale: free, brief, validated for ages 6–12; has parent and teacher versions and includes screens for comorbidities.
- SNAP-IV: based on DSM symptoms; commonly used in research and clinical settings.
Differential Diagnosis: Many conditions can mimic ADHD, and several frequently co-exist with it:
| Condition | Key distinguishing features |
|---|---|
| Anxiety disorder | Inattention driven by worry/rumination; no hyperactivity-impulsivity; responds to anxiolytics |
| Learning disability (dyslexia, dyscalculia) | Inattention confined to specific academic tasks; cognitive testing shows specific processing deficit |
| Autism spectrum disorder | Social communication deficits, restricted interests, stereotyped behaviours; ADHD and ASD commonly co-occur |
| Intellectual disability | Global cognitive delay; IQ <70; ADHD can co-exist |
| Hearing or vision impairment | Apparent inattention due to sensory deficit; resolves with correction |
| Sleep disorders (OSA, restless legs) | Hyperactivity and inattention from sleep deprivation; improves with sleep treatment |
| Thyroid dysfunction (hyperthyroidism) | Restlessness, distractibility; TFT distinguishes |
| Absence epilepsy | Episodic staring spells; EEG shows 3 Hz spike-wave |
| Normal developmental variation | Below threshold; no impairment; age-appropriate overall |
Comorbidities are the rule, not the exception in ADHD:
- Oppositional Defiant Disorder (ODD): 40–60% of children with ADHD
- Conduct Disorder: 15–25%
- Anxiety disorders: 25–35%
- Learning disabilities (reading, writing, maths): 20–40%
- ASD: 30–50% (bidirectional comorbidity)
- Depression: 10–20%
CLINICAL PEARL
The video game paradox — use it to explain ADHD to families: Parents often object to the ADHD diagnosis by saying 'But he can focus for hours on video games!' This is actually consistent with ADHD, not evidence against it. Children with ADHD have deficient voluntary, sustained attention for low-stimulation tasks — but video games are designed with constant novelty, immediate reward, and high arousal, which provide external dopaminergic drive that partially compensates for the prefrontal deficit. The same child who cannot focus on homework for 10 minutes may play a video game for 3 hours. This distinction — intrinsically rewarding vs effortful tasks — is clinically and mechanistically important, and explaining it to parents transforms their understanding from 'my child is choosing not to focus' to 'my child's brain works differently for different types of tasks.'
SELF-CHECK
A 9-year-old girl is referred for poor academic performance. Her teacher reports she is quiet, dreamy, and rarely finishes her work, but is not disruptive. Her parents say she is inattentive at home too. There are no dysmorphic features, hearing is normal, and thyroid function tests are normal. Which diagnosis should you consider first?
A. Intellectual disability
B. Absence epilepsy
C. ADHD, predominantly inattentive presentation
D. Anxiety disorder
Reveal Answer
Answer: C. ADHD, predominantly inattentive presentation
This presentation is classic for ADHD predominantly inattentive presentation — quiet, dreamy, academically underperforming, inattentive in both school and home settings, but NOT hyperactive or disruptive. This presentation is commonly missed, especially in girls, because the child does not cause classroom disturbance. It is the most under-diagnosed ADHD subtype. Absence epilepsy would present with episodic brief staring spells (not pervasive inattention), and intellectual disability would show global developmental delay across all cognitive domains.