Page 8 of 17
PE4.1 | Attention Deficit Hyperactivity Disorder — SDL Guide (Part 2)
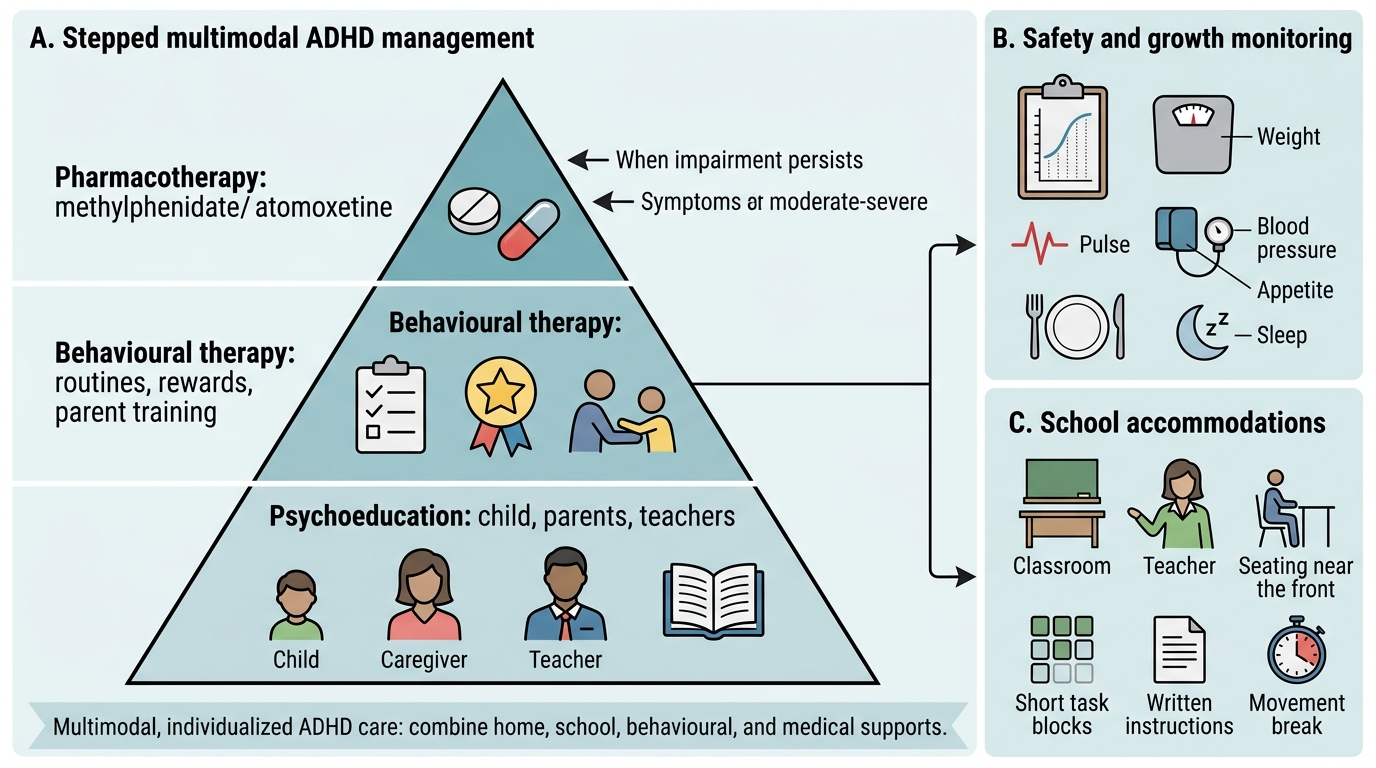
Management of ADHD
The management of ADHD is multimodal — no single intervention is sufficient. Evidence from the landmark MTA (Multimodal Treatment of ADHD) study showed that combined medication plus behavioural therapy produced the best outcomes for core ADHD symptoms and secondary social/academic difficulties. Management should be individualised, family-centred, and involve the school as an active partner.
1. Psychoeducation (the essential first step):
Every family must receive clear information about what ADHD is, what it is not, and what to expect from treatment. Key messages: ADHD is a neurobiological disorder, not a behavioural choice or parenting failure; it is treatable; most children with ADHD can succeed academically and socially with the right support. Psychoeducation significantly improves treatment adherence and reduces parental guilt and stigma.
2. Behavioural and psychological therapies:
- Behavioural parent training (BPT): Teaches parents how to use positive reinforcement, consistent consequences, clear instructions, and structured routines to manage ADHD behaviour at home. Evidence grade A for preschool-age children.
- Behavioural classroom management: Training teachers in token economies, seating (front of class, away from distractions), frequent breaks, and task chunking.
- Cognitive-Behavioural Therapy (CBT): Useful in older children and adolescents for managing impulsivity, emotional dysregulation, and low self-esteem.
- Social skills training: For children with significant peer relationship difficulties.
3. Pharmacotherapy:
Stimulants — first-line:
Methylphenidate (MPH) is the first-line pharmacological treatment for ADHD in children aged ≥6 years in India and globally. It acts by blocking the reuptake of dopamine and norepinephrine at presynaptic terminals, increasing their availability in the synapse. Available in immediate-release (IR, 3–5 hour duration) and extended-release (ER, 8–12 hour duration) formulations.
- Starting dose: 0.3 mg/kg/dose, titrated upward by 0.1 mg/kg increments every 1–2 weeks
- Maximum dose: ~1–2 mg/kg/day (or 60 mg/day in older children)
- Common adverse effects: decreased appetite (most common), insomnia, headache, stomachache, mild increase in heart rate and blood pressure
- Serious adverse effects: growth suppression with long-term use (monitor height/weight regularly), tics (may emerge or worsen), cardiovascular effects (screen for structural heart disease before starting)
- Contraindications: structural cardiac abnormalities, history of symptomatic arrhythmia, hyperthyroidism
Non-stimulants — second-line:
Atomoxetine is a selective norepinephrine reuptake inhibitor (SNRI). It is non-stimulant and non-scheduled (no addiction potential), making it preferred in children with comorbid anxiety, tic disorders, or where there is a risk of stimulant misuse.
- Dose: 0.5 mg/kg/day for 1 week, then increase to 1.2 mg/kg/day (target); maximum 1.8 mg/kg/day
- Onset: 4–6 weeks to full effect (much slower than methylphenidate)
- Common adverse effects: nausea, decreased appetite, fatigue, mood lability
- Black box warning: increased suicidal ideation in children and adolescents (monitor closely)
| Drug | Class | Mechanism | Onset | Key ADRs | Contraindications |
|---|---|---|---|---|---|
| Methylphenidate | Stimulant | DA/NE reuptake inhibitor | Days | Anorexia, insomnia, growth suppression, tics | Structural heart disease, hyperthyroidism |
| Atomoxetine | Non-stimulant SNRI | NE reuptake inhibitor | 4–6 weeks | Nausea, mood lability, suicidal ideation (BBW) | Glaucoma, MAO inhibitor use |
4. School accommodations (critical and often neglected):
- Seating in the front row, away from windows and distracting classmates
- Extended time for examinations
- Reduced homework load with task chunking
- Frequent brief breaks (5 minutes every 20–30 minutes)
- Preferential attention and positive reinforcement from teachers
- India's RPWD Act 2016 and the Rights of Children to Free and Compulsory Education (RTE) Act 2009 entitle children with ADHD to reasonable accommodations in school settings.
5. Monitoring:
Assess response to treatment every 3–6 months using the same rating scales as at diagnosis. Monitor height and weight (growth suppression risk with methylphenidate). Monitor blood pressure and heart rate. Reassess whether medication is still needed during school holidays ('drug holidays') — this also allows growth catch-up.
Multimodal Management of ADHD
SELF-CHECK
A 7-year-old boy with newly diagnosed ADHD (combined presentation) is started on methylphenidate. After 2 weeks, his mother reports his ADHD symptoms are better but he is not eating lunch and is losing weight. What is the most appropriate next step?
A. Stop methylphenidate immediately and switch to atomoxetine
B. Advise giving the dose after meals and offering a high-calorie snack before bedtime
C. Reduce the dose to zero for one week then restart
D. Order a full metabolic panel to investigate weight loss
Reveal Answer
Answer: B. Advise giving the dose after meals and offering a high-calorie snack before bedtime
Decreased appetite is the most common adverse effect of methylphenidate and typically occurs during peak drug effect (midday). The practical management is to give the medication after meals (to avoid appetite suppression during eating), provide a high-calorie breakfast before the morning dose, and offer a substantial snack/meal in the evening when the drug effect has worn off. Stopping methylphenidate immediately is not indicated for this common, manageable side effect. Weight and height should be monitored at every visit, and 'drug holidays' during school vacations can help with growth catch-up.
Self-Assessment
Apply your knowledge of ADHD diagnosis and management to the following clinical cases. These cases are designed to test your ability to apply DSM-5 criteria correctly, distinguish ADHD from its mimics, and formulate a management plan. Work through each case systematically: first identify which symptom domains are described, then check each DSM-5 criterion (symptom count, duration, onset age, pervasiveness, impairment, exclusions) before reaching a diagnosis. Resist the temptation to pattern-match to a label without completing the full criteria check — one of the most common errors in ADHD diagnosis is anchoring on one striking feature (e.g. hyperactivity) and failing to verify the remaining criteria. The second case deliberately introduces a comorbidity — notice how the presence of autism-spectrum features changes the management plan without invalidating the ADHD diagnosis.
Case 1: Priya, a 10-year-old girl, is referred for 'bad grades.' She is described by her teacher as quiet and well-behaved but 'not trying.' Her mother says she forgets homework daily, loses her pencil case constantly, and can never finish a task she starts — but 'can spend all afternoon reading her favourite novel.' There are no concerns at home about hyperactivity. IQ testing is normal. Hearing test is normal.
- Apply DSM-5 criteria: which symptom domains does Priya show? How many symptoms are present in each domain? Are the criteria for ADHD met? Which presentation?
- What rating scales would you use to formalise the assessment?
- What management would you offer first?
Case 2: Vikram, a 7-year-old, is brought by his parents because his teacher says he is 'uncontrollable' — he leaves his seat constantly, talks non-stop, and cannot wait his turn. At home his parents report the same. However, you also notice he does not make eye contact well, he speaks in long monologues about trains, and he becomes very distressed if his routine is changed.
- What additional diagnosis should you consider alongside ADHD?
- How does this affect your management plan?