Page 10 of 17
PE4.2 | Autism Spectrum Disorder — SDL Guide
Learning Objectives
- Describe the clinical features of autism spectrum disorder (ASD) across the two DSM-5 symptom domains with age-appropriate examples
- Explain the multifactorial aetiology of ASD including genetic, neurobiological, and environmental factors
- Apply the DSM-5 diagnostic criteria for ASD and identify appropriate screening and diagnostic tools
- Outline the evidence-based management of ASD including early intensive behavioural intervention, supportive therapies, and pharmacotherapy for comorbid symptoms
INSTRUCTIONS
Autism Spectrum Disorder (ASD) is a lifelong neurodevelopmental condition affecting approximately 1–2% of children in India. It is defined by persistent deficits in social communication and interaction combined with restricted, repetitive patterns of behaviour. ASD is not a single condition but a spectrum — from a minimally verbal child with severe intellectual disability to a highly verbal adult with exceptional abilities in a narrow domain. As a clinician you will encounter ASD in every setting, and your ability to recognise early warning signs, make a timely referral, counsel families compassionately, and co-ordinate access to early intervention will have a profound impact on the trajectory of affected children's lives.
References
- Ghai Essential Pediatrics, 9th ed., Ch 18 (Autism Spectrum Disorder) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 54 (Autism Spectrum Disorder) (textbook)
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5), 2013 — ASD criteria (classification)
- IAP Guidelines on Autism Spectrum Disorder, 2017 (guideline)
- Robins DL et al. M-CHAT-R/F: Modified Checklist for Autism in Toddlers, Revised with Follow-Up, 2014 (tool)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 2-year-old boy, Aarav, is brought to your clinic by his anxious parents. He used to say 'mama' and 'baba' but stopped speaking at 18 months. He does not point to things he wants and rarely makes eye contact — but he can spend 30 minutes lining up toy cars in a perfectly straight row, becoming intensely distressed if anyone moves them. He does not wave goodbye or look where you point. He seems 'in his own world.' His mother has been reading online: 'Doctor, my friend says the MMR vaccine caused this. Is that true?' Where do you begin?
WHY THIS MATTERS
Autism Spectrum Disorder (ASD) is the fastest-growing neurodevelopmental diagnosis worldwide. In India, studies report a prevalence of approximately 1–2% among school-age children, meaning an estimated 2–3 million Indian children are affected. For decades, ASD was misunderstood as a rare condition caused by cold, unloving parents — the now-discredited 'refrigerator mother' theory. Today we know it is a neurobiological disorder with strong genetic roots, and that early, intensive intervention — ideally beginning before age 3 — produces the greatest gains in language, social function, and independence. The clinician who recognises ASD early and connects a family to intervention can fundamentally alter the course of a child's life. The clinician who misses it, or who delays referral waiting for the child to 'come around,' closes a critical developmental window.
RECALL
Before studying ASD, consolidate key background knowledge:
• Joint attention (coordinating attention between a person and an object — pointing, showing, checking-back) emerges by 12–14 months and is absent or reduced in ASD.
• Social smile emerges at 6–8 weeks; response to name is expected by 12 months; absence of both are early red flags.
• Language milestones: first word with meaning ~12 months; 2-word phrases ~18–24 months; regression or plateau is always a red flag.
• Fragile X syndrome (X-linked CGG expansion) and tuberous sclerosis (TSC1/TSC2 mutations) are the most common identifiable genetic causes of ASD.
• MMR vaccine does NOT cause autism — the 1998 Wakefield study was retracted and Wakefield lost his medical license; over 10 large studies involving more than 1 million children have found no link.
Clinical Presentation of Autism Spectrum Disorder
Autism Spectrum Disorder (ASD) is defined by the DSM-5 as a neurodevelopmental disorder characterised by two core domains of difficulty: persistent deficits in social communication and social interaction (Domain A), and restricted, repetitive patterns of behaviour, interests, or activities (Domain B). Both domains must be present for the diagnosis; neither domain alone is sufficient. The shift from the older DSM-IV triad (social, communication, and repetitive behaviour as three separate domains) to the current dyad reflects neuroscientific evidence that social and communication deficits in autism are inseparable aspects of the same underlying impairment rather than independent features.
ASD presents very differently across individuals and across the lifespan — hence the word 'spectrum.' A toddler who does not point, does not respond to their name, and lines up toys is on the same spectrum as a university student who has memorised every train timetable in India but cannot maintain a reciprocal conversation. Understanding the spectrum's breadth prevents the common clinical error of 'ruling out autism' because a child makes eye contact or says a few words.
Domain A — Social Communication and Interaction Deficits (all three must be present):
1. Deficits in social-emotional reciprocity: Reduced sharing of interests, emotions, or affect; failure to initiate or respond to social interaction; poor back-and-forth conversation. Examples: does not bring objects to show parents; does not respond when called by name; talks AT others rather than WITH them.
2. Deficits in nonverbal communicative behaviours: Reduced or atypical eye contact, facial expressions, gestures, and body language; reduced pointing; failure to follow a point or a gaze (absent joint attention).
3. Deficits in developing, maintaining, and understanding relationships: Difficulty adjusting behaviour to social context; no interest in peer relationships; absence of imaginative play; preferring objects to people.
Domain B — Restricted, Repetitive Behaviours (at least two of four must be present):
1. Stereotyped or repetitive motor movements, use of objects, or speech: Hand flapping, rocking, spinning; lining up toys; echolalia (immediate repetition of words/phrases heard) or delayed echolalia; idiosyncratic phrases.
2. Insistence on sameness, inflexible adherence to routines, or ritualised patterns: Extreme distress at small changes (a different route to school, a moved object); rigid daily routines; ritualistic greeting behaviours.
3. Highly restricted, fixated interests that are abnormal in intensity or focus: Intense preoccupation with a narrow topic (train timetables, fans, a single TV character) to the exclusion of other activities.
4. Hyper- or hyporeactivity to sensory input: Apparent indifference to pain or temperature; intense aversion to specific textures, sounds, or lights; excessive smelling or touching of objects; fascination with lights or spinning objects.
Early red flags (any of these in a child under 2 years warrants immediate referral):
• No social smile by 2 months
• No response to own name by 12 months
• No pointing or waving by 12 months
• No single words by 16 months
• No 2-word spontaneous phrases by 24 months
• Any regression (loss of previously acquired language or social skills at any age)
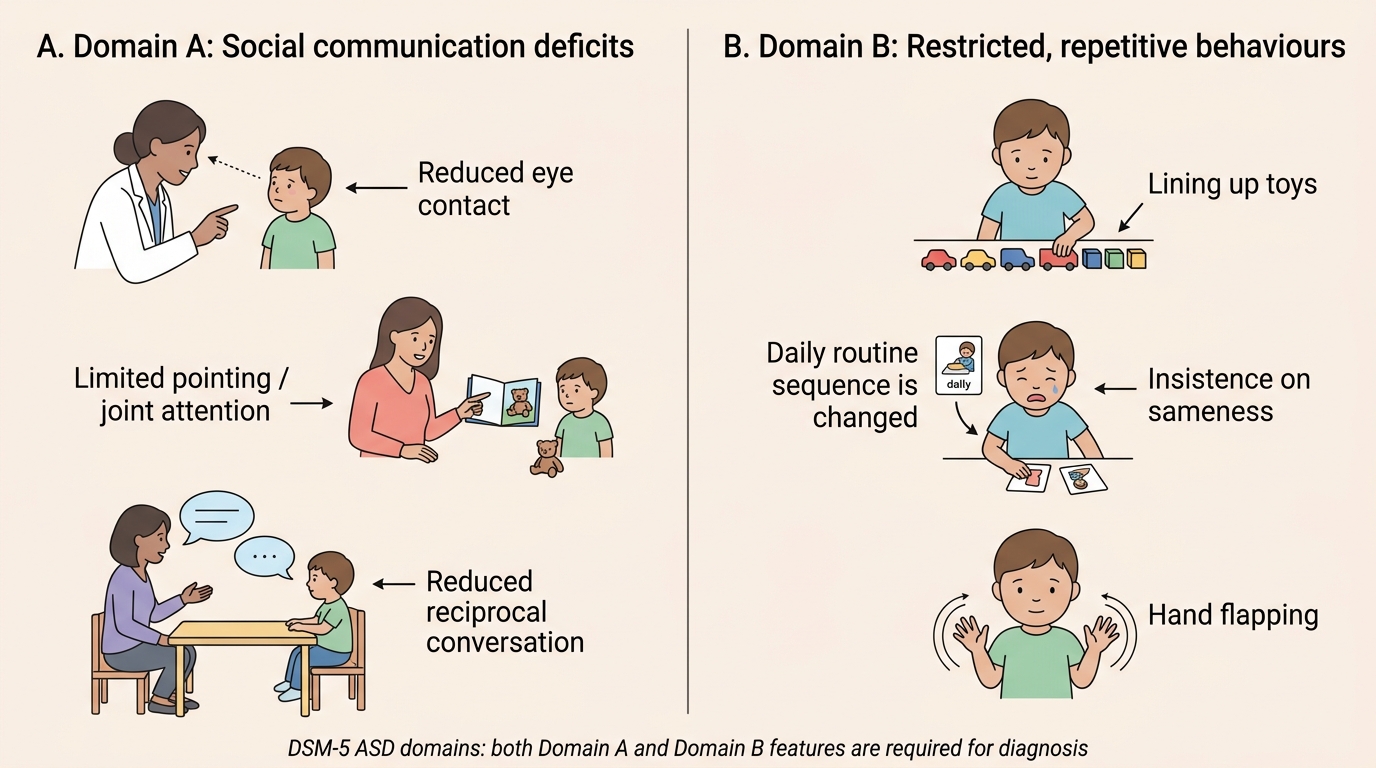
DSM-5 Autism Spectrum Disorder Domains
Pathophysiology and Aetiology of ASD
ASD is a multifactorial neurodevelopmental disorder with one of the highest heritability estimates in psychiatry. Its aetiology involves complex interactions between genetic predisposition, neurobiological development, and environmental modifiers — not a single cause, and certainly not vaccination, parenting style, or a child's diet. Understanding the aetiology serves three practical clinical purposes: it guides the decision to order genetic investigations (which can identify a syndromic cause and has implications for family counselling), it equips the clinician to address parental guilt and misconceptions about causation, and it informs prognosis given that the degree of genetic loading and co-occurring intellectual disability are the strongest predictors of long-term outcome.
Genetic aetiology (the dominant factor):
The heritability of ASD is estimated at 64–91% based on twin studies. If one monozygotic twin has ASD, the co-twin has a 60–90% concordance rate; for dizygotic twins, concordance is approximately 10–30%. Siblings of a child with ASD have approximately 10–20 times the population risk. No single gene causes ASD; it is a polygenic, complex disorder. However, certain genetic findings are clinically important:
- De novo mutations: New mutations not inherited from either parent, occurring in genes such as SHANK3 (encodes a scaffolding protein at excitatory synapses), CNTNAP2 (a neurexin family member), CHD8 (chromatin remodelling), and others, collectively account for approximately 10–15% of ASD cases.
- Copy number variants (CNVs): Chromosomal microdeletions or duplications, e.g. 16p11.2 deletion/duplication, are found in approximately 5–10% of ASD.
- Syndromic ASD: Identifiable chromosomal and single-gene syndromes that present with ASD as a feature:
• Fragile X syndrome (FMR1 CGG expansion) — the most common known inherited cause of ASD and intellectual disability
• Tuberous sclerosis complex (TSC1/TSC2) — ASD in ~50% of affected individuals
• Rett syndrome (MECP2 mutation, females) — regressive ASD phenotype
• 22q11.2 deletion syndrome (velocardiofacial syndrome) — ASD in ~15–25%
• Down syndrome — ASD in ~10–20%
Neurobiological basis:
Neuroimaging studies show atypical development of the social brain network — the interconnected regions that process faces, voices, intentions, and emotions: the superior temporal sulcus, fusiform face area, amygdala, and medial prefrontal cortex. In ASD, these regions show reduced activation during social tasks and atypical connectivity with each other. During the first year of life, the typical trajectory of developing social brain function appears to diverge in children who will later be diagnosed with ASD — before clinical symptoms are clearly apparent. The excitatory-inhibitory (E/I) imbalance hypothesis proposes that overgrowth of cortical excitatory neurons relative to inhibitory interneurons disrupts neural circuit function underlying social and language processing.
Environmental risk factors (modifiers, not causes):
- Advanced parental age (particularly paternal age ≥40) — associated with increased de novo mutations
- Prematurity — especially <28 weeks gestation
- Prenatal valproate exposure — antiepileptic drug that significantly increases ASD risk (2–10x); contraindicated in women of childbearing age where alternatives exist
- Prenatal infections (influenza, rubella) in the first trimester
- Air pollution exposure (preliminary evidence, under active research)
MMR vaccine does NOT cause ASD: The 1998 Wakefield paper in The Lancet was based on fraudulent data, was retracted in 2010, and Wakefield was struck off the medical register. Since then, studies totalling over 1.2 million children across multiple countries have found no causal link between the MMR vaccine and ASD. Vaccine hesitancy driven by this myth has led to resurgence of measles — a far more dangerous outcome. Proactively addressing this with every family of a child with ASD is a clinical and public-health obligation.
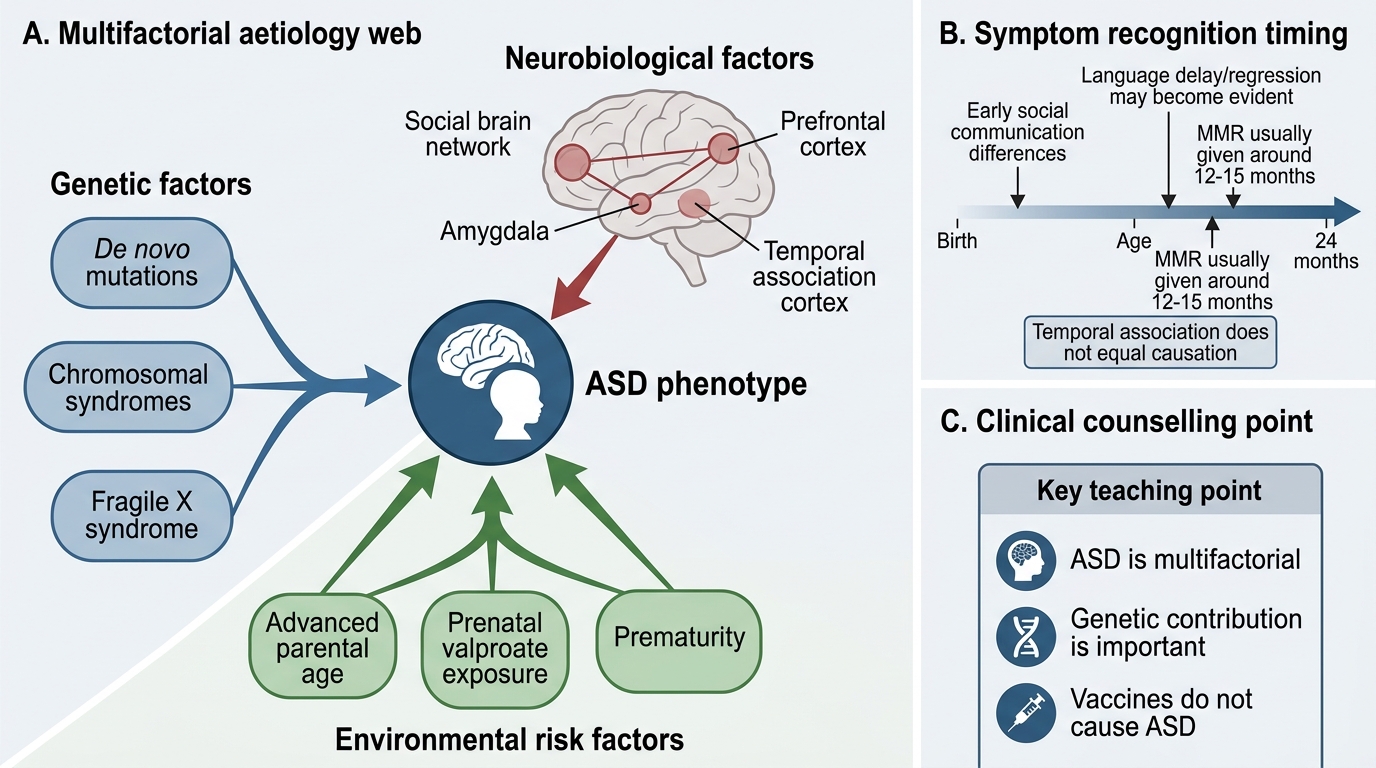
Multifactorial Aetiology of Autism Spectrum Disorder
SELF-CHECK
A parent of a child newly diagnosed with ASD insists that the MMR vaccine given at 15 months caused the autism, pointing to the fact that their child said a few words before the vaccine and stopped speaking shortly after. What is the most important point to address?
A. The MMR vaccine schedule should be delayed until after 2 years in at-risk children
B. The temporal coincidence of MMR and symptom recognition is explained by the fact that ASD symptoms typically become evident around 12–18 months, the same age as the MMR vaccine
C. The child likely had an adverse reaction to the measles component specifically
D. A thimerosal-free MMR formulation should be used for future siblings
Reveal Answer
Answer: B. The temporal coincidence of MMR and symptom recognition is explained by the fact that ASD symptoms typically become evident around 12–18 months, the same age as the MMR vaccine
The apparent link between MMR and ASD is a temporal coincidence, not causation. ASD symptoms — particularly language regression and loss of social engagement — become most apparent in the second year of life, precisely when the MMR vaccine is given. Multiple large studies (>1.2 million children) confirm no causal relationship. The Wakefield paper claiming the link was retracted and found to be fraudulent. MMR vaccination must continue as scheduled; vaccine hesitancy poses real risk of measles outbreaks.
Diagnosis of ASD
ASD is a clinical diagnosis made by a trained clinician using a combination of structured developmental history, direct behavioural observation, and standardised diagnostic instruments. There is no biomarker, blood test, or neuroimaging finding that confirms ASD. The diagnosis requires that both DSM-5 domains (A and B) are present, that symptoms began in the early developmental period, that they cause significant functional impairment, and that they are not better explained by intellectual disability or global developmental delay alone. The diagnostic process must also assess the level of support required (DSM-5 Levels 1–3) and identify comorbidities, because ASD without its comorbidities is the exception rather than the rule, and those comorbidities often drive more day-to-day impairment than the core ASD features themselves.
Step 1 — Developmental surveillance and screening:
All children should undergo universal developmental surveillance at every well-child visit. The M-CHAT-R/F (Modified Checklist for Autism in Toddlers, Revised with Follow-Up) is a validated, free, two-stage parent-report screening tool for ASD in children aged 16–30 months. A positive M-CHAT-R/F score warrants immediate referral for diagnostic evaluation without waiting for further surveillance.
Key red flags that warrant immediate referral at any age:
• No response to name by 12 months
• No pointing or waving by 12 months
• No single words by 16 months
• No 2-word spontaneous phrases by 24 months
• Any loss of previously acquired language or social skills
Step 2 — Diagnostic assessment:
The gold-standard diagnostic instruments are:
- ADOS-2 (Autism Diagnostic Observation Schedule, 2nd edition): A semi-structured, standardised observational assessment administered by a trained clinician; considered the gold standard for ASD diagnosis. Available in modules for different language levels (non-verbal to fluent speech).
- ADI-R (Autism Diagnostic Interview-Revised): A structured parent interview that covers developmental history from infancy; used alongside ADOS-2 for a comprehensive diagnostic picture.
- CARS-2 (Childhood Autism Rating Scale, 2nd edition): A simpler clinician-rated scale that can be used in lower-resource settings; requires only observation and interview.
DSM-5 Levels of Support (severity specifiers):
- Level 1 — Requiring support: Without supports in place, deficits in social communication cause noticeable impairment; difficulty initiating social interactions; atypical responses to social overtures.
- Level 2 — Requiring substantial support: Marked deficits in verbal and nonverbal communication; social impairments apparent even with supports in place; limited initiation of interactions.
- Level 3 — Requiring very substantial support: Severe deficits in verbal and nonverbal communication; very limited initiation of social interactions; minimal response to social overtures.
Differential Diagnosis:
| Condition | Key distinguishing features |
|---|---|
| ADHD | Inattention/hyperactivity dominant; social communication structurally intact; no restricted interests (ADHD and ASD commonly co-occur) |
| Intellectual disability | Global cognitive delay without necessarily the social communication profile or restricted interests of ASD |
| Language disorder (DLD) | Structural language deficit; social interaction motivation intact; no restricted interests |
| Rett syndrome | MECP2 mutation (females); stereotyped hand-wringing; regression after 6–18 months of normal development |
| Social (pragmatic) communication disorder | Social communication deficits without restricted/repetitive behaviours — cannot diagnose ASD if Domain B absent |
| Social anxiety disorder | Fear of negative evaluation; social avoidance; but desire for social relationships; onset often in adolescence |
Comorbidities in ASD (the rule, not the exception):
- Intellectual disability: ~30–50% of individuals with ASD
- ADHD: 30–50% (DSM-5 now permits co-diagnosis of both)
- Anxiety disorders: 40–50%
- Epilepsy: 20–30% (bimodal peak — early childhood and adolescence)
- Sleep disorders: 50–80%
- Gastrointestinal problems: 30–70%
- Language disorder: ~30% are minimally verbal
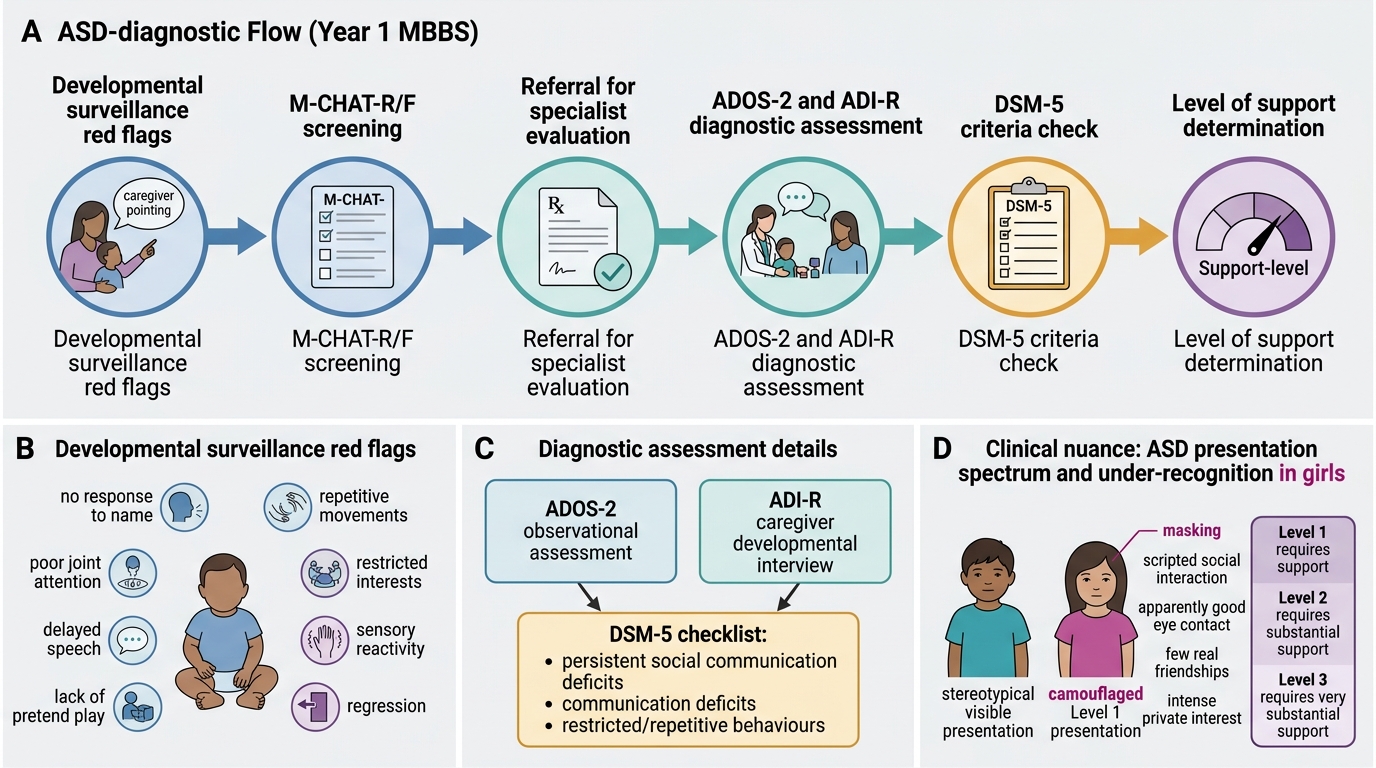
ASD Diagnostic Pathway
CLINICAL PEARL
ASD does not always look the same — and girls are systematically under-diagnosed: The classic ASD picture — the non-verbal boy with intense interests and poor eye contact — is real, but it is not the only picture. Girls with ASD frequently 'camouflage' or 'mask' their difficulties by imitating social behaviour they observe, scripting social interactions from memory, and hiding their restricted interests because they are socially unacceptable. A girl who makes eye contact, appears friendly, but has no real friends, follows social rules rigidly without understanding them, and has an intense private interest in, say, a specific fictional character may have ASD Level 1 that has gone unrecognised for years. The female-to-male diagnostic ratio in ASD is approximately 1:3–4, but true prevalence may be closer to 1:2 when masking is accounted for.
SELF-CHECK
A 3-year-old child with ASD has significant aggression and self-injurious behaviour (head-banging) that is disrupting family functioning. His core ASD symptoms (communication deficits, restricted interests) are unchanged. Which pharmacotherapy is most appropriate?
A. Methylphenidate to reduce hyperactivity contributing to aggression
B. Risperidone for irritability and aggression associated with ASD
C. A selective serotonin reuptake inhibitor (SSRI) to treat core ASD symptoms
D. Valproate as a mood stabiliser
Reveal Answer
Answer: B. Risperidone for irritability and aggression associated with ASD
Risperidone (an atypical antipsychotic) is FDA-approved for the treatment of irritability and aggression in children with ASD aged 5 years and above, and aripiprazole has a similar indication. These medications treat the comorbid irritability symptom cluster — they do NOT treat core ASD symptoms (social communication deficits, restricted interests). There is no approved medication for core ASD symptoms. SSRIs are sometimes used for co-occurring anxiety or repetitive behaviours but are not first-line for aggression. Methylphenidate can be used for co-occurring ADHD symptoms but does not address aggression as a primary target.