Page 11 of 17
PE4.2 | Autism Spectrum Disorder — SDL Guide (Part 2)
Management of ASD
There is no cure for ASD and no medication that treats its core features. However, early, intensive, individualised intervention can produce profound improvements in language, social function, adaptive behaviour, and quality of life. The evidence base for early intervention is clear and consistent: children who begin intensive intervention before age 3 — during the period of maximal neuroplasticity — show the greatest gains. Every month of delay in starting intervention has a cost. The management of ASD is therefore primarily about organising timely access to the right therapies and ensuring families have the knowledge and support to implement them at home.
1. Early Intensive Behavioural Intervention:
Applied Behaviour Analysis (ABA) — particularly the Early Intensive Behavioural Intervention (EIBI) model — is the most evidence-based intervention for ASD. The Lovaas (1987) study demonstrated that 40 hours per week of intensive ABA beginning before age 4 produced significant IQ gains and improved school placement in nearly half of treated children. ABA uses principles of reinforcement to systematically teach social, communication, and adaptive behaviour skills, and to reduce maladaptive behaviours. In India, intensive ABA is delivered in specialised therapy centres and should be supplemented with home-based implementation by trained parents. Lower-intensity ABA and naturalistic developmental behavioural interventions (NDBIs) such as JASPER and ESDM (Early Start Denver Model) are evidence-based alternatives for milder presentations.
2. Speech and Language Therapy:
Essential for all children with ASD, regardless of language level. For minimally verbal children, augmentative and alternative communication (AAC) strategies — picture exchange communication system (PECS), communication boards, and voice-output devices — can dramatically improve functional communication. For verbal children, therapy focuses on pragmatics (social use of language), narrative skills, and conversational reciprocity.
3. Occupational Therapy:
Addresses sensory processing difficulties (sensory integration therapy), fine motor skills, and activities of daily living. Many children with ASD have significant sensory sensitivities — loud sounds, specific textures, bright lights — that cause extreme distress; OT can develop sensory diets and environmental modifications.
4. Special Education:
Children with ASD benefit from structured, predictable learning environments with visual schedules, low sensory stimulation, and explicit social skills instruction. Under the RPWD Act 2016, children with ASD are entitled to an Individualized Education Plan (IEP) and inclusive education support in mainstream schools where appropriate.
5. Parent Training and Support:
Parents are the most important intervention agents in their child's life — they are present far more hours per week than any therapist. Training parents in naturalistic ABA principles, positive behaviour support, and augmentative communication strategies amplifies the effect of formal therapy many times over. Parent support groups (e.g., Action for Autism India, Autism Society India) provide peer support, advocacy, and access to resources.
6. Pharmacotherapy (for comorbid symptoms, NOT core ASD):
No medication treats the core features of ASD. Medications are used only for specific comorbid symptoms:
- Risperidone (5+ years) and aripiprazole: FDA-approved for irritability and aggression in ASD
- Methylphenidate/atomoxetine: for co-occurring ADHD symptoms
- SSRIs (fluoxetine, sertraline): for co-occurring anxiety or obsessive-compulsive symptoms (evidence modest; use with caution)
- Melatonin: for sleep onset insomnia (highly prevalent in ASD; good safety profile)
- Antiepileptics: for co-occurring epilepsy (20–30% of children with ASD)
7. Government entitlements in India:
ASD is a recognised disability under the RPWD Act 2016 (enacted in India), entitling affected individuals to: disability certificate, inclusive education with IEP, reservation in employment (in adulthood), and social protection. The National Trust Act 1999 provides legal guardianship and welfare schemes. RBSK provides free screening and referral for children with ASD from birth to 18 years.
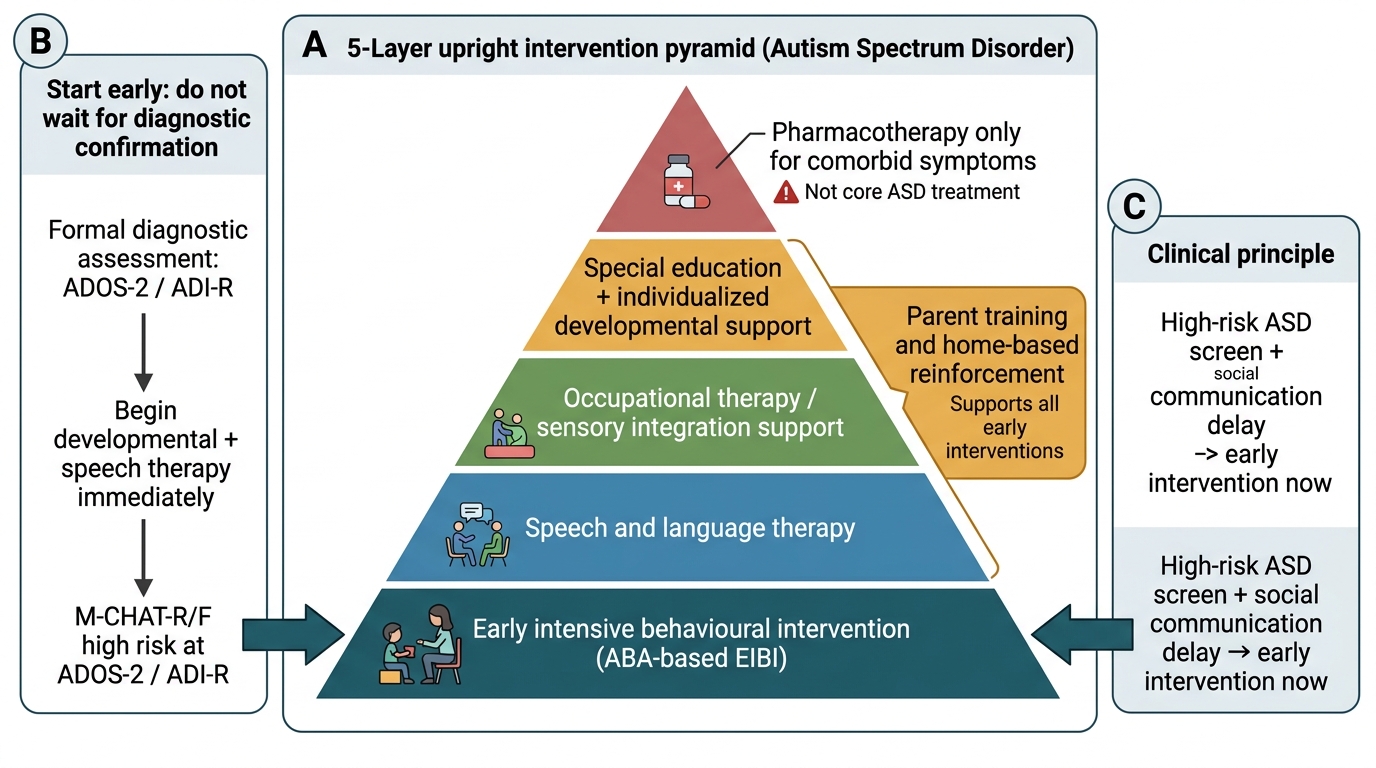
ASD Intervention Pyramid
SELF-CHECK
A 2-year-old child is identified as high-risk for ASD on the M-CHAT-R/F. The parents ask: 'Should we wait to start therapy until the diagnosis is confirmed?' What is the most appropriate response?
A. Yes — therapy should start only after a formal ADOS-2 diagnosis to ensure the right intervention is chosen
B. No — begin early developmental and speech therapy immediately; waiting for diagnostic confirmation wastes critical intervention time
C. Yes — but start only if the child has at least 3 clear ASD symptoms
D. No — but defer to a specialist before starting any intervention
Reveal Answer
Answer: B. No — begin early developmental and speech therapy immediately; waiting for diagnostic confirmation wastes critical intervention time
Do not wait for a confirmed ASD diagnosis to start early intervention. The diagnostic process (ADOS-2, ADI-R) can take weeks to months, especially in resource-limited settings. Since the evidence shows that the earlier intervention begins the better the outcome, and since speech therapy, developmental therapy, and ABA-based techniques are beneficial for any child with language or social-communication delay (regardless of ultimate diagnosis), early intervention should begin immediately upon identifying a concern. This is the 'diagnose and treat simultaneously' approach recommended by both IAP and AAP guidelines.
Self-Assessment
Apply your knowledge of ASD diagnosis and management to the following clinical cases. Work through each case using the DSM-5 two-domain framework: first check whether Domain A (social communication deficits) is present across all three subdomains, then check whether Domain B (restricted/repetitive behaviours) is present with at least two of the four criteria met. Only when both domains are present, onset is in the early developmental period, and there is significant functional impairment — and other diagnoses have been systematically considered — should the diagnosis of ASD be applied. Pay particular attention to the second case, which raises the clinical question of co-occurring ASD and intellectual disability, a pairing that has significant implications for the level of support required and for educational placement.
Case 1: Meera is a 3-year-old girl brought by her parents. She does not speak, does not respond to her name, does not point or gesture, and shows no interest in other children. She lines up her dolls in order every day and becomes inconsolably distressed if they are moved. She rocks back and forth when excited. On examination there are no dysmorphic features. Hearing assessment is normal. DQ on DASII is in the intellectual disability range.
- Which DSM-5 domains of ASD are present? Is ASD level 2 or 3 appropriate here?
- What investigations would you order to look for a genetic cause?
- What management would you initiate today — before diagnostic confirmation?
Case 2: Arjun is a 10-year-old boy brought for 'school problems.' He is highly verbal, reads encyclopaedias for pleasure, and can recite every cricket statistic since 1975. However, his teacher reports he has no friends, does not understand jokes, cannot work in a group, and becomes agitated when the school timetable changes. His parents report he has always been 'different' but very 'bright.'
- Which DSM-5 presentation does Arjun most likely represent (and which DSM-IV label does this correspond to)?
- What level of support does he likely require?
- How would you explain the diagnosis to his parents, who see his abilities and are surprised by the diagnosis?