Page 1 of 17
PE3.1-3 | Developmental Delay — SDL Guide
Learning Objectives
- Define developmental delay and intellectual disability and distinguish between global and domain-specific delay
- Describe the causes of developmental delay under prenatal, perinatal, and postnatal categories including chromosomal, genetic, structural, infective, and metabolic aetiologies
- Apply a structured clinical approach to a child presenting with developmental delay including history, examination, developmental assessment tools, and targeted investigations
- Counsel parents of a child with developmental delay regarding diagnosis, prognosis, early intervention, and support services
INSTRUCTIONS
Developmental delay is one of the most common reasons for paediatric consultation in India, affecting approximately 3–5% of children under five years. Recognising delay early and identifying its cause is essential because many conditions — congenital hypothyroidism, phenylketonuria, lead toxicity, hearing loss — respond to timely intervention that can prevent or minimise intellectual disability. This module equips you to define the condition, reason through its causes, conduct a structured clinical assessment, and counsel families with clarity and sensitivity.
References
- Ghai Essential Pediatrics, 9th ed., Ch 2 (Growth and Development) and Ch 18 (Developmental Paediatrics) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 38–40 (Developmental-Behavioural Paediatrics) (textbook)
- IAP Guidelines on Developmental Delay and Intellectual Disability, 2022 (guideline)
- Developmental Assessment Scale for Indian Infants (DASII), revised 2017 (tool)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A mother brings her 3-year-old son Arjun to the outpatient clinic. He is not yet speaking in sentences — he uses only a few isolated words — and he still cannot walk steadily without support. The mother reports a normal pregnancy, though the delivery was prolonged and required forceps assistance. She is anxious: 'All the other children in the neighbourhood are talking and running. What is wrong with my child?' You look at Arjun and notice he makes little eye contact, does not point to objects, and seems absorbed in his own world. Where do you begin?
WHY THIS MATTERS
Developmental delay affects an estimated 3–5% of Indian children under five years, making it one of the most frequently encountered problems in paediatric outpatient clinics. Yet it is also one of the most frequently missed: a child who 'seems slow' may wait years for a diagnosis, during which the critical window for early intervention closes. The earlier a cause is identified — a metabolic disorder, a sensory deficit, a treatable infection sequela — the better the neurodevelopmental outcome. As a final-year medical student and future clinician, your ability to recognise developmental red flags, structure an assessment, and communicate clearly with distressed parents will directly shape the lives of affected children and their families.
RECALL
Before studying delay, recall the key developmental milestones from your PE-foundation study:
• Gross motor: neck control ~3 months; sits without support ~6–8 months; stands with support ~9 months; walks alone ~12–15 months.
• Fine motor: palmar grasp ~3–4 months; pincer grasp ~9 months; scribbles with crayon ~18 months.
• Language: cooing ~2 months; babbling ~6 months; first word with meaning ~12 months; 2-word sentences ~18–24 months.
• Social/adaptive: social smile ~6–8 weeks; stranger anxiety ~6–8 months; parallel play ~2 years.
Also recall that the brain undergoes rapid myelination and synaptic pruning during the first three years — this explains both the vulnerability to insults and the potential for compensatory plasticity with early intervention.
Clinical Presentation of Developmental Delay
Developmental delay is defined as failure to attain expected developmental milestones for a given chronological age in one or more domains. When delay is present in two or more domains simultaneously in a child under five years, it is termed global developmental delay (GDD). The term intellectual disability (ID) is used when, after formal assessment at an appropriate age (generally ≥5 years), a child demonstrates both a significantly below-average intellectual ability (IQ <70) and substantial deficits in adaptive functioning, with onset before age 18 years.
Provided image
Children with developmental delay present in several ways. A parent may notice that their child is not reaching milestones compared to siblings or peers. A health worker at an immunisation clinic or growth-monitoring camp may screen and flag a concern. Less often, the child presents with an unrelated complaint and delay is incidentally detected on routine developmental surveillance.
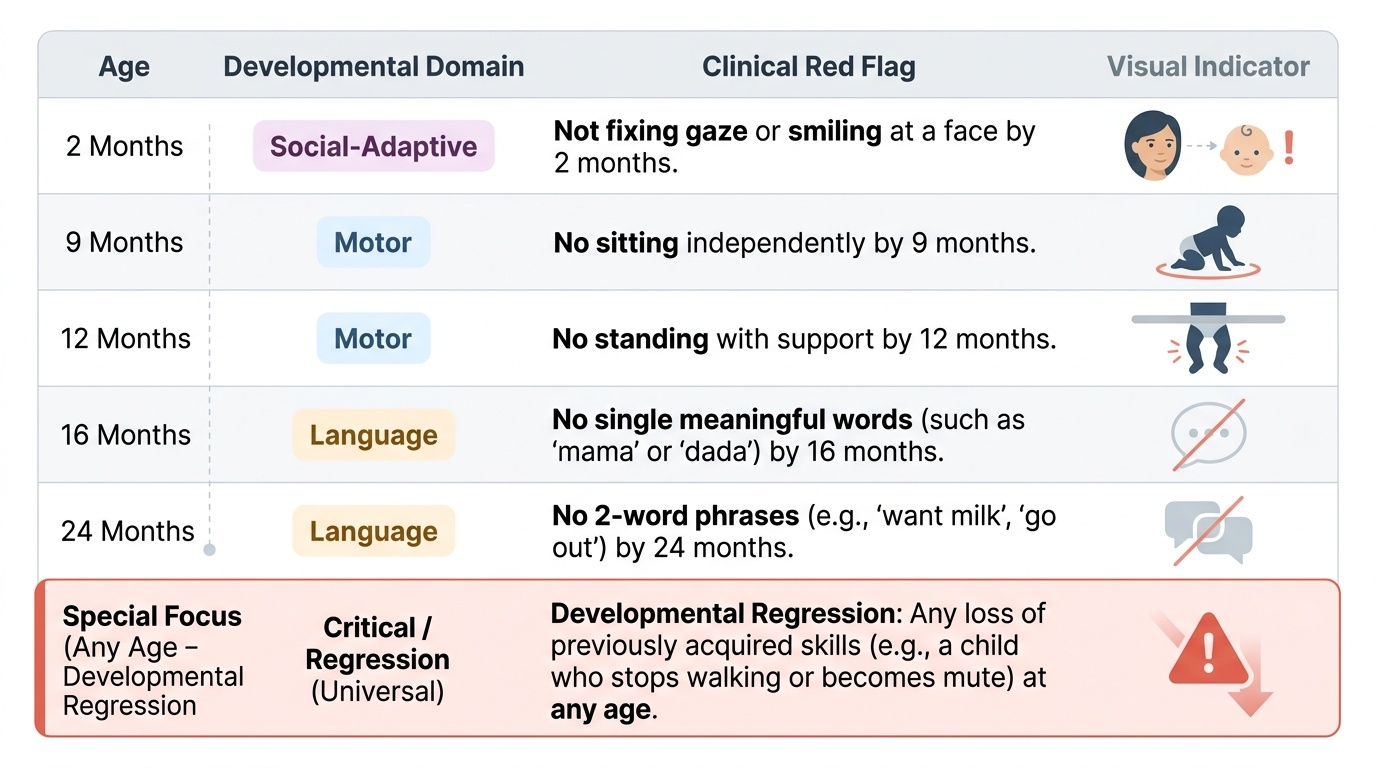
Recognising red flags is the clinical skill that separates early detection from missed diagnosis. Key red flags include:
• Not fixing gaze or smiling at a face by 2 months
• No sitting by 9 months
• No standing with support by 12 months
• No single meaningful words by 16 months
• No 2-word phrases by 24 months
• Any loss of previously acquired skills (developmental regression) at any age — this is a critical red flag requiring urgent evaluation
Regression deserves special emphasis: a child who was walking and then stops walking, or who was saying words and then becomes mute, suggests a neurodegenerative disorder and demands immediate investigation — it is never 'normal'.
Developmental delay should be distinguished from developmental variation (within-normal-limits individual variation in milestone timing), motor disorders such as cerebral palsy (where intellectual function may be spared), and isolated sensory deficits (hearing or vision impairment that may mimic language or developmental delay without primary CNS involvement).
Pathophysiology and Aetiology of Developmental Delay
Understanding the cause of developmental delay requires thinking in terms of timing of the insult to the developing brain. The classical framework for organising the causes of developmental delay divides them into prenatal, perinatal, and postnatal categories, reflecting when the brain was exposed to the damaging event. This temporal framing is clinically useful because it guides both the history-taking process and the selection of investigations — the timing of an antenatal infection, the circumstances of a difficult delivery, or the occurrence of a post-neonatal meningitis each points toward a distinct investigative pathway. Prenatal causes collectively account for the majority of identifiable aetiologies, while perinatal events — particularly birth asphyxia and its sequelae — are historically over-attributed and in reality responsible for only 10–15% of cases. Postnatal causes are especially important to identify because many are preventable or treatable, and because the brain retains considerable plasticity during early childhood.
Prenatal causes account for the majority of cases with identifiable aetiology:
- Chromosomal disorders: Down syndrome (trisomy 21) is the most common chromosomal cause. Fragile X syndrome is the most common single-gene (X-linked) inherited cause of intellectual disability. Turner, Klinefelter, and other aneuploidies also contribute.
- Structural brain malformations: Anencephaly, lissencephaly, pachygyria, holoprosencephaly — often due to errors in neuronal migration or cortical organisation during the first and second trimesters.
- TORCH infections: Toxoplasma, Rubella, Cytomegalovirus (CMV), Herpes simplex, and others that infect the fetus transplacentally, causing periventricular calcifications, microcephaly, and sensorineural hearing loss.
- Toxic and teratogenic exposures: Alcohol (fetal alcohol syndrome is the leading preventable cause of intellectual disability worldwide), phenytoin, isotretinoin, maternal iodine deficiency (cretinism).
- Inborn errors of metabolism: Phenylketonuria (PKU), galactosaemia, maple syrup urine disease, Gaucher disease — many are detectable by newborn screening; untreated, they cause progressive neurological damage.
Perinatal causes:
- Birth asphyxia / hypoxic-ischaemic encephalopathy (HIE): Inadequate oxygen delivery to the neonatal brain during labour/delivery; leads to neuronal death in watershed zones.
- Prematurity and its complications: Periventricular leukomalacia (PVL), intraventricular haemorrhage (IVH) are well-recognised antecedents of cerebral palsy and developmental delay in preterm infants.
- Neonatal hyperbilirubinemia (kernicterus): Unconjugated bilirubin deposition in the basal ganglia causes athetoid cerebral palsy and hearing loss.
- Neonatal hypoglycaemia and hypocalcaemia: Metabolic disturbances in the first hours/days of life can cause brain injury if severe and prolonged.
Postnatal causes:
- CNS infections: Bacterial meningitis, viral encephalitis — sequelae include hydrocephalus, hearing loss, epilepsy, and intellectual disability.
- Traumatic brain injury and non-accidental injury.
- Lead toxicity: Chronic lead exposure — from soil, paint, water (especially in old pipes), kite thread — causes cognitive impairment and behavioural problems; blood lead level >5 µg/dL warrants action per CDC current reference value.
- Severe malnutrition and psychosocial deprivation: Protein-energy malnutrition and environmental neglect in early childhood impair synaptic development and cognitive potential.
- Congenital hypothyroidism (if not detected and treated by neonatal screening): A fully treatable cause of intellectual disability.
Approximately 30–50% of cases of developmental delay and intellectual disability remain without an identifiable aetiology even after thorough investigation — this is important to communicate to families to avoid prolonged, futile investigative cycles.
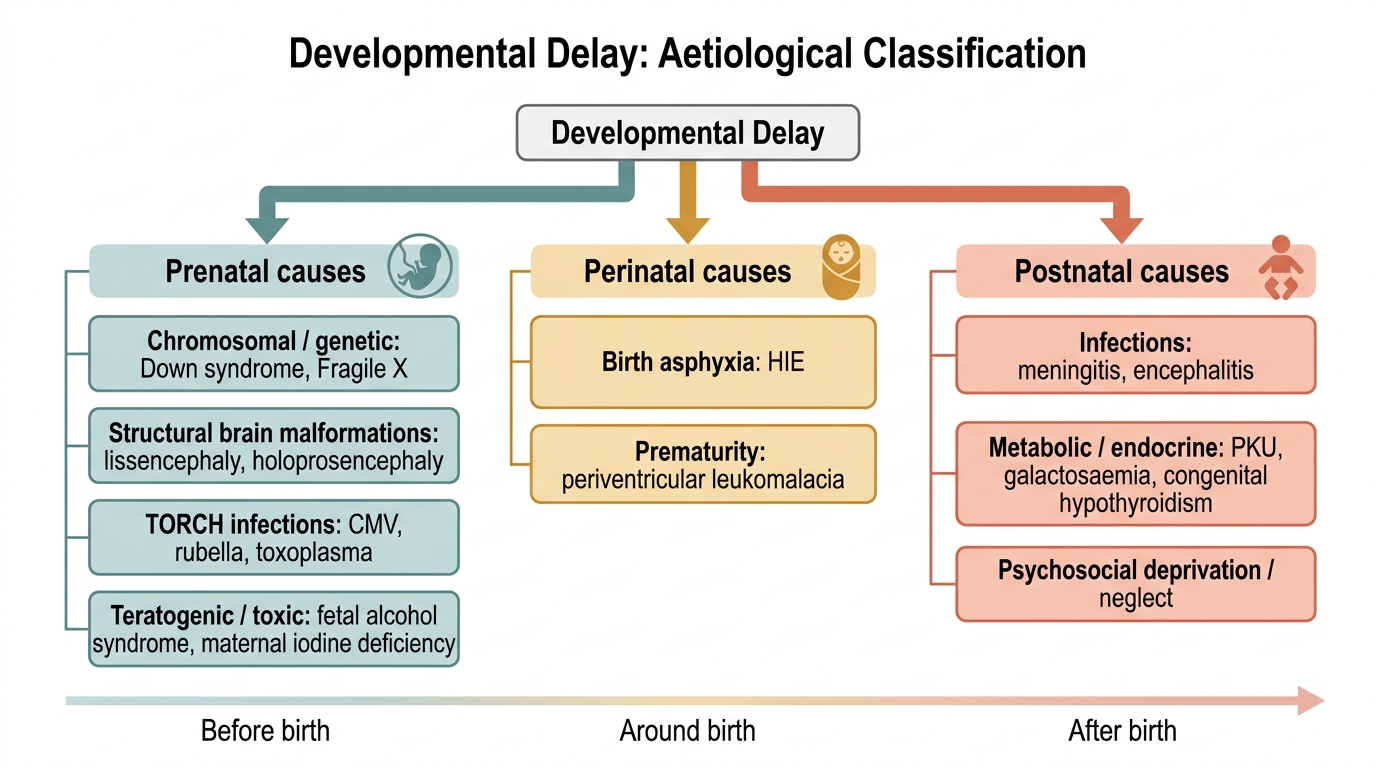
Aetiological Classification of Developmental Delay
| Timing | Category | Common Examples |
|---|---|---|
| Prenatal | Chromosomal | Down syndrome (trisomy 21), Fragile X |
| Prenatal | Structural brain | Lissencephaly, holoprosencephaly |
| Prenatal | TORCH infections | CMV, rubella, toxoplasma |
| Prenatal | Teratogenic/toxic | Fetal alcohol syndrome, maternal iodine deficiency |
| Prenatal | Metabolic/genetic | PKU, galactosaemia, congenital hypothyroidism |
| Perinatal | Asphyxia | HIE, periventricular leukomalacia |
| Perinatal | Prematurity | IVH, PVL |
| Perinatal | Metabolic | Kernicterus, hypoglycaemia |
| Postnatal | Infections | Meningitis, encephalitis |
| Postnatal | Toxic | Lead poisoning |
| Postnatal | Nutritional/psychosocial | Severe malnutrition, deprivation |
SELF-CHECK
A 2-year-old child previously achieving normal milestones begins to lose previously acquired speech and motor skills over 6 months. What is the most important clinical distinction to make?
A. Global developmental delay
B. Developmental regression requiring urgent investigation
C. Language delay isolated to expressive speech
D. Autism spectrum disorder
Reveal Answer
Answer: B. Developmental regression requiring urgent investigation
Developmental regression — the loss of previously acquired skills — is a critical red flag that is never normal and demands urgent neurological evaluation for neurodegenerative disorders, metabolic diseases, or structural brain pathology. It is distinct from simple developmental delay (failure to progress) and must prompt immediate investigation rather than 'watchful waiting'.
Approach to Diagnosis and Investigation
The clinical approach to a child with suspected developmental delay is systematic and must be conducted in a structured manner, because developmental delay is not a single diagnosis but a presentation with many possible underlying causes. A thorough evaluation integrates four components: a detailed history, a targeted physical and neurological examination, a standardised formal developmental assessment, and directed investigations guided by clinical findings. The fundamental goals are to confirm that delay is genuinely present (and not a reflection of environmental deprivation alone), to characterise which developmental domains are affected and how severely, to identify the underlying aetiology, and to screen for comorbidities such as epilepsy, sensory deficits, and behavioural disorders that commonly coexist with developmental delay. No investigation should be ordered without a clinical reason, and no child with a positive screening test should leave the clinic without a concrete follow-up plan and a referral to early intervention services.
History:
- Perinatal and birth history: gestational age, mode of delivery, birth weight, birth asphyxia (need for resuscitation, Apgar scores), neonatal complications (jaundice, hypoglycaemia, sepsis).
- Developmental history: exact age of attaining each milestone; any period of normal development followed by loss (regression).
- Medical history: CNS infections, seizures, head trauma, chronic illnesses, drug exposures, lead exposure risk (chewing on painted surfaces, living near industrial sites).
- Nutritional history: breastfeeding, complementary feeding, dietary adequacy.
- Family history: consanguinity (increases risk of autosomal recessive metabolic disorders), relatives with intellectual disability, unexplained deaths in infancy.
- Antenatal history: maternal infections (TORCH), substance use (alcohol, drugs), medications, thyroid disease, iodine deficiency.
- Social and environmental history: socioeconomic status, caregiver involvement, psychosocial deprivation.
Examination:
- General: dysmorphic features (Down syndrome facies, large ears of Fragile X, café-au-lait spots of neurofibromatosis), skin lesions (hypopigmented macules of tuberous sclerosis), abnormal hair or nails.
- Anthropometry: weight, height, head circumference (microcephaly <−2 SD, macrocephaly >+2 SD).
- Neurological: tone (hypotonia or hypertonia), deep tendon reflexes, primitive reflexes, cerebellar signs, cranial nerve examination, fundoscopy (papilloedema, retinal lesions in CMV).
- Developmental assessment: a hands-on, age-appropriate assessment of gross motor, fine motor-adaptive, language, and social domains.
Standardised Developmental Assessment Tools:
- DASII (Developmental Assessment Scale for Indian Infants): a standardised, norm-referenced tool developed and validated on Indian children, covering ages 0–30 months. It is preferred in the Indian context over Western norms.
- Denver Developmental Screening Test II (DDST-II): widely used screening tool for ages 0–6 years; covers personal-social, fine motor-adaptive, language, and gross motor.
- Vineland Adaptive Behavior Scales: used to assess adaptive functioning, particularly when intellectual disability is suspected.
Investigations (targeted, not shotgun):
- First-line: thyroid function tests (TSH, T4), blood lead level, haemogram, serum calcium/phosphate/glucose, hearing assessment (Brainstem Evoked Response Audiometry — BERA), vision assessment, urine metabolic screen.
- Neuroimaging: MRI brain (preferred over CT for soft tissue and myelination assessment); CT only if MRI unavailable or for calcifications (TORCH).
- Chromosomal/genetic: karyotype (if dysmorphic features), chromosomal microarray (copy number variants), targeted gene panels (Fragile X FMRP PCR).
- Metabolic screen: tandem mass spectrometry (TMS) for amino acidopathies, organic acidaemias, fatty acid oxidation defects — particularly if regression is present or if newborn screening was not done.
- EEG: if seizures are present or suspected.
INVESTIGATION PRINCIPLE: Investigations should be guided by the clinical findings. A child with dysmorphic features gets a karyotype; a child with skin lesions gets neuroimaging; a child with suspected regression gets a metabolic screen. Routine 'developmental delay panels' without clinical reasoning waste resources and delay the specific diagnosis.
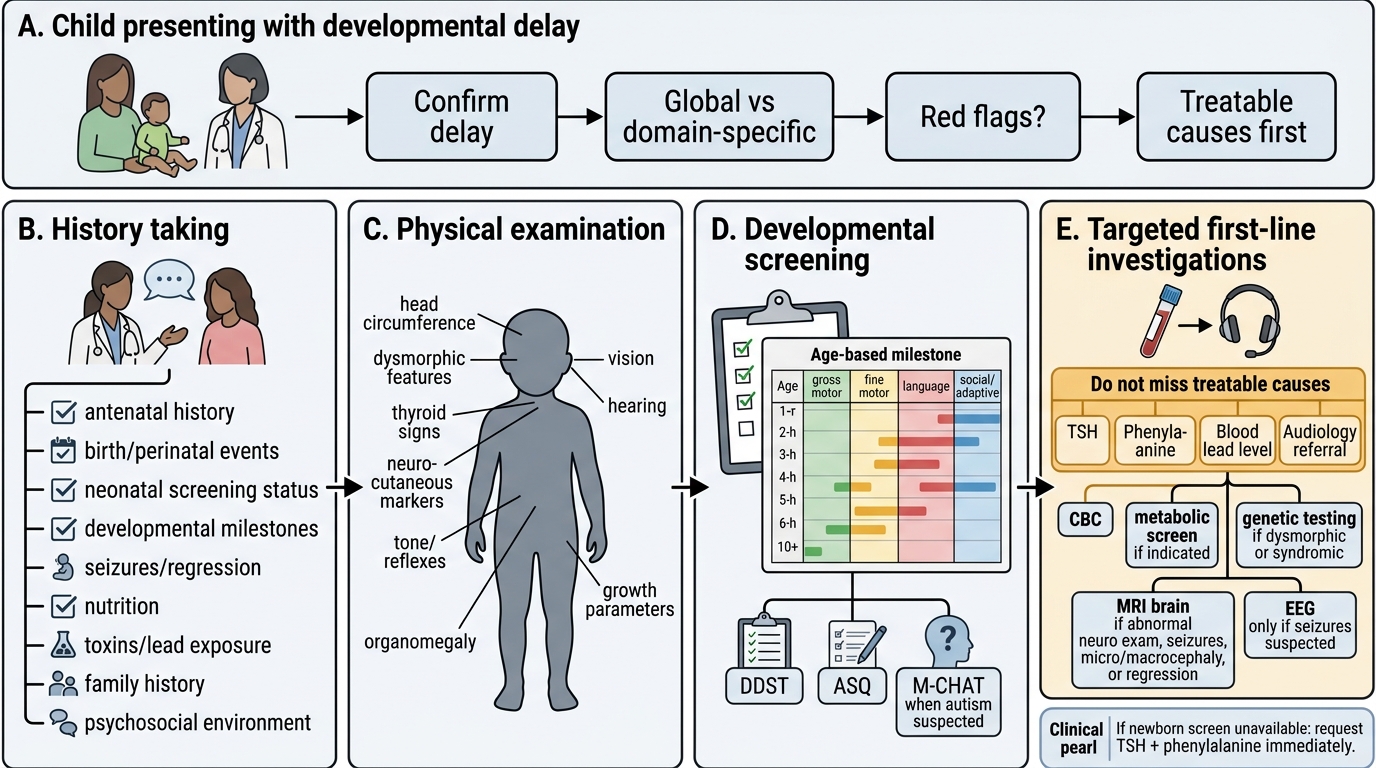
Diagnostic Algorithm for Developmental Delay
CLINICAL PEARL
Don't miss the treatable causes: Congenital hypothyroidism and phenylketonuria are included in India's Rashtriya Bal Swasthya Karyakram (RBSK) newborn screening programme. If a child presents with developmental delay and newborn screening was NOT done or results are unavailable, request TSH and phenylalanine levels immediately — these are completely preventable causes of intellectual disability when treated early. Similarly, hearing impairment causing apparent language delay is easily identified with an audiology referral and fitted with hearing aids: this is developmental delay that 'vanishes' with the correct intervention.
SELF-CHECK
Which of the following is the MOST appropriate first-line investigation for a 2-year-old with global developmental delay, no dysmorphic features, and no known perinatal complications?
A. MRI brain
B. Chromosomal karyotype
C. Thyroid function tests and blood lead level
D. EEG
Reveal Answer
Answer: C. Thyroid function tests and blood lead level
Thyroid function tests and blood lead level are among the first-line investigations for unexplained global developmental delay without dysmorphic features because congenital hypothyroidism (if untreated) and lead toxicity are common, treatable causes. More expensive or invasive investigations (MRI, karyotype, EEG) are targeted based on specific clinical pointers (e.g., dysmorphic features → karyotype; seizures → EEG; abnormal neurological exam → MRI).