Page 10 of 17
PE5.4 | Enuresis — SDL Guide
Learning Objectives
- Define enuresis and classify it into primary vs secondary and nocturnal vs diurnal types.
- Explain the three principal pathophysiological mechanisms of monosymptomatic nocturnal enuresis.
- Identify organic causes of enuresis and outline the appropriate investigations to exclude them.
- Describe the management of enuresis, including non-pharmacological therapies, desmopressin, and the limited role of imipramine.
INSTRUCTIONS
Enuresis — involuntary urinary incontinence — is one of the most common problems encountered in paediatric practice, affecting about 15–20% of 5-year-olds and generating significant distress for children and families. A confident clinical approach, built on understanding the normal developmental trajectory of bladder control and the three key pathophysiological mechanisms, enables the paediatrician to identify the rare child with an organic cause, reassure the majority with benign primary nocturnal enuresis, and prescribe effective evidence-based treatment.
References
- Ghai Essential Pediatrics, 9th ed., Ch 17 (Behavioural Problems) and Ch 22 (Urinary System) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 554 (Enuresis) (textbook)
- International Children's Continence Society (ICCS) Standardisation Document on Enuresis, 2014 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old boy is brought to your clinic by his mother, who is increasingly distressed: 'He wets the bed almost every night — we have tried everything. He is too embarrassed to go for a school camp.' The boy has never had a dry month in his life and has no daytime wetting, no dysuria, and no thirst. He is otherwise healthy with normal growth and development. His urine dipstick is clear. His mother asks: 'Is something wrong with his kidneys? Will he grow out of it? Is there a tablet that will help?' How do you classify this child's problem, what is the most likely mechanism, and what is your treatment plan?
WHY THIS MATTERS
Enuresis affects approximately 5–10 million children in India and is one of the three most common chronic conditions of childhood alongside asthma and obesity. Despite this prevalence, it is frequently under-reported because of the stigma and embarrassment that surround it — many families delay seeking help for years, and children suffer significant loss of self-esteem, social restriction, and family stress. The condition is also frequently over-investigated (unnecessary renal imaging) or over-treated (inappropriate antibiotic courses for assumed UTI). Understanding the condition precisely — its definition, classification, mechanisms, and evidence-based treatments — enables the paediatrician to deliver rapid, effective, and reassuring care. Secondary enuresis, in particular, is an important red flag that must not be attributed to simple developmental variation.
RECALL
Before proceeding, recall:
• Normal bladder control development: daytime dryness normally achieved by age 2–3 years; nighttime dryness by age 4–5 years; bedwetting is entirely normal before 5 years.
• ADH (antidiuretic hormone, vasopressin): secreted by the posterior pituitary; concentration peaks during sleep, reducing nocturnal urine production; acts on collecting duct aquaporin-2 channels.
• Functional bladder capacity: the maximum volume of urine a child can hold before urgency; increases with age; reduced capacity → more frequent, smaller voids.
• DDAVP (desmopressin): synthetic analogue of ADH; used to reduce nocturnal urine production; hyponatraemia is the key adverse effect if fluid restriction is not observed.
• Urinalysis as screen: glucose in urine = diabetes mellitus; nitrites + leucocytes = UTI; specific gravity reflects ADH action.
Clinical Presentation and Classification of Enuresis
Enuresis is defined as involuntary voiding of urine beyond the developmental age at which bladder control is expected. It is not diagnosed before the age of 5 years (the accepted threshold beyond which bedwetting is considered a clinical problem rather than a developmental variation). The condition affects approximately 15–20% of 5-year-olds, 5% of 10-year-olds, and 1–2% of adolescents — reflecting a strong tendency toward spontaneous resolution of approximately 15% per year. Despite this natural course, the psychological impact on the child (shame, avoidance of sleepovers and school camps, reduced self-esteem) and on the family (parental frustration, sleep disruption, laundry burden) is substantial and fully justifies active clinical assessment and management.
Provided image
The clinical classification of enuresis uses two independent axes:
Axis 1 — Timing:
- Nocturnal enuresis: involuntary voiding during sleep; by far the most common form.
- Diurnal (daytime) enuresis: involuntary voiding while awake; more often organic or associated with overactive bladder.
- Combined: both nocturnal and diurnal; warrants more thorough investigation.
Axis 2 — History:
- Primary enuresis: the child has never been continuously dry at night for more than 6 months; represents 80–85% of nocturnal enuresis cases; more likely to be functional/developmental.
- Secondary enuresis: the child was dry for ≥6 months and then relapsed; accounts for 15–20%; almost always has a precipitant — psychological stress (new sibling, parental separation, school transition), urinary tract infection, diabetes mellitus, or, rarely, neurological disorder. Secondary enuresis must always be investigated.
Monosymptomatic nocturnal enuresis (MNE) is the most common clinical subtype: nocturnal wetting only, with no daytime symptoms (no urgency, frequency, or daytime incontinence) and no organic cause. This is the 'classical' bedwetting scenario and carries an excellent prognosis. Non-monosymptomatic enuresis (with daytime symptoms) suggests overactive bladder or other pathology and requires more detailed evaluation.
Aetiology and Pathophysiology
The aetiology of enuresis is multifactorial and, in the vast majority of children with monosymptomatic nocturnal enuresis, one or more of three functional mechanisms can be identified. Recognising the dominant mechanism in an individual child guides treatment selection. A strong genetic component underlies MNE — concordance in identical twins is approximately 77%, and if one parent had enuresis, the child has a 40% risk; if both parents were affected, the risk rises to approximately 77%. This genetic predisposition is thought to operate through all three functional mechanisms below.
Mechanism 1 — Reduced nocturnal ADH secretion (nocturnal polyuria):
Normally, ADH secretion rises during sleep, concentrating the urine and reducing nocturnal urine production to within the bladder's capacity. Many children with MNE lack this physiological nocturnal ADH surge, producing large volumes of dilute urine during sleep (nocturnal polyuria) that exceed bladder capacity and cause wetting. This is the most common mechanism in MNE and explains the efficacy of desmopressin (synthetic ADH), which restores the missing nocturnal ADH effect.
Mechanism 2 — High arousal threshold (deep sleep):
A child with a normal bladder capacity and normal urine production who nevertheless does not wake when their bladder is full has a high arousal threshold — they sleep deeply enough that the sensory signal from a full bladder fails to reach wakefulness. This is NOT a disorder of sleep architecture (sleep studies show no consistent abnormality); it is a maturational variation. The enuresis alarm works by conditioning the arousal response to the sensation of wetness, and is particularly effective in this group.
Mechanism 3 — Reduced functional bladder capacity:
Some children have a bladder that is functionally smaller than expected for their age — it triggers a voiding reflex at lower volumes. This is often associated with daytime symptoms (urgency, frequency) and is the non-monosymptomatic pattern. Bladder training exercises and anticholinergic drugs (if overactive bladder is the underlying mechanism) are targeted interventions.
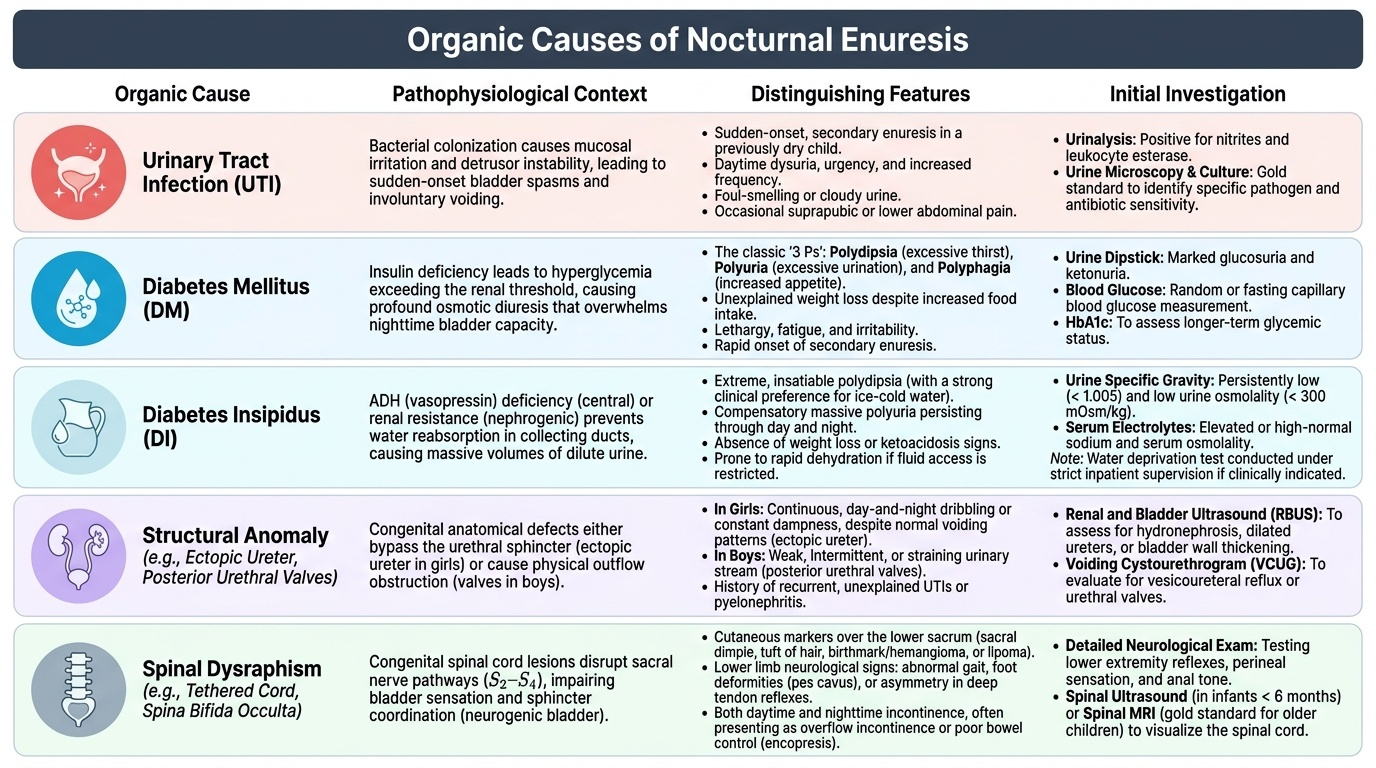
Organic causes account for a minority of enuresis but must be excluded, particularly in secondary enuresis or atypical presentations:
- Urinary tract infection (UTI): dysuria, frequency, fever; urine dipstick shows nitrites and leucocytes.
- Diabetes mellitus: polyuria and polydipsia with weight loss; glucosuria on dipstick.
- Diabetes insipidus: massive polyuria, dilute urine (low specific gravity), hypernatraemia; fails water deprivation test.
- Structural anomaly: posterior urethral valves (boys), ectopic ureter, ureterocele — often present with continuous dribbling or recurrent UTIs.
- Neurological causes: spinal dysraphism (spina bifida occulta) causes neurogenic bladder — look for sacral skin stigmata (tuft of hair, dimple, lipoma), absent anal wink, or lower limb neurological signs.
- Psychological: emotional abuse, post-traumatic stress, school bullying — often secondary enuresis.
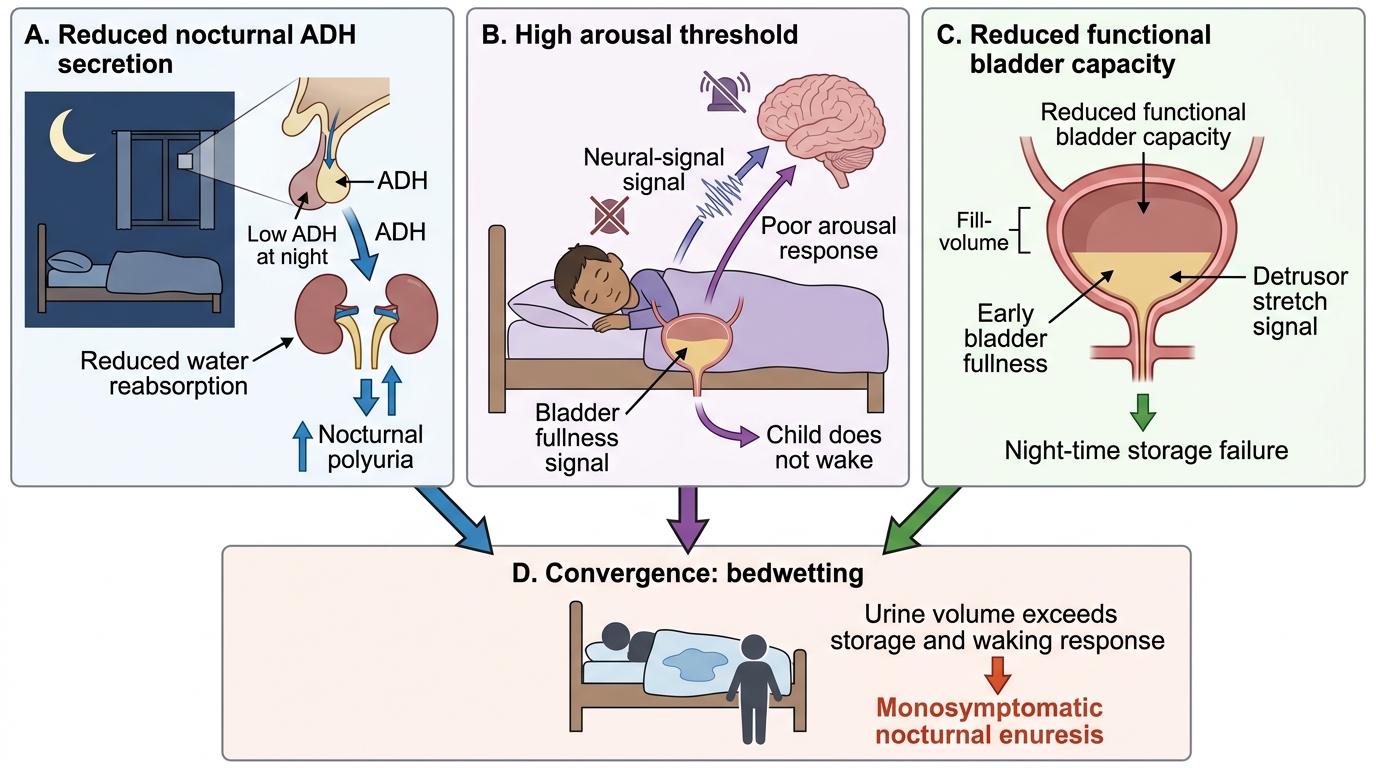
Pathophysiological Pathways in Monosymptomatic Nocturnal Enuresis
SELF-CHECK
A 9-year-old girl has been wetting the bed 3–4 times per week. She was consistently dry at night from age 5 to age 8 years, but relapsed 3 months ago around the time her parents separated. She has no daytime symptoms and no dysuria. Urine dipstick is normal. Which classification best describes her enuresis, and what is the most important next step?
A. Primary monosymptomatic nocturnal enuresis; start desmopressin immediately
B. Secondary nocturnal enuresis; explore psychological precipitants and screen for organic causes (urine culture, blood glucose)
C. Diurnal enuresis; refer for urodynamic studies
D. Normal developmental variation; reassure and review in 6 months
Reveal Answer
Answer: B. Secondary nocturnal enuresis; explore psychological precipitants and screen for organic causes (urine culture, blood glucose)
This is secondary nocturnal enuresis — she was dry for ≥6 months and then relapsed. Secondary enuresis almost always has a precipitant, which in this case is likely the parental separation (psychosocial stress). Even so, organic causes (UTI, diabetes mellitus, diabetes insipidus) must be excluded with urine culture and blood glucose. Primary monosymptomatic nocturnal enuresis would require that she had never been dry. It is not diurnal enuresis (no daytime symptoms). At age 9 it is not a normal developmental variation. The psychological context must be explored and supportive counselling initiated.
Diagnosis and Investigation
The diagnosis of enuresis is clinical, based on a structured history. The goal of evaluation is to classify the enuresis (primary/secondary, nocturnal/diurnal, MNE/non-MNE) and to identify any organic cause that requires targeted treatment. Investigations in MNE are minimal; secondary or atypical enuresis warrants a more extensive work-up. The structured history, physical examination, and a simple urine dipstick will identify the vast majority of organic causes and guide appropriate management. A bladder diary adds precision by quantifying urine volumes and identifying nocturnal polyuria. The clinician should resist ordering renal ultrasound or urodynamic studies routinely — these are reserved for specific indications identified through systematic clinical assessment. Over-investigation exposes the child to unnecessary procedures, generates parental anxiety, and delays evidence-based treatment.
Structured history should document:
- Age of onset and whether the child has ever been dry for >6 months (primary vs secondary).
- Frequency: how many nights per week, how many episodes per night.
- Timing within the night (early vs late night wetting).
- Daytime symptoms: urgency, frequency, daytime incontinence (if present → non-MNE, warrants further evaluation).
- Fluid intake pattern (including evening fluids) and voiding frequency/volumes.
- Associated symptoms: dysuria, haematuria, polyuria, polydipsia, weight loss, abdominal pain.
- Family history of enuresis (strong genetic component).
- Psychosocial history: family stressors, school performance, peer relationships, emotional wellbeing.
- Previous treatments tried and their outcomes.
Physical examination:
- Growth parameters (weight loss suggests diabetes mellitus or other chronic illness).
- Abdomen: palpable bladder (chronic retention), loin tenderness (UTI).
- Genitalia: phimosis, meatal stenosis, labial adhesions, urethral anomalies.
- Spine and lower back: sacral dimple, tuft of hair, lipoma, scoliosis (signs of spinal dysraphism).
- Neurological: lower limb tone, power, reflexes; anal wink reflex (S2–S4 integrity).
A bladder diary (voiding diary) kept for 2–3 days records all voids, volumes, incontinent episodes, and fluid intake — invaluable for identifying nocturnal polyuria (nocturnal urine volume >20% of 24-hour total) or reduced bladder capacity.
Investigations:
- Urine dipstick + culture: mandatory in all children with enuresis to exclude UTI and diabetes mellitus (glycosuria).
- Blood glucose: if polyuria/polydipsia or glycosuria suggests diabetes mellitus.
- Renal ultrasound: if UTI, structural anomaly, or diurnal enuresis is suspected; not routine for MNE.
- Urodynamic studies: only if non-MNE with refractory symptoms or suspected neurogenic bladder.
- MRI lumbosacral spine: if spinal dysraphism is suspected clinically.
- Water deprivation test: to distinguish central DI from nephrogenic DI if DI is suspected.
CLINICAL PEARL
Secondary enuresis is never 'just normal' and must be investigated. A child who was dry for months or years and then starts wetting again has a reason — the three most important are psychosocial stress (ask about family changes, school bullying, abuse), UTI (dipstick always), and new-onset diabetes mellitus (blood glucose, glycosuria). Failing to identify a psychological precipitant — particularly abuse — in a child presenting with secondary enuresis is a serious clinical error. Also remember: the enuresis alarm is more effective than desmopressin for long-term cure (~65–75% success, ~10–15% relapse), while desmopressin works quickly (within days) but relapse after stopping is high (~70%). For a child who needs short-term relief (school camp, overnight trip), desmopressin is ideal; for long-term cure, the alarm is superior.