Page 11 of 17
PE5.4 | Enuresis — SDL Guide (Part 2)
Management of Enuresis
Management of enuresis is stratified by the type and underlying mechanism, with non-pharmacological therapies as the first line for all children with MNE and specific pharmacological therapies reserved for those who have failed non-pharmacological approaches or who require short-term situational control. The paediatrician should always begin with reassurance and general measures before escalating, and should always address any identified organic cause or psychological precipitant before initiating symptomatic treatment. A stepwise approach — general measures first, then enuresis alarm, then pharmacological therapy — ensures that the majority of children with uncomplicated MNE receive effective, evidence-based care without unnecessary drug exposure. Family motivation and commitment to the management plan are as important as the choice of treatment modality.
General measures — applicable to all children:
- Reassurance: explain the condition is common, benign, and has a high spontaneous remission rate; normalise the child's experience; remove blame and punishment.
- Fluid management: adequate fluids during the day; reduce intake in the 2 hours before bedtime; avoid caffeinated drinks (tea, cola) in the evenings.
- Regular voiding: encourage voiding every 2–3 hours during the day and immediately before bed.
- Motivational therapy: a star chart or reward calendar for dry nights (positive reinforcement); effective in younger children as a simple motivational tool.
- Lifting/waking: waking the child to void at a fixed time before the parent goes to bed — a temporising measure that reduces the wet episode frequency but does not treat the underlying problem and does not achieve dryness.
Enuresis alarm (conditioning therapy):
The enuresis alarm (bell-and-pad or wearable alarm) is the most effective long-term treatment for MNE and is the first-line specific therapy. A moisture sensor triggers an alarm when the child begins to wet; this wakes the child (or the parent, who then wakes the child), who then goes to the toilet to complete voiding. Over 12–16 weeks, classical conditioning links the sensation of a full bladder with the arousal response, eventually allowing the child to wake and void before the alarm sounds, and ultimately to sleep through the night dry. Success rate: ~65–75%; relapse: ~10–15% (much lower than desmopressin). The alarm requires parental commitment and a minimum trial of 12–16 weeks before assessing efficacy. It is less suitable for children who share a bedroom (noise disturbance) or in households where parental support is limited.
Pharmacological therapy:
Desmopressin (DDAVP): A synthetic analogue of ADH (vasopressin) that reduces nocturnal urine production by concentrating the urine. It is effective for the nocturnal polyuria subtype of MNE. Onset is rapid — a dry night may occur from the first dose. Dose: oral tablet 0.2–0.4 mg at bedtime (or sublingual melt 120–240 µg). The key safety precaution is fluid restriction: the child must not drink for 1 hour before the dose and must restrict fluids for 8 hours after the dose, to prevent hyponatraemia (water retention from excessive ADH effect). Desmopressin does not cure the underlying condition — relapse after stopping is approximately 70%. It is therefore most useful for situational/short-term control (e.g., school camp, overnight stay with friends) rather than as a curative treatment. If used long-term, structured withdrawal (gradual dose reduction) improves the chance of sustained dryness.
Imipramine: A tricyclic antidepressant that reduces enuresis through a combination of mild anticholinergic effects on the bladder, ADH-like reduction of urine output, and changes in sleep architecture. It was historically the most commonly prescribed drug for enuresis in India but is now third-line due to its risk of cardiac arrhythmia and fatal accidental overdose in children. The therapeutic window is narrow and the drug should be stored safely. It should only be prescribed by a paediatrician with careful monitoring, and is not recommended as a first or second-line treatment.
Organic causes: treat specifically — antibiotics for UTI, insulin for diabetes mellitus, DDAVP or other therapy for diabetes insipidus, surgical referral for structural anomalies or spinal dysraphism.
Secondary enuresis: address the precipitant — psychological support (counselling, family therapy) for stress-related relapse; treat UTI or diabetes if identified; assess for safeguarding concerns if abuse is suspected.
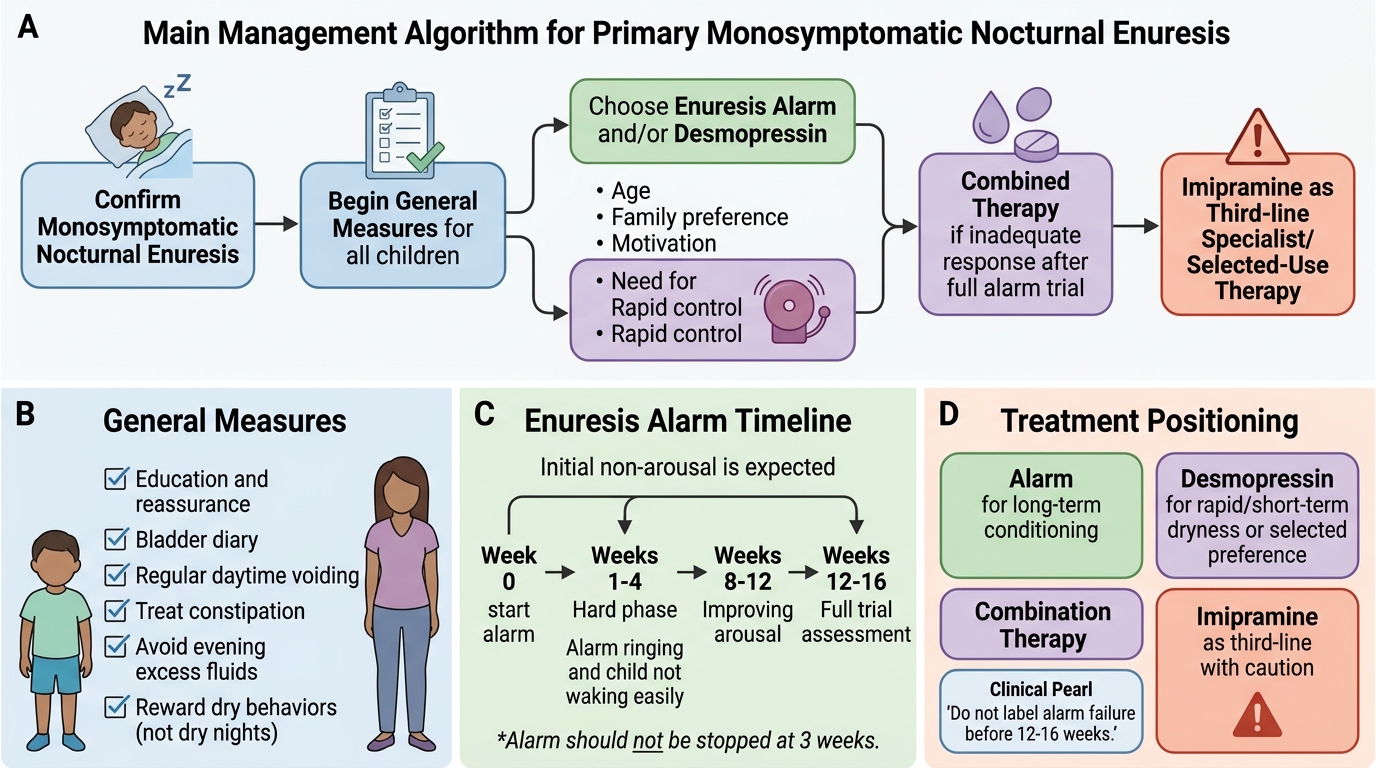
Management Algorithm for Monosymptomatic Nocturnal Enuresis
SELF-CHECK
A 10-year-old boy with primary monosymptomatic nocturnal enuresis is started on the enuresis alarm. His parents return after 3 weeks saying 'the alarm goes off every night but he doesn't wake up — it's not working.' What is the most appropriate advice?
A. Discontinue the alarm and start oral desmopressin instead
B. Continue the alarm for a full 12–16 week trial — initial non-arousal is expected and improvement typically occurs over 2–3 months
C. Switch to imipramine as first-line pharmacotherapy
D. Refer for urodynamic studies as the alarm is contraindicated
Reveal Answer
Answer: B. Continue the alarm for a full 12–16 week trial — initial non-arousal is expected and improvement typically occurs over 2–3 months
The enuresis alarm requires a minimum trial of 12–16 weeks; non-arousal in the first few weeks is common and expected — this is part of the conditioning process. The child's arousal threshold gradually lowers as the conditioning reflex develops. Parents must be warned in advance that the first 2–4 weeks are the hardest. Discontinuing after 3 weeks and labelling it as 'not working' is premature. Imipramine is third-line (not first-line). Urodynamic studies are not indicated for MNE. Desmopressin may be added if the alarm alone is insufficient after a full trial.
Self-Assessment
You have now covered the definition, classification, pathophysiology, diagnosis, and management of enuresis. The key conceptual anchors are the two classification axes (timing and history), the three functional mechanisms of MNE, and the distinction between the enuresis alarm (best for long-term cure) and desmopressin (best for short-term situational control). Secondary enuresis is the most clinically important pattern to identify promptly, as it always has an underlying precipitant that must be found and addressed. Use the checklist below to confirm your readiness for clinical examination questions — each point maps directly to commonly tested examination stems on enuresis. Ensure you can recall both the factual thresholds (ages, doses, relapse rates) and the underlying reasoning, since clinical vignettes test whether you understand why, not just what.
- Enuresis is not diagnosed before age 5 years; affects 15–20% of 5-year-olds, 5% of 10-year-olds.
- Primary: never dry for >6 months; secondary: dry ≥6 months then relapsed → always investigate.
- MNE: nocturnal only, no daytime symptoms, no organic cause — the most common subtype.
- Three mechanisms of MNE: (1) reduced nocturnal ADH → nocturnal polyuria; (2) high arousal threshold; (3) reduced functional bladder capacity.
- Organic causes: UTI, DM, DI, structural anomaly, spinal dysraphism — screen with urine dipstick + culture ± blood glucose.
- Enuresis alarm: most effective long-term (~65–75% success); requires 12–16 week trial.
- Desmopressin: rapid onset; restrict fluids (prevent hyponatraemia); relapse ~70% on stopping; best for situational use.
- Imipramine: third-line only; risk of cardiac arrhythmia and fatal accidental overdose.