Page 2 of 28
PE6.1-3 | Adolescent Development — SDL Guide (Part 2)
Psychological and Social Development in Adolescence
Psychological development during adolescence is as profound as the physical transformation. Three frameworks are especially useful for clinicians encountering adolescents.
Provided image
Piaget's cognitive development theory places adolescence in the formal operational stage (from approximately 12 years onward), characterised by the emergence of abstract reasoning, hypothetical thinking, and the capacity to consider multiple possibilities simultaneously. Before this stage (in Piaget's earlier concrete operational phase), the child's thinking is bounded by tangible, observable realities. Adolescents become capable of understanding probability, considering future consequences, constructing systematic plans, and engaging in scientific reasoning. However, formal operational thinking is not uniformly present at the start of adolescence — it develops progressively, with many young adolescents still relying on concrete-operational strategies in novel domains. This has direct implications for how health information is presented: early adolescents benefit from concrete, example-based explanations; older adolescents can engage with probability-based risk discussions.
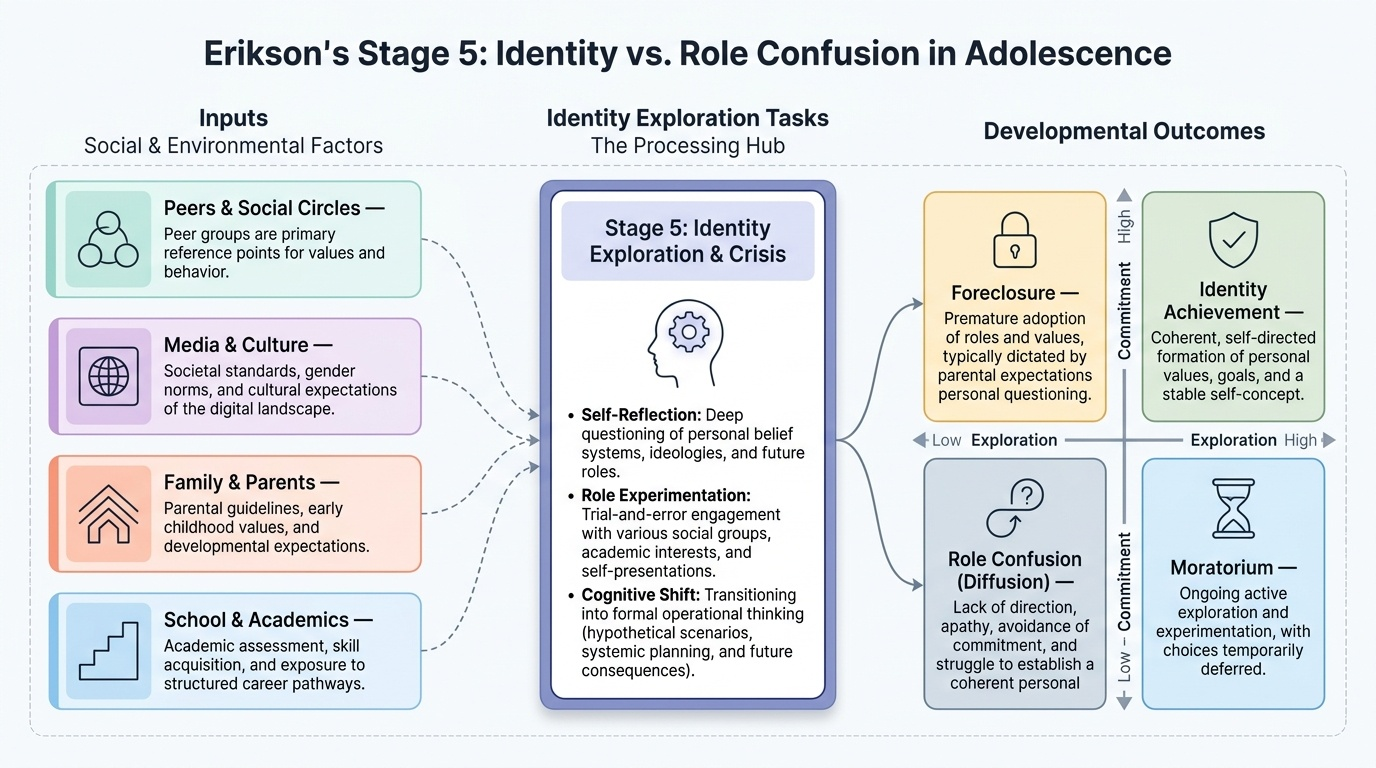
Erikson's psychosocial theory identifies adolescence as the stage of Identity vs. Role Confusion (Stage 5 of 8). The central developmental task is the formation of a coherent personal identity — a stable sense of who one is, what one values, and where one is headed. Successful resolution leads to a strong self-concept (identity achievement); failure to resolve the stage results in role confusion — uncertainty about identity, aimlessness, and social isolation. Between these poles, many adolescents pass through moratorium (active exploration without commitment) or foreclosure (premature commitment without exploration, often following parental prescription). Peer group membership, academic performance, body image, and cultural expectations all feed into identity formation.
Social and emotional development in adolescence is characterised by:
- Peer primacy: the peer group replaces parents as the primary reference group for values, behaviour, and identity, especially in middle adolescence.
- Risk-taking behaviour: experimentation with substances, unsafe sexual practices, and thrill-seeking is driven partly by an imbalance between the maturing limbic system (emotional, reward-seeking) and the still-maturing prefrontal cortex (impulse control, long-term planning), which does not fully mature until the mid-20s.
- Autonomy drive: the push for independence from parental control is developmentally normal and necessary for adult competence, but creates family conflict when misread as oppositional behaviour.
- Body image concerns: especially prominent in girls; the mismatch between the media-projected ideal body and the adolescent's own changing body contributes to eating disorders and low self-esteem.
IMPORTED FROM IMAGE SLOTS:
General Health Problems of Adolescence
The biopsychosocial vulnerability of adolescence creates a distinctive disease burden that differs substantially from both childhood and adulthood. Understanding this spectrum is essential for anticipatory guidance and early intervention.
Nutritional disorders are the leading cause of morbidity among Indian adolescents. Anaemia (predominantly iron-deficiency) affects up to 56% of adolescent girls in India — driven by menstrual blood loss, poor dietary iron intake (predominantly non-haem iron in cereal-based diets), and rapid growth-related iron demand. Adolescent boys are also affected (approximately 30%), though less severely. Undernutrition (thinness, BMI-for-age below −2 SD) remains prevalent in rural India, while overweight and obesity are rising steeply in urban populations due to ultra-processed food consumption and sedentary lifestyles. Vitamin D deficiency and calcium insufficiency during the critical bone-mineralisation window of adolescence contribute to future osteoporosis. Eating disorders — anorexia nervosa and bulimia nervosa — while less prevalent than general under/over-nutrition, carry significant morbidity and mortality and are addressed in the dedicated SDL (PE6.5).
Reproductive and sexual health problems include menstrual disorders (dysmenorrhoea, irregular cycles in the first 2 years after menarche — which is normal), adolescent pregnancy (a major public-health concern; India's adolescent birth rate has declined but remains significant), sexually transmitted infections (STIs), and sexual abuse. The confidential, non-judgmental consultation environment is critical for adolescents to disclose reproductive health concerns, as explored in PE6.4 and PE6.7.
Mental health disorders emerge predominantly during adolescence: approximately 50% of all lifetime mental health disorders have their onset before age 14. Depression, anxiety disorders, attention-deficit/hyperactivity disorder (ADHD), and conduct disorder are the most prevalent. Suicide is the third leading cause of death in the 15–29 age group globally; in India, it is a leading cause of mortality in female adolescents. Self-harm without suicidal intent is also prevalent. These are covered in detail in the PE6.6 SDL.
Substance use — tobacco (bidis, cigarettes, smokeless tobacco), alcohol, inhalants (whitener, petrol), cannabis, and in urban areas, harder substances — begins predominantly in adolescence. Early initiation is strongly predictive of dependence. The HEADSS/HEEADSSS screening tool probes substance use in every adolescent encounter.
Injuries and violence account for a disproportionate share of adolescent mortality: road traffic accidents (RTAs), drowning, burns (particularly in adolescent girls in low-income households), and both witnessing and experiencing violence. Risk-taking behaviour (speed, impaired driving, non-use of helmets) amplifies injury risk.
| Health Problem Category | Key Indian Points |
|---|---|
| Anaemia | 56% girls; iron-deficiency primary; addressed by WIFS |
| Undernutrition/Obesity | Dual burden — rural thinness, urban obesity |
| Menstrual disorders | Dysmenorrhoea common; irregular cycles normal first 2 years |
| Mental health | Depression, anxiety, suicide risk — peak onset in adolescence |
| Substance use | Tobacco/alcohol/inhalants — onset in adolescence predicts dependence |
| RTAs/Injuries | Leading preventable cause of adolescent mortality |
| STIs/Adolescent pregnancy | Confidentiality essential for disclosure |
| Sexual abuse | High prevalence; under-reported; POCSO 2012 applies |
CLINICAL PEARL
Physiological vs. pathological in adolescent girls: Irregular menstrual cycles for up to 2 years after menarche are NORMAL and reflect an immature HPG axis that has not yet established regular ovulatory cycles. Do NOT treat with hormonal therapy for irregular cycles alone in the first 2 years. However, primary dysmenorrhoea (painful periods with no underlying pathology) is common and causes significant school absenteeism — NSAIDs (ibuprofen, mefenamic acid) initiated at the onset of menstruation are highly effective first-line treatment. Also remember: delayed puberty investigations should be initiated if a girl shows no breast development by age 13, or if menarche has not occurred within 3 years of thelarche, or by age 16 in a girl with otherwise normal development.
SELF-CHECK
Which of the following accurately describes the RKSK (Rashtriya Kishor Swasthya Karyakram) programme?
A. A national programme targeting children under 5 years for prevention of malnutrition
B. A national programme launched in 2014 under NHM targeting 10–19-year-olds across six thematic areas including nutrition, sexual and reproductive health, and mental health
C. A programme providing iron supplementation exclusively to adolescent girls in school settings
D. A programme targeting youth aged 15–24 years for vocational training and employment
Reveal Answer
Answer: B. A national programme launched in 2014 under NHM targeting 10–19-year-olds across six thematic areas including nutrition, sexual and reproductive health, and mental health
RKSK (Rashtriya Kishor Swasthya Karyakram) was launched in 2014 by the Ministry of Health and Family Welfare under the National Health Mission (NHM). It targets adolescents aged 10–19 years — both in-school and out-of-school — across six thematic areas: nutrition, sexual and reproductive health, substance misuse, mental health, injuries and violence, and non-communicable diseases. RKSK operationalises adolescent-friendly health services through Adolescent Friendly Health Clinics (AFHCs) at the block and district level. The WIFS (Weekly Iron-Folic Acid Supplementation) programme, which provides IFA to adolescent girls (and boys in high-anaemia districts), is a component of RKSK, not a standalone programme. RKSK does not focus on under-5 children or vocational training.
National Programmes — RKSK, AFHC, WIFS, and HEEADSSS Assessment
RKSK (Rashtriya Kishor Swasthya Karyakram) is India's flagship adolescent health programme, launched in 2014 under the National Health Mission. It covers approximately 253 million adolescents (10–19 years) across six thematic areas: nutrition, sexual and reproductive health, substance misuse, mental health, injuries and violence, and non-communicable diseases. RKSK replaced the earlier ARSH (Adolescent Reproductive and Sexual Health) programme with a broader, more comprehensive mandate.
Adolescent-Friendly Health Clinics (AFHCs) are the delivery mechanism for RKSK. They operate at block/CHC level (and ideally PHC level), providing confidential, non-judgmental outpatient services specifically for adolescents. The AFHC model mandates: (a) a designated space with privacy; (b) trained healthcare providers with adolescent-communication skills; (c) a weekly dedicated session; (d) a defined package of services covering the six thematic areas; and (e) peer-educator outreach linkage.
WIFS (Weekly Iron-Folic Acid Supplementation) is a RKSK sub-component addressing the critical problem of adolescent anaemia. Under WIFS:
- Adolescent girls 10–19 years (both in-school and out-of-school): weekly IFA tablet (100 mg elemental iron + 500 µg folic acid) throughout the year, plus biannual deworming with albendazole 400 mg.
- Adolescent boys in high-anaemia-burden districts: weekly IFA to address male adolescent anaemia.
- In-school WIFS: supervised weekly administration at schools on a designated day.
- Out-of-school WIFS: distributed through ANMs/ASHAs for adolescents not in the school system.
HEEADSSS psychosocial assessment is a structured, evidence-based tool for identifying psychosocial risk in adolescent clinical encounters. The mnemonic covers nine domains:
- H — Home (living situation, family relationships, safety at home)
- E — Education/Employment (school performance, absenteeism, vocational status)
- E — Eating (dietary habits, body image, disordered eating concern)
- A — peer Activity (hobbies, sports, peer group, screen time)
- D — Drugs (tobacco, alcohol, inhalants, cannabis, other substances)
- S — Sexuality (sexual activity, orientation, contraception, STI risk, pregnancy concern)
- S — Suicide/depression (mood, self-harm, suicidal ideation)
- S — Safety (road safety, physical violence at home/school, bullying, abuse)
HEEADSSS is typically introduced with general, less sensitive questions (Home, Education, Activities) before moving to more sensitive domains (Drugs, Sexuality, Suicide). It is NOT a written questionnaire to be handed to the adolescent — it is a structured interview technique. Confidentiality must be established clearly at the outset: the clinician should explain to the adolescent that information shared will remain private UNLESS there is immediate risk of harm to themselves or others. This mirrors the ethical framework discussed in PE6.7.
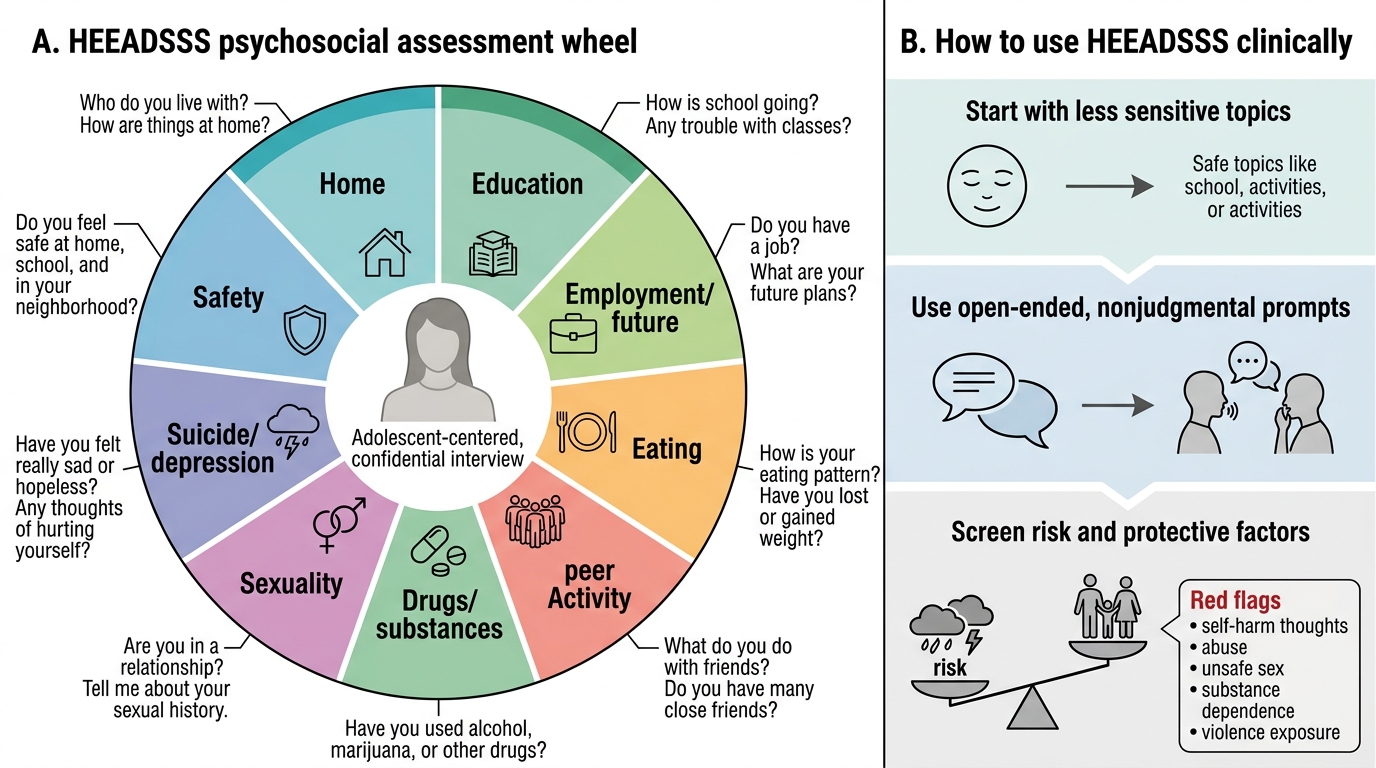
HEEADSSS Psychosocial Assessment Wheel