Page 3 of 28
PE6.1-3 | Adolescent Development — SDL Guide (Part 3)
Self-Assessment — Adolescent Development
Use these questions to consolidate your understanding. Attempt each before checking the answers.
Provided image
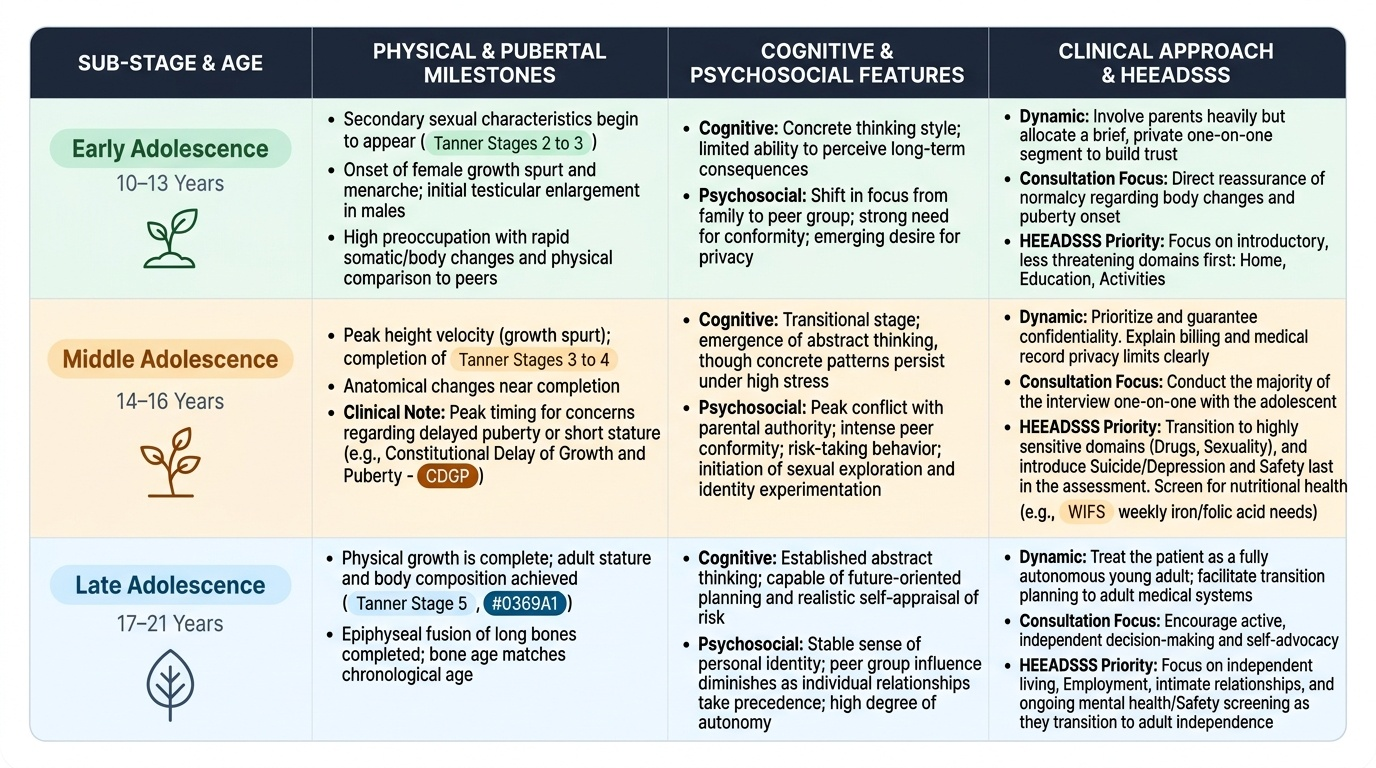
Question 1: A 16-year-old boy presents with concerns about his height — he is shorter than all his classmates. He has Tanner Stage 2 genitalia and Tanner Stage 1 pubic hair, and his bone age on X-ray is consistent with 13 years. His parents both reached their full height in their late teens. What is the MOST likely diagnosis?
Answer: Constitutional delay of growth and puberty (CDGP). The constellation of delayed pubertal onset, delayed bone age, and a family history of late puberty (positive family history) strongly supports CDGP — the most common cause of short stature with delayed puberty in boys. CDGP is a variant of normal. Boys with CDGP will ultimately reach a normal adult height (predicted from mid-parental height), simply on a delayed timeline. Reassurance, nutritional optimisation, and close monitoring are the management; short-course low-dose testosterone is occasionally used for psychosocial distress.
Question 2: Which of the following is a COMPONENT of the WIFS programme?
Answer: Weekly IFA tablet (100 mg elemental iron + 500 µg folic acid) and biannual albendazole 400 mg for adolescent girls 10–19 years, and in high-anaemia districts, for boys as well.
Question 3: During a HEEADSSS assessment of a 15-year-old, which domain is introduced LAST because it is the most sensitive?
Answer: Suicide/depression and Safety are typically the most sensitive domains and are covered later in the assessment, after rapport is established. Drugs and Sexuality are also sensitive. Home and Education are introduced first.
SELF-CHECK
A 12-year-old girl's mother reports her daughter has begun developing breast buds over the past 3 months. On examination you confirm bilateral Tanner Stage 2 breast development. There is no pubic hair, no axillary hair, and she has not had menarche. Her height plots on the 50th centile. What is the appropriate clinical response?
A. Reassure: breast budding (thelarche) as the first sign of puberty at age 12 is completely within the normal range
B. Refer immediately for workup of precocious puberty — breast development before age 14 is abnormal
C. Order bone age, LH, FSH, oestradiol to rule out central precocious puberty before reassuring
D. Start combined oral contraceptive pill to halt premature pubertal progression
Reveal Answer
Answer: A. Reassure: breast budding (thelarche) as the first sign of puberty at age 12 is completely within the normal range
Thelarche (breast budding, Tanner Stage B2) as the first sign of puberty typically occurs between 8 and 13 years in girls. The lower limit of normal is 8 years; thelarche before 8 years requires evaluation for precocious puberty. At age 12, this girl's thelarche is completely within the normal range and requires only reassurance and anticipatory guidance. The normal pubertal sequence should be explained to both the mother and daughter. Precocious puberty is defined as development of secondary sexual characteristics before 8 years in girls (or before 9 years in boys) — not before 14 years as stated in option B. Hormone suppression and contraceptives are never used to 'halt' normal puberty.