Page 15 of 28
PE6.8 | Adolescent Health Checkup — SDL Guide
Learning Objectives
- Perform a comprehensive adolescent health history using the HEEADSSS psychosocial screening tool
- Conduct a structured physical examination including Sex Maturity Rating (Tanner staging), growth assessment using IAP growth charts, and systemic examination including thyroid and breast
- Interpret findings from the adolescent health checkup to identify normal pubertal progress and detect concerning deviations
- Apply ethical principles of confidentiality, chaperoning, and sensitive communication in adolescent health encounters
INSTRUCTIONS
Adolescent health checkup is a unique clinical encounter requiring skills distinct from routine paediatric assessment. Unlike younger children, adolescents carry a heavy burden of psychosocial risk — substance use, mental health issues, unsafe sexual behaviour, and nutritional disorders — that rarely surfaces spontaneously. This module equips you to conduct a systematic, privacy-respecting health checkup that addresses both physical and psychosocial dimensions. Mastering this skill enables early identification of preventable health problems at a pivotal developmental window, and connects to the wider RKSK and AFHS framework under which adolescent services are delivered in India.
References
- Ghai Essential Pediatrics, 9th Ed, Ch 7 (Adolescent Health) (textbook)
- Nelson Textbook of Pediatrics, 21st Ed, Section 6 (Adolescent Medicine) (textbook)
- IAP Guidelines on Adolescent Health, 2022 (guideline)
- National Health Mission — RKSK Programme Guidelines, MoHFW India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-year-old girl is brought by her mother to the outpatient department for a routine check-up. The mother mentions her daughter has been 'moody' and 'not eating properly' for the past few months. On surface observation, the girl appears healthy. However, when you briefly see her alone, she discloses that she has been skipping meals intentionally, feels 'fat' even though her BMI plots at the 35th percentile, and has been receiving hurtful messages online. How would you systematically uncover what is really affecting this adolescent's health, and what structured examination would reveal pubertal status, nutritional state, and other concerns her mother cannot report?
WHY THIS MATTERS
Adolescents (10–19 years) constitute approximately 21% of India's population and are disproportionately affected by under-nutrition, anaemia, mental health disorders, substance use, and reproductive health challenges — yet they are the least likely to seek healthcare spontaneously. A structured health checkup is the only opportunity to detect these hidden problems before they cause lasting harm. The competency PE6.8 requires you to perform this checkup in a supervised setting, incorporating both the HEEADSSS psychosocial screen and a complete physical examination including pubertal staging and growth assessment. Getting this right matters: an adolescent examined cursorily and sent home may have an eating disorder, thyroid mass, or unsafe behaviour that goes unaddressed for years.
RECALL
Before proceeding, recall the following foundational concepts:
- Puberty is driven by the hypothalamic-pituitary-gonadal (HPG) axis: GnRH pulses trigger LH/FSH release, stimulating gonads to produce sex steroids that cause secondary sexual characteristics and the adolescent growth spurt.
- Growth monitoring requires IAP/WHO reference growth charts; for adolescents you plot height-for-age, weight-for-age, and BMI-for-age on sex-specific charts and interpret against percentile bands.
- Normal pubertal timing in Indian girls: thelarche 8–13 yr, menarche 11–14 yr (mean ~12.5 yr); boys: testicular enlargement 9–14 yr, voice change 13–15 yr.
- Confidentiality is both an ethical principle and a legal right for adolescents in India (consistent with Supreme Court judgements on privacy and the MTP/POCSO framework for minors). Establishing trust is pre-requisite to an honest HEEADSSS screen.
Clinical Indication and Relevance of Adolescent Health Checkup
Adolescent health checkup is indicated as a preventive, proactive health service for every person aged 10–19 years, delivered through primary care, school health programmes, and dedicated adolescent clinics under RKSK (Rashtriya Kishor Swasthya Karyakram). Unlike sick-child encounters which are symptom-driven, the adolescent checkup follows a structured health-maintenance framework addressing biological, psychological, and social dimensions simultaneously. This integrated approach is justified by the epidemiological reality: the leading causes of adolescent morbidity and mortality in India — anaemia (56% of girls, 30% of boys nationally), undernutrition, adolescent mental disorders (~15–20% prevalence), substance use initiation, and reproductive health risks — are largely silent on routine physical examination alone.
The WHO defines adolescence as 10–19 years, subdivided into early (10–13), middle (14–16), and late (17–19) phases. Each sub-phase has distinct developmental tasks and vulnerabilities. Early adolescence is dominated by pubertal change and identity formation; middle adolescence by peer influence, risk-taking behaviour, and the highest vulnerability to substance initiation; late adolescence by vocational identity, intimate relationships, and consolidation of adult health behaviour. Understanding this phasing directs which HEEADSSS domains you probe most intensively at each visit.
The checkup serves multiple functions:
• Screening — detecting anaemia, malnutrition, pubertal disorders, hypertension, thyroid disease, mental health problems
• Anticipatory guidance — nutrition, safe sex, substance avoidance, road safety
• Immunisation update — Td booster, HPV (girls), school boosters per NIS
• Referral gateway — to AFHS specialised services or tertiary care for complex problems
IMPORTANT_NOTE: Perform this checkup in a private room. Spend a few minutes with the adolescent alone — without the parent/guardian — to allow honest disclosure, particularly for psychosocial concerns.
HEEADSSS Framework for Adolescent Assessment
Anatomy and Governing Principles: Pubertal Development and Assessment
The cornerstone of the physical examination of an adolescent is Sex Maturity Rating (SMR), commonly called Tanner staging, which provides a standardised, observer-independent description of pubertal progress. Tanner published the criteria in 1962 based on longitudinal observations on British schoolchildren; they have since been validated across multiple populations, including Indian adolescents, with minor timing differences that are addressed in the IAP normative dataset. The fundamental value of SMR is that it decouples pubertal assessment from chronological age — two 13-year-olds may be at completely different pubertal stages, and using age alone would either falsely reassure or falsely alarm. SMR instead stages each individual's own developmental trajectory by observing the actual physical changes present at examination. This makes it an objective, reproducible, and clinically meaningful tool that guides counselling, investigation decisions, and referrals. Understanding the staging criteria in detail is therefore essential to clinical practice in adolescent medicine.
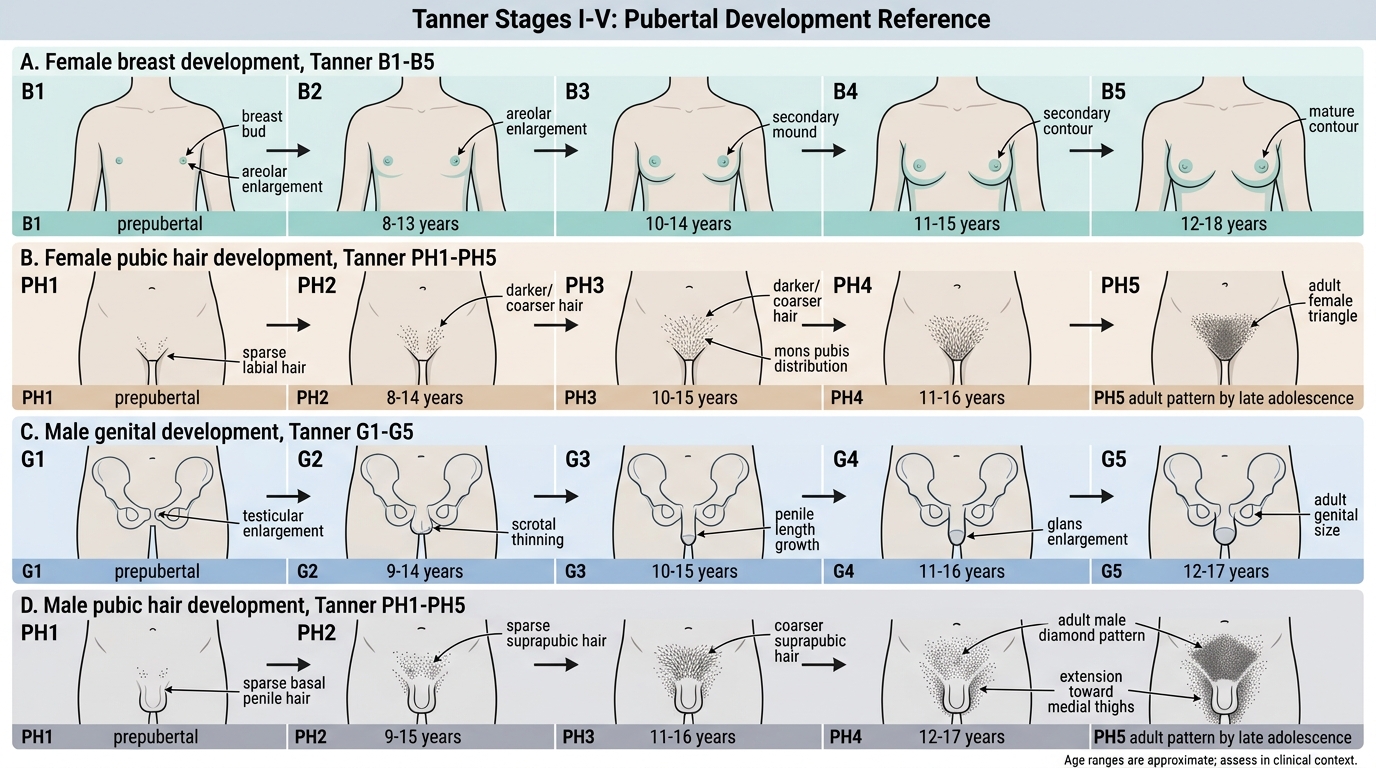
For girls, two separate SMR scales are used:
1. Breast development (B1–B5): B1 = prepubertal (no glandular tissue); B2 = breast budding, small raised area around areola (thelarche, first sign of puberty in most girls); B3 = further enlargement; B4 = secondary mound of areola over breast; B5 = mature adult contour, areola recedes to breast plane.
2. Pubic hair (PH1–PH5): PH1 = no hair; PH2 = sparse, slightly pigmented downy hair along labia; PH3 = darker, coarser, curlier, spread over pubic symphysis; PH4 = adult type but limited distribution; PH5 = adult-pattern spread to medial thighs.
For boys, two separate SMR scales are used:
1. Genital development (G1–G5): G1 = prepubertal; G2 = testicular enlargement >4 mL (by Prader orchidometer), scrotal skin reddening/thinning (first sign of puberty in boys); G3 = penile lengthening + further testicular growth; G4 = further enlargement, scrotal darkening; G5 = adult size and appearance.
2. Pubic hair (PH1–PH5): same criteria as girls.
Indian normative data (IAP) suggests thelarche typically begins at Tanner B2 around 10–12 years (slightly earlier than the original Tanner UK data), and menarche usually occurs at Tanner B3–B4 (mean age ~12.4–12.8 years). For boys, testicular volume ≥4 mL (G2 transition) typically occurs at 10–12 years.
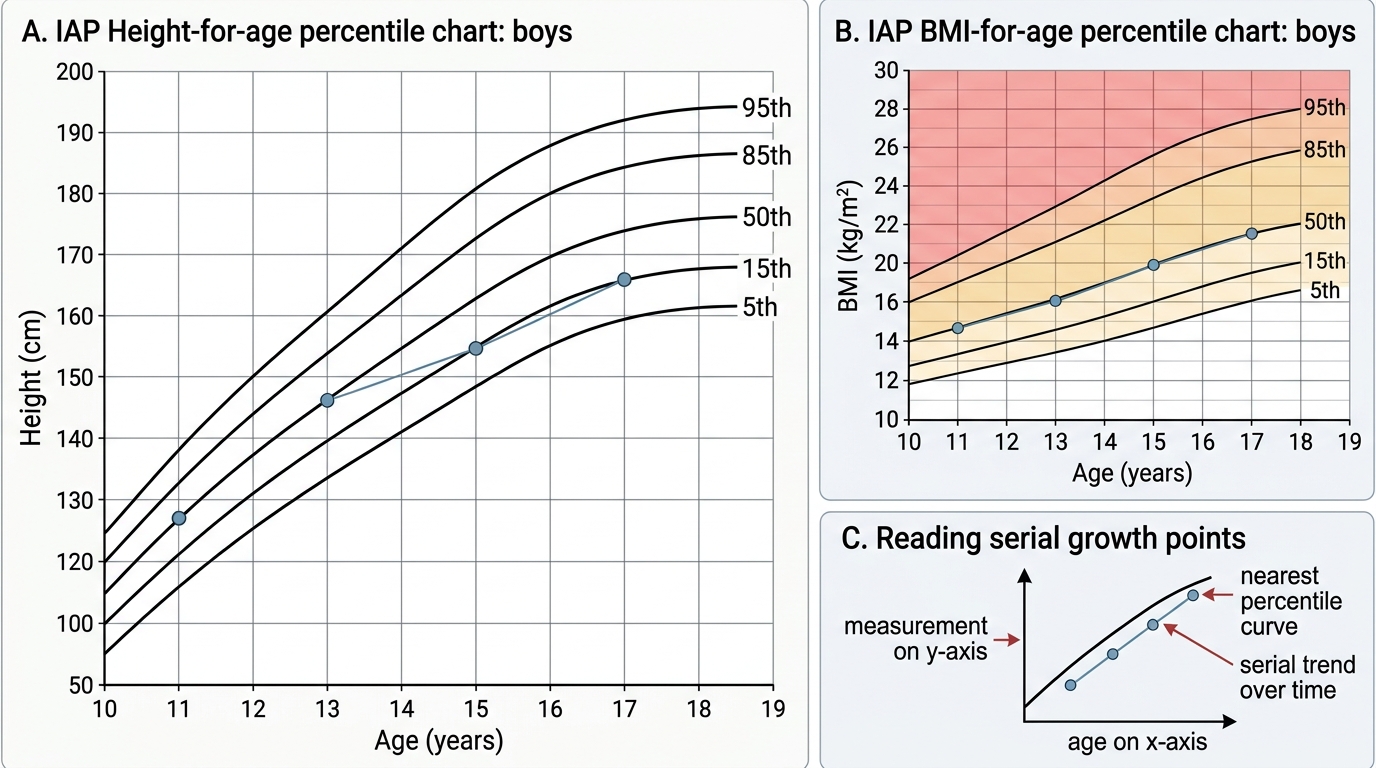
The IAP growth chart uses sex-specific centile curves (3rd, 10th, 25th, 50th, 75th, 90th, 97th percentiles) for height-for-age, weight-for-age, and BMI-for-age. In adolescence, BMI-for-age is preferred over absolute BMI because normal adiposity changes rapidly with age and pubertal stage.
IMPORTANT: Precocious puberty is defined as onset of secondary sexual characteristics before age 8 in girls or age 9 in boys. Delayed puberty is absence of pubertal onset by age 13 in girls (no breast bud) or age 14 in boys (testicular volume <4 mL). Both require investigation.
Tanner Staging Reference for Adolescents
Procedure: Structured Adolescent Health Checkup Technique
A comprehensive adolescent health checkup proceeds in a defined sequence: setting the environment, psychosocial history (HEEADSSS), general physical assessment, growth measurement, pubertal staging, and systemic examination. Each step builds on the previous, and the clinician must maintain a non-judgmental, empathic communication style throughout.
Step 1 — Environment and Rapport:
Begin by welcoming the adolescent and parent/guardian together, explaining the purpose of the visit. Then — and this is non-negotiable — ask the parent to wait outside briefly while you speak with the adolescent alone. Explain the principle of confidentiality: information shared will not be disclosed without consent, except where safety is at risk. This brief private time is when honest psychosocial disclosure occurs.
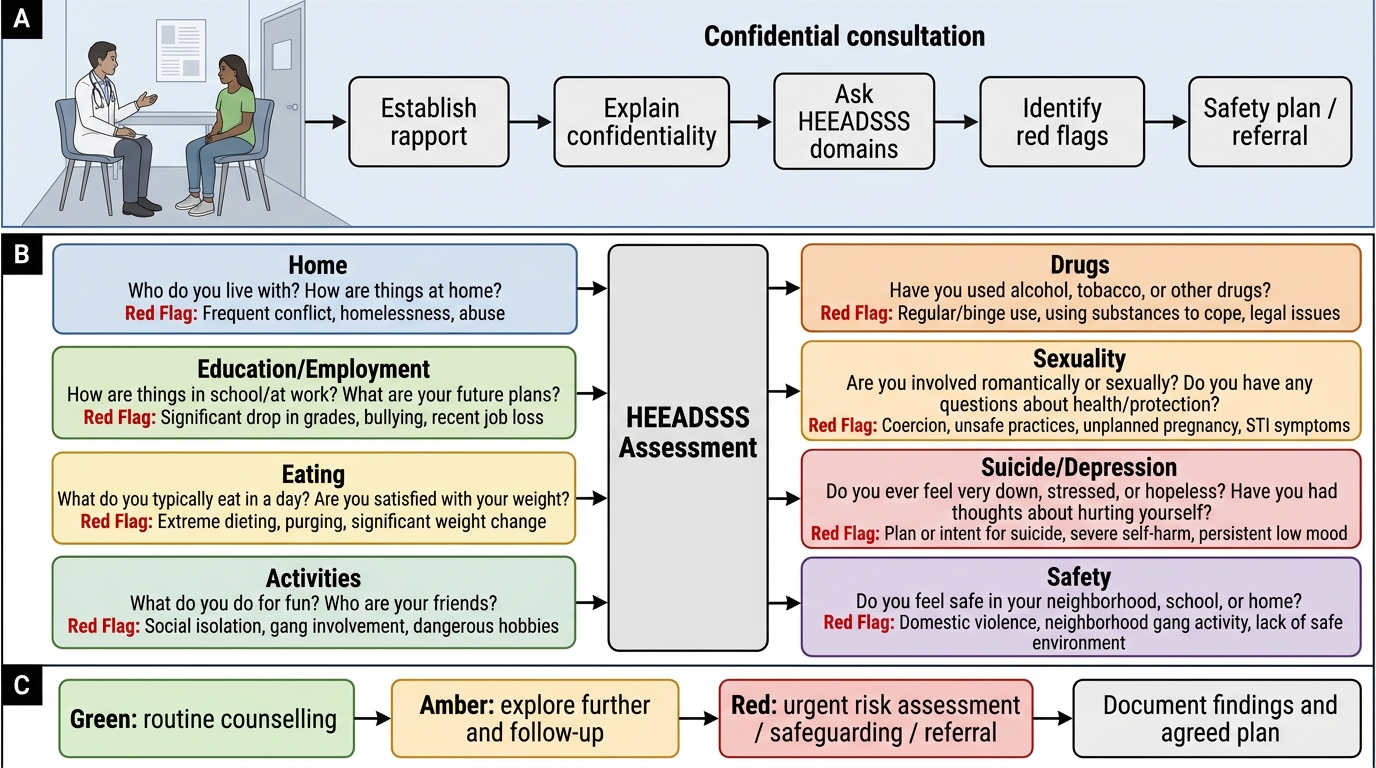
Step 2 — HEEADSSS Psychosocial Screen:
HEEADSSS is a structured psychosocial screening tool validated for adolescent health encounters. Each letter represents a domain:
• H — Home: Who lives with you? Family relationships, recent changes, safety at home
• E — Education/Employment: School/college performance, attendance, goals, bullying
• E — Eating: Dietary habits, body image, weight concerns, skipped meals
• A — Activities: Exercise, hobbies, peer group, screen time
• D — Drugs: Tobacco, alcohol, cannabis, other substances (self and peers)
• S — Sexuality: Pubertal concerns, romantic relationships, sexual activity, contraception, STIs
• S — Suicide/Self-harm: Mood, hopelessness, self-harm, suicidal ideation (use PHQ-A or direct questions)
• S — Safety: Road safety, physical/sexual abuse, online safety, violence
Move from less sensitive to more sensitive domains to build trust. Use open-ended, non-judgmental questions. Red flags — abuse disclosure, suicidal ideation, active substance use, unsafe sexual behaviour — must trigger immediate action within the limits of confidentiality.
Step 3 — Growth Measurements:
Measure height (stadiometer, shoes removed, Frankfurt plane), weight (calibrated digital scale, light clothing), and calculate BMI = weight(kg)/height(m)². Plot all three on sex-specific IAP growth charts against chronological age and read percentiles. Flags:
• Height velocity: < 5 cm/year after age 10 may indicate growth disorder
• BMI ≥ 85th percentile = overweight; ≥ 95th = obese
• BMI < 5th percentile combined with food-restriction history = at risk for eating disorder
Step 4 — General Physical Examination:
Assess vital signs (BP with appropriate cuff size — adolescent cuff), anaemia (conjunctival/palmar pallor), jaundice, lymphadenopathy. Calculate mid-arm circumference if nutritional assessment warranted.
Step 5 — Pubertal Staging (SMR):
Explain procedure sensitively and obtain verbal consent. Chaperone (same sex or as requested) is mandatory. For girls: assess breast stage (inspection and gentle palpation for nodularity) + pubic hair stage. For boys: genital stage (inspection; testicular volume by Prader orchidometer or measurement) + pubic hair stage. Record as, e.g., 'Tanner B3, PH3' or 'Tanner G3, PH3'.
Step 6 — Systemic Examination including Thyroid and Breast:
Thyroid: inspect for goitre (ask adolescent to swallow water, observe neck); palpate thyroid isthmus and lobes, assess texture, tenderness, nodules, bruit. Thyroid disorders — autoimmune thyroiditis, simple goitre, Graves' disease — are not uncommon in adolescent girls.
Breast examination (in girls): inspect for symmetry, skin changes, nipple discharge; gently palpate all four quadrants and axillary tail. Differentiate normal thelarche nodularity from fibroadenoma (discrete, mobile mass, common in adolescents).
Cardiovascular: look for signs of iron-deficiency anaemia (pallor, tachycardia, haemic murmur) — highly prevalent in adolescent girls.
Abdomen: hepatosplenomegaly, tenderness.
Skin: acne grading (useful marker of androgen activity and counselling needs).
| Examination Component | Technique | Key Finding to Note |
|---|---|---|
| Blood pressure | Appropriate cuff; auscultatory; seated | Hypertension ≥130/80 in adolescents needs repeat and evaluation |
| Thyroid | Inspect + palpate; swallow test | Goitre size (WHO grade 0/1/2), nodule, bruit |
| Breast | Inspect + palpate all quadrants | Tanner stage, fibroadenoma, discharge |
| Pubertal staging | SMR criteria; chaperone | Stage and concordance of breast/pubic hair |
| BMI-for-age | Plotted on IAP chart | Percentile; overweight/obese/thin |
IAP Growth Chart Interpretation in Adolescent Boys
SELF-CHECK
A 13-year-old girl has breast budding with small raised areola and sparse, slightly pigmented pubic hair along the labia majora. What is her correct Tanner (SMR) staging?
A. Breast B1, Pubic Hair PH1
B. Breast B2, Pubic Hair PH2
C. Breast B3, Pubic Hair PH3
D. Breast B2, Pubic Hair PH3
Reveal Answer
Answer: B. Breast B2, Pubic Hair PH2
Breast budding with a small raised area around the areola is the classic description of Tanner breast stage B2 (thelarche), which is the first sign of puberty in most girls. Sparse, slightly pigmented downy hair along the labia is Tanner pubic hair stage PH2. Both stages are B2/PH2, corresponding to early puberty onset. B3 involves further breast enlargement beyond the simple bud; PH3 involves darker, coarser hair spread over the mons pubis.