Page 16 of 28
PE6.8 | Adolescent Health Checkup — SDL Guide (Part 2)
Interpretation of Findings in Adolescent Health Checkup
Interpretation of the adolescent health checkup requires a deliberate synthesis step: each set of findings — pubertal staging, growth chart data, thyroid and breast examination, and HEEADSSS responses — must be compared against age- and sex-specific norms, and then integrated into a holistic clinical picture. Isolated findings are rarely sufficient; a BMI at the 88th percentile means very different things in a constitutionally large, active, Tanner-stage-5 adolescent versus a sedentary, anxious 11-year-old. The four key interpretive questions to answer at the end of every adolescent checkup are: (1) Is pubertal progress appropriate for age and following a normal sequence? (2) Is growth tracking as expected on the IAP centile curves? (3) Are there physical signs of systemic disease (thyroid, anaemia, hypertension)? (4) Have any HEEADSSS domains flagged a psychosocial or safety concern requiring action?
Provided image
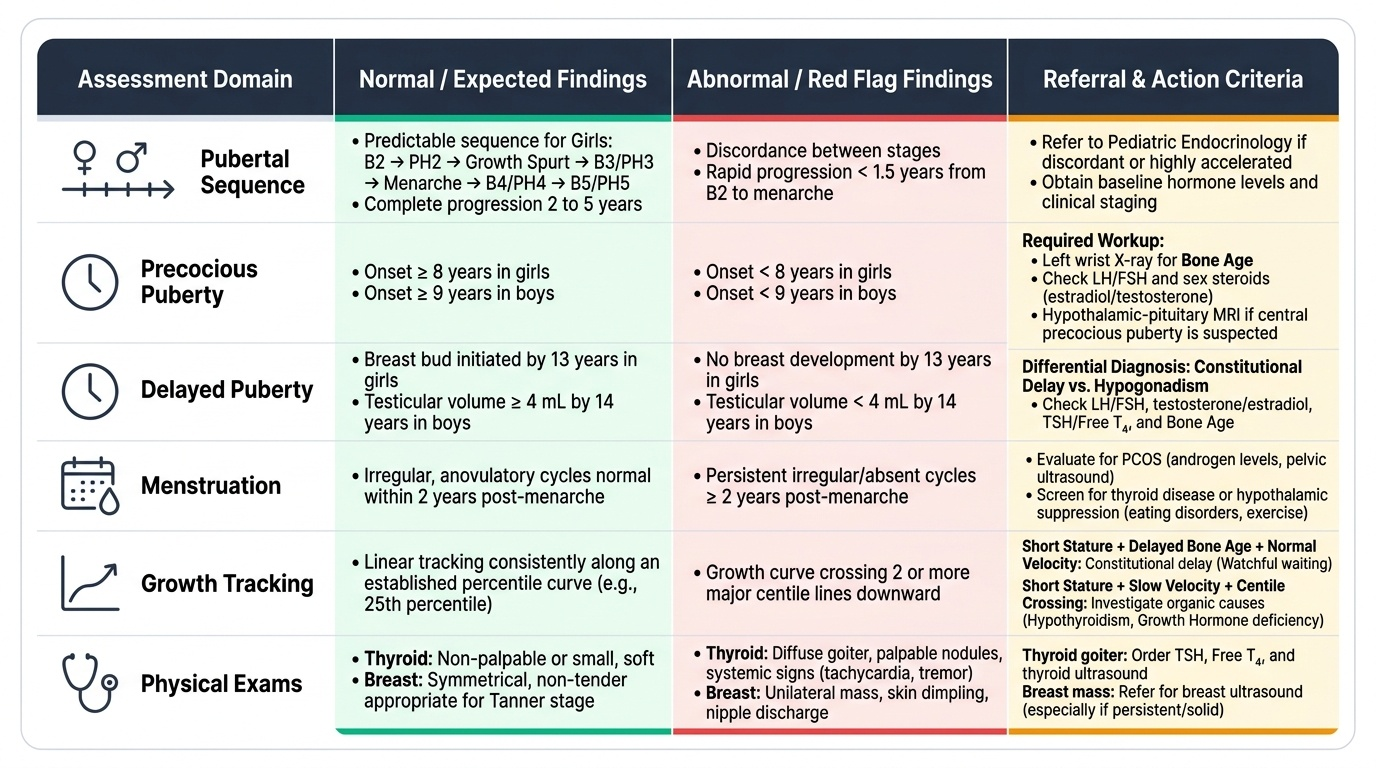
Interpreting pubertal staging:
Normal puberty has a predictable sequence (in girls: B2 → PH2 → growth spurt → PH3–B3 → menarche → B4–PH4 → B5–PH5) completed over 2–5 years. Discordance between stages (e.g., advanced pubic hair without breast development), very rapid progression (<1.5 years from B2 to menarche), or puberty outside the normal age range requires evaluation.
- Precocious puberty (girls <8 yr, boys <9 yr): investigate with bone age (left wrist X-ray), LH/FSH, sex steroids, and hypothalamic-pituitary imaging if indicated.
- Delayed puberty (girls no breast bud by 13 yr, boys testicular volume <4 mL by 14 yr): evaluate constitutional delay vs hypogonadism; check LH/FSH, testosterone/oestradiol, thyroid function, bone age.
- Menstrual irregularity in a girl within 2 years of menarche is physiologically normal (anovulatory cycles common). Beyond 2 years, irregular cycles warrant evaluation for PCOS, thyroid disease, or hypothalamic suppression (intense exercise, disordered eating).
Interpreting growth:
• Serial plotting is more informative than a single measurement. A child tracking the 25th percentile is normal; one who has crossed two major centile lines downward needs investigation.
• Short stature plus delayed bone age + normal growth velocity = constitutional delay (commonest, watchful waiting).
• Short stature + slow velocity + abnormal centile crossing = consider organic cause (hypothyroidism, GH deficiency, chronic illness).
• Obesity (BMI ≥95th percentile): screen for hypertension, dyslipidaemia, insulin resistance, and metabolic syndrome. Lifestyle counselling and family-based intervention first line.
Interpreting thyroid findings:
• Simple goitre (smooth, diffuse, non-tender, euthyroid): common in iodine-sufficient areas due to physiological demand during adolescence; check TSH and urinary iodine.
• Tender goitre with recent viral illness: consider Hashimoto thyroiditis (auto-antibodies positive, TSH elevated, T4 low).
• Palpable nodule: ultrasound neck ± FNAC; thyroid cancer, though rare, does occur in adolescents.
HEEADSSS red-flag responses requiring action:
• Suicidal ideation with plan/intent → immediate risk assessment and referral to mental health
• Active self-harm → document, refer, safety plan
• Disclosure of abuse (sexual, physical, emotional) → mandatory reporting per POCSO Act 2012 if victim <18 years
• Unsafe sexual activity → STI risk counselling, contraceptive guidance, refer to AFHS
• Active substance use → brief intervention, refer
CLINICAL PEARL
Clinical Pearl — The Confidentiality Caveat in Adolescent Health:
The promise of confidentiality to an adolescent has one critical exception: safety override. If an adolescent discloses that they are at risk of serious harm to themselves (suicidal plan with intent) or serious harm to others, or is the victim of ongoing abuse, you are both ethically obliged and legally required (POCSO Act 2012 for victims <18 yr) to involve appropriate adults or authorities — even if this breaks confidentiality. Always pre-disclose this limitation at the start: 'What we discuss is between us, unless I'm worried about your safety or someone else's — in that case I'll need to involve others, and I'll tell you first.' This framing maintains trust while ensuring safety. Never agree to unconditional confidentiality.
SELF-CHECK
During a HEEADSSS screen, a 15-year-old boy discloses that three of his friends use cannabis regularly but he does not. Which is the most appropriate next step?
A. Reassure him that this is normal for his age group and move on
B. Inform his parents immediately about his social circle
C. Acknowledge his non-use positively, provide brief education about risks of initiation, and discuss peer-pressure coping strategies
D. Refer him to a substance abuse counsellor for formal evaluation
Reveal Answer
Answer: C. Acknowledge his non-use positively, provide brief education about risks of initiation, and discuss peer-pressure coping strategies
The HEEADSSS tool identifies risk contexts — not just individual behaviour. This adolescent is in a peer environment that is a risk factor for initiation. The appropriate response is to affirm his current non-use (reinforces protective behaviour), provide anticipatory guidance about cannabis risks (brain development, academic performance, risk of progression), and discuss concrete peer-pressure coping strategies. Informing parents breaks confidentiality for a disclosure that is not an immediate safety risk. Formal substance abuse referral is not indicated when the adolescent himself is not using. Normalising drug use by friends without guidance would be a missed opportunity.
Applied and Supervised Practice: Special Considerations
In supervised clinical practice, several practical and ethical dimensions of the adolescent health checkup require specific attention beyond technical competence. These apply directly when you encounter adolescent patients in outpatient or school health settings.
Chaperoning:
A chaperone — a trained healthcare worker of the same sex as the adolescent (or as requested) — must be present during the physical examination, particularly for breast and pubertal staging examinations. The chaperone's role is to protect both patient and clinician and to assist with examination logistics. The chaperone should be introduced and their role explained to the adolescent. Never proceed with intimate examination without a chaperone.
Communication skills specific to adolescents:
Avoid leading questions (e.g., 'You don't drink, do you?') and closed questions during HEEADSSS. Use open-ended, normalising statements ('Many teenagers your age try cigarettes — have you ever?') to reduce shame-based non-disclosure. Maintain a neutral, non-reactive tone when sensitive disclosures occur — any visible shock or judgment will shut down further communication.
Documentation:
Record Tanner stages explicitly (e.g., 'B3, PH3' for girls; 'G3, PH3' for boys). Plot growth measurements on the chart and record the percentile. Note each HEEADSSS domain assessed and whether any red flags were identified. If no red flags: 'HEEADSSS screen — no concerns disclosed in any domain.' If red flags present: document disclosure, action taken, and referral made.
The RKSK linkage:
Under India's Rashtriya Kishor Swasthya Karyakram (RKSK), adolescent health checkups are delivered through RKSK peer-educators, Sub-Centres, PHCs, and dedicated Adolescent Friendly Health Clinics (AFHC). As a physician, you should know the referral pathway: complex problems identified at primary care level (eating disorders, pubertal disorders, mental health, reproductive health) are referred to AFHC or district hospitals with adolescent clinics. Completing the checkup without knowing where to refer an identified problem is incomplete care.
Follow-up scheduling:
Annual well-adolescent checkups are recommended. Adolescents with identified concerns (overweight, menstrual irregularity, elevated BP) need interval follow-up. Immunisations should be updated at each visit per the National Immunization Schedule — Td at 10 and 16 years; HPV vaccine (girls, 9–14 years, 2-dose schedule) where available.
Self-Assessment
The following self-assessment questions are designed to test your readiness for supervised clinical practice with adolescent patients. Work through each question independently before checking your answers against the module content. A clinician who can answer all seven questions confidently has the conceptual framework to perform a competent initial adolescent health checkup under faculty supervision. Pay particular attention to questions 4 and 5, which address the two most commonly examined topics in assessments: pubertal delay evaluation and the limits of confidentiality. These are also the areas where students most frequently lose marks in OSCE stations. If you find yourself uncertain on any domain, return to the relevant section and review the HEEADSSS framework diagram and Tanner staging panels before your next clinic session.
- Name all eight domains of the HEEADSSS tool and give one example question for each.
- Describe the Tanner stages B1–B5 (breast) and distinguish B2 from B3 clinically.
- On an IAP growth chart, a 13-year-old girl plots at the 90th percentile for BMI. What does this signify, and what is your next step?
- A 14-year-old girl has had breast budding for 3 years but no menarche. What term describes this? What is your evaluation plan?
- What is the 'safety override' exception to adolescent confidentiality, and under which Act is reporting mandatory for sexual abuse of a minor?
- In a thyroid examination of an adolescent, what findings would prompt you to order an ultrasound?
- During HEEADSSS, the adolescent discloses suicidal ideation without a specific plan. What is your immediate management?