Page 21 of 28
PE6.11 | Adolescent Non Communicable Disease Risk — SDL Guide
Learning Objectives
- Enumerate the importance of obesity and other non-communicable disease (NCD) risks in adolescents
- Describe the epidemiology and rising prevalence of NCD risk factors among Indian adolescents
- Explain the biological and social mechanisms by which adolescent lifestyle factors drive adult NCD burden
- Apply a structured approach to NCD risk screening and lifestyle counselling at the primary care level
INSTRUCTIONS
Non-communicable diseases — diabetes, hypertension, cardiovascular disease, chronic respiratory disease, and cancer — account for approximately 60% of all deaths in India. What is not widely appreciated is that the risk factors for these diseases are largely established during adolescence. An obese 15-year-old has a dramatically higher lifetime risk of type 2 diabetes, hypertension, and cardiovascular disease than their lean peer. A tobacco user who started at age 14 carries a risk profile entirely different from one who began at 25. Understanding adolescent NCD risk is therefore not paediatric trivia — it is the foundation of preventive medicine for the entire adult lifespan. This module addresses the competency requirement to enumerate the importance of obesity and other NCDs in adolescents, with direct application to clinical screening in the AFHC setting.
References
- Ghai Essential Pediatrics, 9th Ed, Ch 7 (Adolescent Health) (textbook)
- Nelson Textbook of Pediatrics, 21st Ed, Section 6 (Adolescent Medicine) (textbook)
- IAP Guidelines on Childhood Obesity, 2015 (guideline)
- WHO Global Action Plan for the Prevention and Control of NCDs 2013–2030 (guideline)
- ICMR-INDIAB Study, India Diabetic Report 2023 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old boy is brought to the adolescent clinic by his father because 'he is too fat and lazy'. His BMI plots at the 96th percentile on the IAP chart. His blood pressure measured today is 138/86 mmHg. He drinks two glasses of cola daily, eats fast food four times a week, and spends 7–8 hours daily on his phone. He has a family history of type 2 diabetes (both parents) and has visible dark, velvety skin patches on his neck. His father asks you: 'Is this just a phase, or is something wrong?' How would you explain the NCD risks embedded in this boy's current health picture, and what does his adolescent trajectory predict for his adult health?
WHY THIS MATTERS
Non-communicable diseases now account for approximately 60–65% of all deaths in India, with cardiovascular disease, diabetes, chronic respiratory disease, and cancer as the leading causes. The Global Burden of Disease framework and India's own National NCD Monitoring Framework both identify that the behavioural and metabolic risk factors for these diseases — unhealthy diet, physical inactivity, tobacco use, alcohol, and obesity — are predominantly established during adolescence, not in adulthood. This means that preventing adult NCDs requires intervening during the adolescent window. As a physician, you will identify the 16-year-old who already has hypertension and pre-diabetes years — potentially decades — before his first cardiac event. That identification opportunity is irreplaceable. Competency PE6.11 requires you to enumerate why adolescent NCD risk matters — not just list the conditions, but understand their significance as a public health priority.
RECALL
Before proceeding, recall the following:
- BMI-for-age is the correct adiposity measure in adolescents — plotted on sex-specific IAP growth charts. BMI ≥85th percentile = overweight; ≥95th percentile = obese.
- Metabolic syndrome is a cluster of cardiovascular risk factors: central obesity, elevated blood pressure, dyslipidaemia, and impaired fasting glucose. Each component amplifies the others.
- Insulin resistance — reduced cellular response to insulin — is the central pathophysiology linking obesity to type 2 diabetes, hypertension, and dyslipidaemia. Acanthosis nigricans (dark, velvety skin at neck/axilla) is a visible clinical marker.
- The four shared modifiable NCD risk factors per WHO: unhealthy diet, physical inactivity, tobacco use, and harmful alcohol use. These are modifiable — and adolescence is the optimal window for modification.
Orientation: Why NCD Risk Begins in Adolescence
Non-communicable diseases (NCDs) are chronic conditions not transmitted by infection — primarily cardiovascular diseases (coronary artery disease, stroke), type 2 diabetes mellitus, chronic obstructive pulmonary disease, cancers, and mental health disorders. The conventional framing places NCDs as diseases of adulthood, but this framing is fundamentally misleading for clinical and public health purposes. The biological processes underpinning adult NCDs — arterial endothelial damage from dyslipidaemia and hypertension, pancreatic beta-cell exhaustion from chronic insulin resistance, pulmonary parenchymal damage from tobacco smoke — begin not in the fifth or sixth decade, but in adolescence, or even earlier with the rise of childhood obesity.
The concept of early origins of disease (the Barker hypothesis, extended by the Developmental Origins of Health and Disease framework) establishes that metabolic programming set in the first two decades of life — including adolescence — has profound and lasting effects on adult disease risk. A 15-year-old with BMI at the 96th percentile who has had central obesity since age 10 may already have measurable endothelial dysfunction, elevated fasting insulin, and early dyslipidaemia — the invisible precursors of a myocardial infarction at age 45. Equally, a 14-year-old who initiates tobacco use has already started the 20–30 year accumulation of carcinogen exposure that manifests as lung cancer in their 40s.
Adolescence is therefore not merely a period of risk-factor acquisition — it is the critical window during which interventions can interrupt the causal pathway from risk to disease with maximum impact, precisely because the disease has not yet caused irreversible damage. This is the clinical and public health importance of adolescent NCD risk.
In India, this urgency is compounded by the double burden of malnutrition: India simultaneously faces undernutrition (anaemia, stunting, wasting — well-documented) AND rapidly rising overweight/obesity, particularly in urban adolescents. A healthcare system that focuses only on undernutrition will miss the emerging NCD epidemic embedded in the same age group.
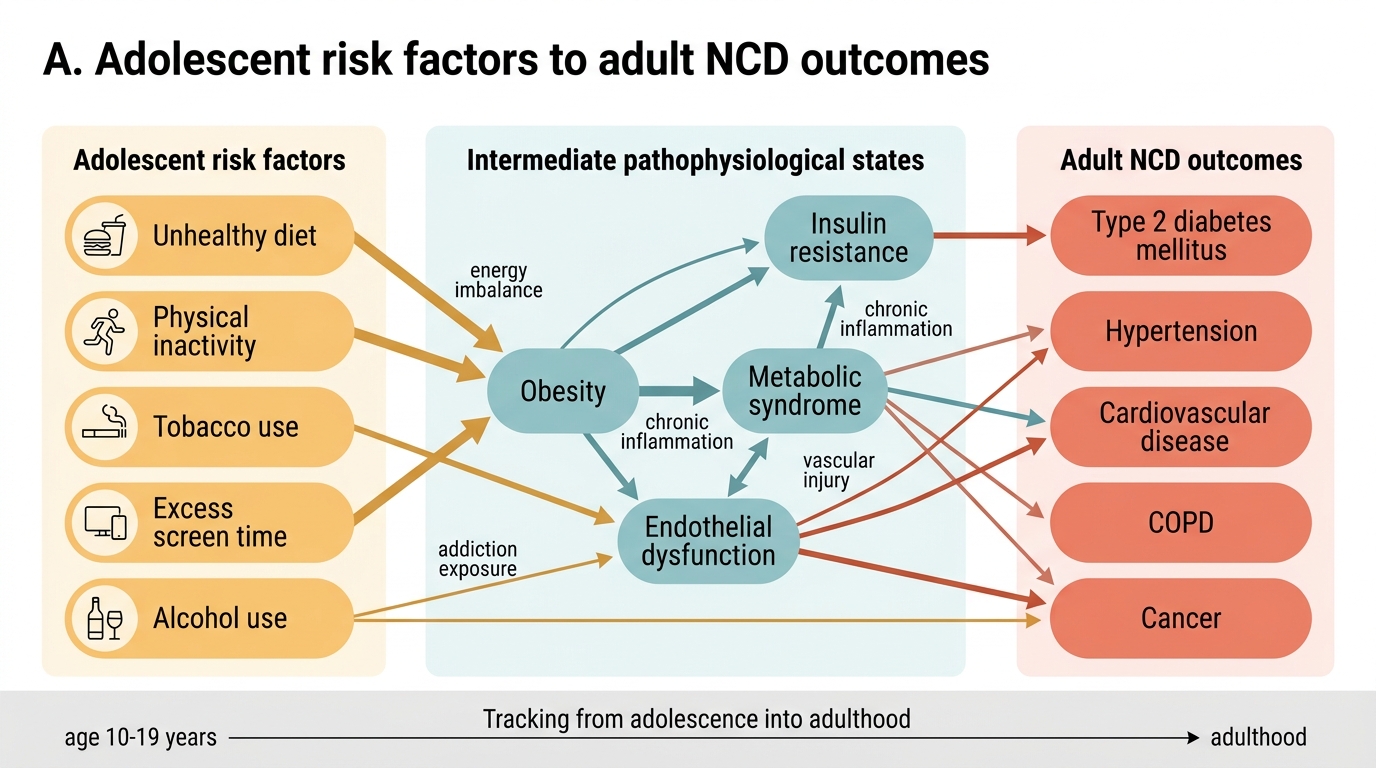
Adolescent Risk Factors and Adult NCD Pathways
Magnitude of NCD Risk in Indian Adolescents
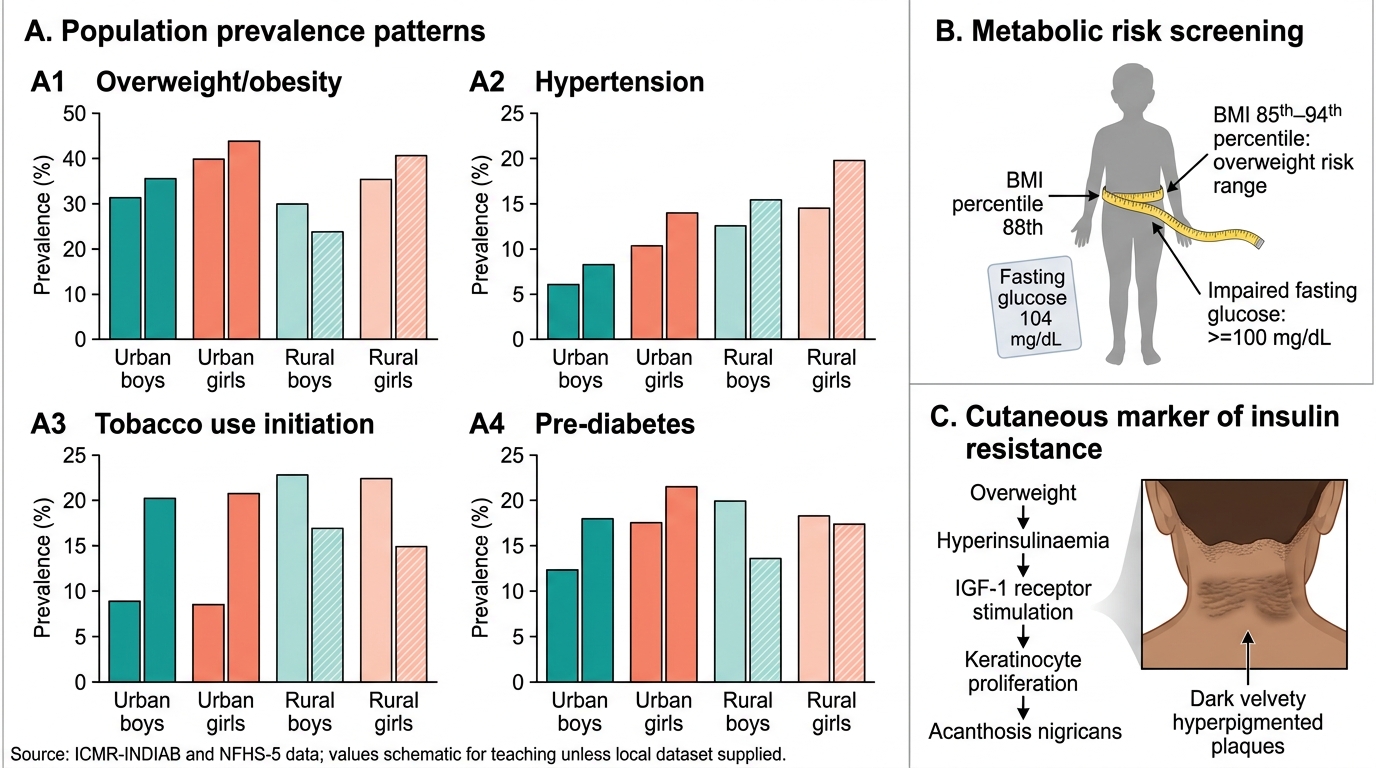
The epidemiological data on NCD risk in Indian adolescents have evolved rapidly since the NFHS-5 (2019–21), ICMR-INDIAB, and multiple school-based survey datasets became available. The picture that emerges is one of a rapidly rising burden that is no longer an urban elite problem — it is tracking across socioeconomic strata, with important urban–rural and sex differentials.
Obesity and overweight: National survey data suggest 4–8% of adolescents are obese and 10–15% overweight on IAP cut-offs, with significantly higher rates in urban, private-school-going adolescents (where prevalence can exceed 20–25% overweight/obese in some studies). Among lower-income and rural adolescents, undernutrition still dominates, but urban poor adolescents increasingly show co-existing stunting and overweight — the so-called double burden household.
Hypertension: Studies from Indian schools and urban adolescent clinics report hypertension prevalence of 8–14% among adolescents, with overweight/obesity as the strongest predictor. Most cases are not symptomatic and are discovered only on routine BP measurement — reinforcing why BP measurement is a mandatory component of the adolescent health checkup.
Pre-diabetes and type 2 diabetes: Indian adolescents with obesity have a high risk of insulin resistance and impaired fasting glucose, particularly given the South Asian phenotype (metabolic risk at lower BMI than Western populations; greater visceral adiposity for a given BMI). ICMR-INDIAB 2023 data indicate India has over 100 million diabetics; a significant and growing proportion is in the 15–30-year age group. Type 2 diabetes in adolescence — once extremely rare — is now being increasingly reported from tertiary centres.
Tobacco and substance use: GATS (Global Adult Tobacco Survey) India data show tobacco initiation before age 18 in over 60% of adult tobacco users. School health surveys document 10–15% tobacco use (any form) among adolescent boys in some states. Smokeless tobacco (gutka, khaini) is particularly prevalent in lower-income adolescents and is directly linked to oral cancer risk.
Dyslipidaemia and cardiovascular risk: Studies in obese Indian adolescents report dyslipidaemia (elevated LDL-C, low HDL-C, elevated triglycerides) in 30–50% of cases — rates comparable to metabolic syndrome criteria in adults. Early atherosclerotic changes (elevated carotid intima-media thickness) have been demonstrated in obese adolescents as young as 12–14 years.
Adolescent Metabolic and Behavioural Risk Patterns in India
SELF-CHECK
A 14-year-old boy has a BMI at the 88th percentile for age and sex on the IAP growth chart, a fasting blood glucose of 104 mg/dL, and visible dark velvety patches on the nape of his neck. Which metabolic condition do the skin findings suggest?
A. Addison's disease (adrenal insufficiency)
B. Insulin resistance (acanthosis nigricans)
C. Hypothyroidism
D. Tinea versicolor
Reveal Answer
Answer: B. Insulin resistance (acanthosis nigricans)
Acanthosis nigricans — dark, velvety, hyperpigmented skin changes at the neck, axilla, and groin — is a well-recognised cutaneous marker of insulin resistance. It results from stimulation of keratinocyte proliferation by elevated circulating insulin acting on IGF-1 receptors. In an overweight adolescent (BMI at 88th percentile) with impaired fasting glucose (104 mg/dL, above the 100 mg/dL threshold for IFG), acanthosis nigricans strongly suggests metabolic syndrome and should prompt full evaluation: fasting lipid profile, fasting insulin, OGTT if indicated. Addison's disease causes hyperpigmentation but in a generalised distribution with adrenal insufficiency symptoms; hypothyroidism causes skin changes but not velvety neck patches; tinea versicolor is a fungal infection with hypo- or hyperpigmented scaly patches.
Mechanisms and Determinants of NCD Risk in Adolescents
The mechanisms linking adolescent lifestyle factors to adult NCD outcomes form an interconnected web rather than isolated causal chains. Understanding these mechanisms is essential because it enables you to counsel adolescents (and their parents) with genuine explanatory power — not just a list of 'don'ts', but a mechanistic narrative that motivates change.
Central role of obesity and metabolic syndrome:
Obesity — specifically visceral/central adiposity — is the master driver of most adolescent NCD risk. Visceral adipose tissue is metabolically active: it secretes pro-inflammatory cytokines (TNF-α, IL-6), free fatty acids, and leptin while reducing adiponectin (a cardioprotective adipokine). This adipose-derived inflammatory and metabolic milieu drives insulin resistance in the liver and skeletal muscle, leading to elevated fasting insulin, impaired glucose tolerance, and eventually type 2 diabetes. The same inflammatory state damages endothelial cells, promotes atherogenic dyslipidaemia (elevated VLDL, LDL, triglycerides; reduced HDL), and activates the renin-angiotensin-aldosterone system — raising blood pressure. The cluster of central obesity + hypertension + dyslipidaemia + impaired fasting glucose = metabolic syndrome, which carries a 5-fold increased risk of cardiovascular disease.
Determinants of adolescent obesity:
Obesity in adolescence results from a chronic energy imbalance (energy intake > expenditure), but the specific drivers in the Indian context include:
• Ultra-processed food consumption: high in added sugars, saturated fats, sodium; energy-dense but micronutrient-poor; marketed aggressively to adolescents
• Sugar-sweetened beverages: each 250 mL serving of cola adds ~100 kcal with no satiety; strong dose-response relationship with adolescent obesity
• Physical inactivity: decline in structured physical activity with transition from primary to secondary school; displacement of outdoor play by screen time
• Screen time: WHO/IAP recommends ≤2 hours recreational screen time daily for adolescents; >4 hours associated with sedentary behaviour, disrupted sleep, and increased food marketing exposure
• Sleep deprivation: adolescents sleeping <7 hours have higher ghrelin (hunger hormone) and lower leptin (satiety), driving increased caloric intake
• Socioeconomic factors: in upper-income urban families, excess caloric intake from processed foods; in lower-income families, micronutrient deficiency + emerging caloric surplus in urban slums
Tobacco and cancer risk:
Tobacco initiation in adolescence is particularly dangerous because the developing brain and lung are more susceptible to carcinogen damage, and because the duration of exposure before cancer manifests (typically 20–30 years) means adolescent initiators experience cancer risk at younger ages than adult initiators. Smokeless tobacco in India contains highly carcinogenic nitrosamines and is directly associated with oral submucous fibrosis and oral cancer.
Mental health as an NCD:
The WHO classifies mental health disorders as NCDs. Depression, anxiety disorders, and substance use disorders — with peak onset in adolescence — carry their own direct health burden and interact with physical NCDs: depression worsens metabolic syndrome outcomes; substance use is a risk factor for liver disease, cardiovascular disease, and cancer.
Social determinants:
NCD risk is not evenly distributed — urban residence, high-income household, sedentary school environment, and food environment are social determinants that cluster NCD risk. However, the adolescent period is the last window in which behaviour-change interventions have maximum efficacy before adult risk behaviour patterns solidify.
CLINICAL PEARL
Clinical Pearl — The South Asian Paradox: Metabolic Risk at Lower BMI:
South Asians, including Indians, have significantly higher visceral adiposity and insulin resistance for any given BMI compared to Caucasians — a phenomenon called the 'South Asian phenotype' or 'thin-fat Indian'. This means that an Indian adolescent with a BMI at the 75th–80th percentile (technically 'normal' on Western cut-offs) may already have meaningful metabolic risk. The IAP-adapted BMI cut-offs are appropriate, but clinically you should measure waist circumference and look for acanthosis nigricans in any adolescent with a family history of diabetes or cardiovascular disease, regardless of their absolute BMI percentile. A waist circumference >90th percentile for age and sex indicates central adiposity even in the 'normal' BMI range.