Page 22 of 28
PE6.11 | Adolescent Non Communicable Disease Risk — SDL Guide (Part 2)
Clinical and Applied Significance: Prevention and Screening
The clinical application of adolescent NCD knowledge is primarily through structured screening within the adolescent health checkup and AFHC, combined with targeted lifestyle counselling and timely referral. The physician's role at first-contact is not to diagnose and treat adult-pattern NCDs in adolescents — that is a tertiary role — but rather to identify risk early, provide evidence-based preventive counselling, and escalate appropriately when thresholds are crossed. Primary prevention (preventing risk-factor acquisition — stopping the 14-year-old from initiating tobacco, reducing the 15-year-old's sugar-sweetened beverage intake) and secondary prevention (identifying early risk such as pre-hypertension or impaired fasting glucose and arresting progression before frank disease develops) are both achievable within the AFHC model. The key to making this practical is using a structured screening protocol rather than relying on clinical intuition, since most adolescent NCD risk is asymptomatic and will not be detected without deliberate measurement.
Provided image
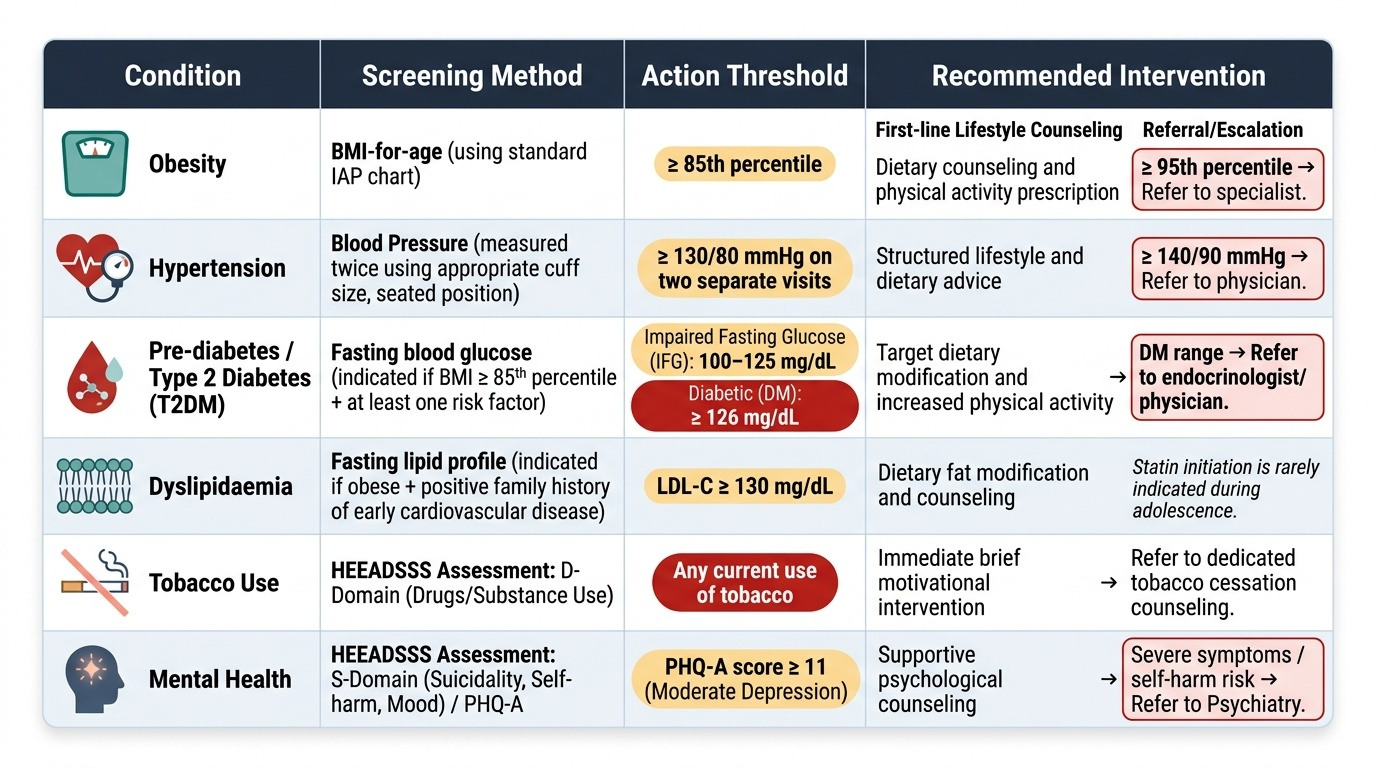
Structured NCD screening at AFHC:
| Condition | Screening Method | Action Threshold | Response |
|---|---|---|---|
| Obesity | BMI-for-age (IAP chart) | ≥85th percentile | Dietary counselling, activity prescription; ≥95th = refer |
| Hypertension | BP (appropriate cuff, seated, ×2) | ≥130/80 on two visits | Lifestyle advice; ≥140/90 = refer to physician |
| Pre-diabetes / T2DM | Fasting glucose if BMI ≥85th + risk factor | ≥100 mg/dL (IFG); ≥126 mg/dL (DM) | Dietary change, activity; DM = refer |
| Dyslipidaemia | Fasting lipid profile if obese + family history | LDL-C ≥130 mg/dL | Dietary fat modification; statin rarely needed in adolescence |
| Tobacco | HEEADSSS D-domain | Any current use | Brief intervention; refer to cessation counselling |
| Mental health | HEEADSSS S-domain (mood, self-harm) | PHQ-A ≥11 (moderate depression) | Counselling; refer to psychiatry if severe |
The four shared modifiable NCD risk factor messages for adolescents:
- Unhealthy diet: reduce sugar-sweetened beverages, ultra-processed food, and excess sodium; increase fruit, vegetables, pulses, and whole grains. Practical: replace cola with water or lassi; eat home-cooked food at least once daily.
- Physical inactivity: ≥60 minutes of moderate-to-vigorous physical activity daily (WHO recommendation for adolescents); include at least 3 sessions of bone-strengthening activity weekly. Practical: walk to school, take stairs, join a sport.
- Tobacco: zero tolerance for initiation; brief advice at every visit; enlist peer pressure positively. Smokeless tobacco is equally carcinogenic — address it specifically.
- Harmful alcohol: early initiation is a strong risk factor for alcohol use disorder; liver disease in adolescence; brain development disruption. Brief motivational advice under HEEADSSS D-domain.
When to refer:
Adolescents with confirmed hypertension (≥140/90 on two measurements), fasting glucose ≥126 mg/dL, severe obesity (BMI ≥99th percentile), or dyslipidaemia unresponsive to dietary change should be referred to a paediatric medicine specialist or district hospital. Mental health referral criteria are as described in the AFHS module.
SELF-CHECK
According to WHO recommendations for adolescents, what is the minimum daily duration of moderate-to-vigorous physical activity recommended to reduce NCD risk?
A. 30 minutes daily
B. 45 minutes daily
C. 60 minutes daily
D. 90 minutes daily
Reveal Answer
Answer: C. 60 minutes daily
WHO recommends that children and adolescents (5–17 years) accumulate at least 60 minutes of moderate-to-vigorous physical activity daily for health benefit, including NCD risk reduction. This is substantially higher than the 150 minutes per week (≈21 minutes/day) recommended for adults, reflecting the greater developmental benefit of physical activity during the growth period. In addition, muscle- and bone-strengthening activities should be incorporated at least 3 days per week. This 60-minutes/day target is the benchmark used in adolescent health counselling and school health programme recommendations.
Self-Assessment
The questions below are designed to test whether you can enumerate and explain adolescent NCD importance — the core demand of competency PE6.11. Notice that the competency uses the word 'enumerate': you are expected not just to name conditions but to articulate WHY they matter in this age group. In examinations, a list without rationale will not fully satisfy the question. Practise constructing answers that name the condition, explain the prevalence and magnitude in India, state the mechanism linking it to adult disease, and identify the specific prevention opportunity available in the adolescent window. This four-part structure maps directly to the PE-foundation arc — orientation, magnitude, mechanism, clinical significance — and is exactly how a high-scoring answer to a 'discuss NCD in adolescents' question should be organised in your professional examinations.
- Name six NCD risk factors identifiable in an adolescent during a routine health checkup, and for each state one specific screening method.
- Why does obesity have a disproportionately large impact on adult NCD burden when it begins in adolescence compared with obesity onset in adulthood?
- What is acanthosis nigricans? What metabolic condition does it signal, and why is it clinically important in an obese adolescent?
- State the WHO daily physical activity recommendation for adolescents and explain the physiological basis for this being higher than the adult recommendation.
- A 13-year-old girl lives in an urban slum, has a BMI at the 87th percentile, and her mother is diabetic. What is your NCD risk assessment and what is your counselling plan?
- Explain the 'South Asian phenotype' of metabolic risk and its implication for using BMI-for-age alone as the NCD screening metric in Indian adolescents.