Page 4 of 21
PE7.1-3 | Breastfeeding Physiology and Milk Composition — SDL Guide
Learning Objectives
- Explain the anatomy of the lactating breast and the neuroendocrine physiology of lactation, including the roles of prolactin and oxytocin
- Describe the temporal sequence of milk secretion (colostrum, transitional, mature milk) and their compositional differences
- Compare the composition of human milk and cow's milk, explaining why cow's milk is unsuitable for infants under one year
- Enumerate the nutritional, immunological, neurodevelopmental, maternal, and economic advantages of breastfeeding
- Recognise common cultural beliefs and practices that impair breastfeeding, and counsel mothers to overcome them
INSTRUCTIONS
Breastfeeding is the single most cost-effective public-health intervention for reducing infant morbidity and mortality worldwide. In India, suboptimal breastfeeding — including delayed initiation, prelacteal feeds, and early weaning — contributes substantially to neonatal deaths and under-five malnutrition. As a future paediatrician you will counsel every postnatal mother on breastfeeding, respond to cultural barriers at the bedside, and manage conditions such as mastitis or inadequate milk supply. Understanding the physiology behind lactation and the science of milk composition gives you the evidence base for that counselling — it transforms 'breast is best' from a slogan into a clinically defensible recommendation you can explain and defend.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 7 — Infant Feeding (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 55 — Breast Milk (textbook)
- IAP Policy Statement on Breastfeeding, 2023 (guideline)
- WHO/UNICEF Baby-Friendly Hospital Initiative (BFHI) Ten Steps to Successful Breastfeeding (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Baby Ananya, born at term by normal delivery, is brought to you at 48 hours of life. Her mother looks anxious and tells you: 'Doctor, my mother-in-law says my first milk is watery and bad for the baby. She wants me to give the baby some honey water first and start formula until my real milk comes in.' The baby's weight is down 180 g from birth, she is slightly jaundiced, and she has passed only one meconium stool. How do you counsel this mother — and what is the physiology behind the advice you are about to give?
WHY THIS MATTERS
Breastfeeding physiology underpins almost every conversation you will have in the newborn nursery and well-baby clinic. The hormonal drivers of lactation explain why frequent demand feeding establishes milk supply, why separation of mother and baby derails it, and why anxiety can inhibit the let-down reflex. Knowing the composition of colostrum versus mature milk explains why delaying breastfeeding for even 24–48 hours deprives the newborn of passive immunity at its most vulnerable window. Understanding how human and cow's milk differ allows you to counsel families against inappropriate formula use and to explain why cow's milk causes iron-deficiency anaemia and renal solute overload in infants under one year. This foundational knowledge is the science behind BFHI policy — and the evidence you need when cultural beliefs conflict with safe infant feeding.
RECALL
Before proceeding, activate what you already know. From Physiology (PY): the hypothalamic-pituitary axis regulates anterior and posterior pituitary hormone secretion; prolactin is an anterior pituitary hormone regulated by dopaminergic inhibitory control; oxytocin is a posterior pituitary peptide released by the paraventricular nucleus in response to suckling and other stimuli. From Anatomy (AN): the breast is a modified sweat gland composed of 15–20 glandular lobes, each draining via a lactiferous duct to the nipple; alveoli lined by secretory epithelial cells and surrounded by myoepithelial cells form the functional unit. From Biochemistry (BI): immunoglobulins are glycoproteins; secretory IgA (sIgA) is the mucosal immunoglobulin, distinct from serum IgG. Hold these concepts — they are the framework on which lactation physiology is built.
Orientation: Why Breastfeeding Matters in Paediatric Practice
Breastfeeding is not merely a feeding method — it is a biological system evolved over millions of years to deliver optimal nutrition, passive immunity, and growth signals to the human infant. The World Health Organization (WHO) and Indian Academy of Pediatrics (IAP) recommend exclusive breastfeeding for the first six months of life, followed by continued breastfeeding alongside appropriate complementary foods until two years or beyond. These recommendations are grounded in decades of evidence showing that exclusively breastfed infants have substantially lower rates of diarrhoeal illness, acute respiratory infections, otitis media, urinary tract infections, and necrotising enterocolitis compared with formula-fed infants. In low- and middle-income countries, including India, suboptimal breastfeeding is estimated to account for 11–13% of all under-five deaths.
In India, the National Family Health Survey (NFHS-5, 2019–2021) reports that only about 63.7% of infants under 6 months are exclusively breastfed — a figure that varies widely by state, rural-urban setting, and maternal education. Prelacteal feeding (giving honey, water, formula, or animal milk before the first breastfeed) is practised in approximately 30% of households and is associated with increased neonatal mortality. The Baby-Friendly Hospital Initiative (BFHI), implemented in India through the Ministry of Health and Family Welfare, mandates that all birthing facilities follow the Ten Steps to Successful Breastfeeding, including putting the baby to the breast within one hour of birth (ideally within 30 minutes for vaginal delivery) and rooming-in of mother and baby.
Understanding these epidemiological and policy realities contextualises the clinical science that follows. Every physiological mechanism you learn in this module has a direct corollary in breastfeeding counselling: the prolactin surge explains why early initiation is essential; the let-down reflex explains why a calm, supportive environment matters; the immunological richness of colostrum explains why discarding it is harmful.
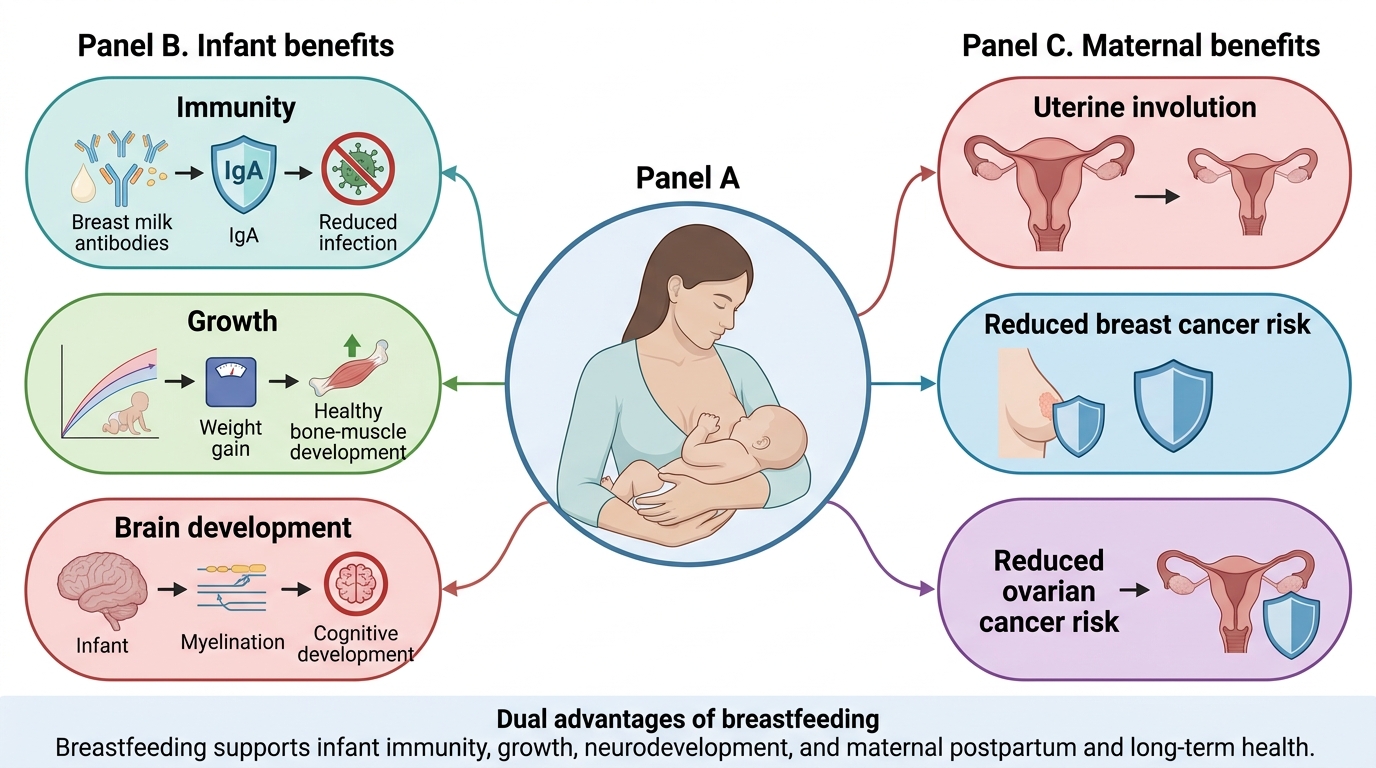
Dual Benefits of Breastfeeding
Breast Anatomy and Lactation Physiology
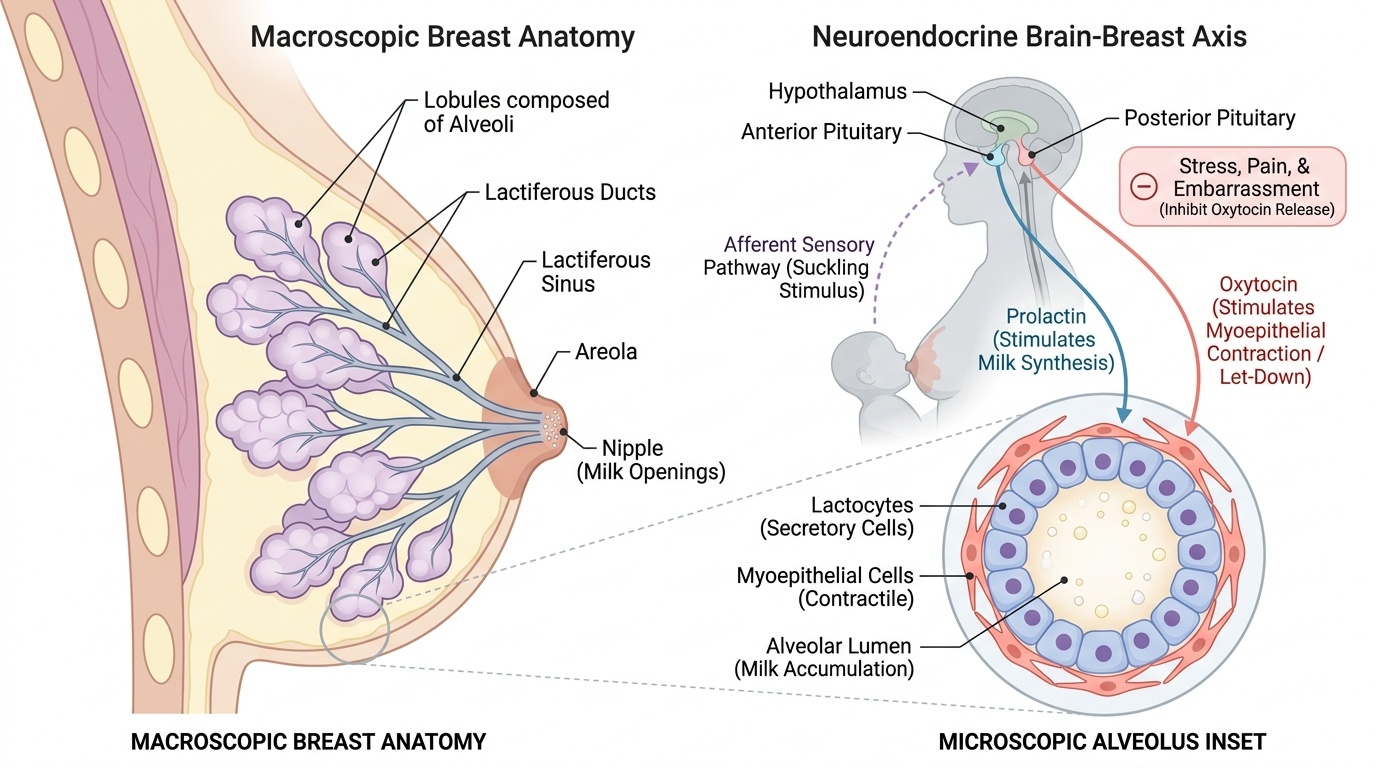
The lactating breast is organised into 15–20 lobes, each subdivided into lobules composed of alveoli — the secretory units where milk is synthesised. Each alveolus is lined by a single layer of secretory epithelial cells (lactocytes) surrounded by myoepithelial cells capable of contraction. Milk synthesised in the alveolus drains into progressively larger lactiferous ducts, which converge beneath the areola into lactiferous sinuses, and exit through the nipple via 15–20 small openings.
Provided image
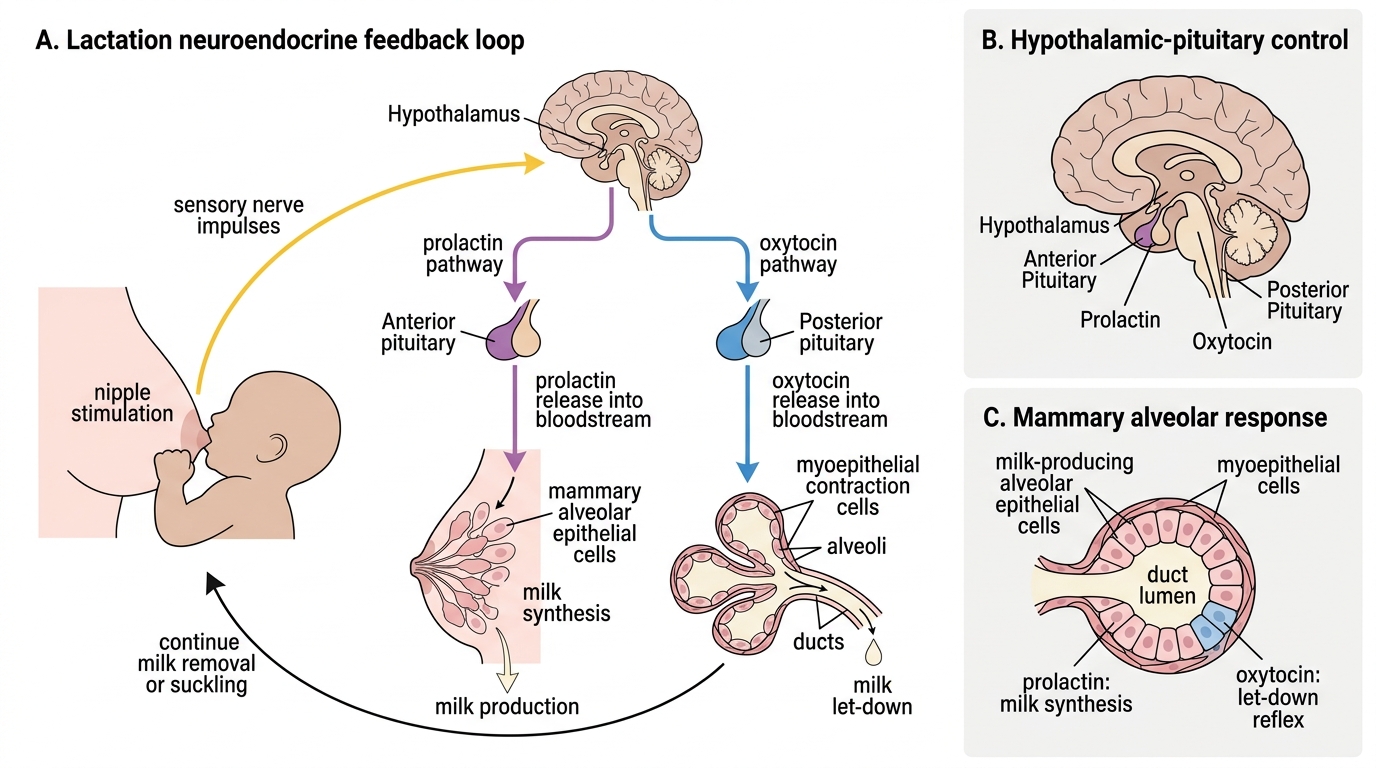
Lactation is governed by two key pituitary hormones in a precisely coordinated neuroendocrine reflex:
1. Prolactin (milk synthesis): Prolactin is secreted by lactotroph cells of the anterior pituitary. During pregnancy, rising oestrogen and progesterone stimulate prolactin secretion but suppress lactogenesis at the alveolar level. After delivery, the fall in placental oestrogen and progesterone removes this suppression. When the infant suckles, mechanoreceptors in the nipple-areola transmit afferent signals via spinal pathways to the hypothalamus, inhibiting dopamine (prolactin-inhibiting factor) secretion and triggering a surge of prolactin. Prolactin acts on lactocytes to stimulate milk synthesis from precursors (glucose, fatty acids, amino acids). The prolactin surge is greatest with early, frequent suckling — the basis for the demand-driven establishment of milk supply in the first days of life.
2. Oxytocin (milk ejection / let-down reflex): The same suckling stimulus — and conditioned stimuli such as hearing the baby cry — activates magnocellular neurons in the hypothalamic paraventricular and supraoptic nuclei, which release oxytocin from the posterior pituitary. Oxytocin acts on myoepithelial cells surrounding the alveoli, causing them to contract and expel milk into the ducts — the let-down reflex or milk ejection reflex. Without a functional let-down, milk cannot be effectively removed from the breast even if supply is adequate. Emotional stress, pain, and embarrassment all inhibit oxytocin release via hypothalamic pathways, explaining why a calm, private, supportive feeding environment is clinically important.
Key points to remember:
• Prolactin = milk production (synthesis in alveoli; anterior pituitary)
• Oxytocin = milk ejection (let-down; posterior pituitary)
• Frequent suckling → maintains prolactin levels → sustains milk supply (supply=demand principle)
• Engorgement and missed feeds → prolactin falls → supply diminishes
SELF-CHECK
A mother complains that her milk 'does not come out' when she tries to feed, even though she can feel the breast is full. She is tense and anxious about her baby's weight loss. Which hormone deficiency most directly explains this presentation?
A. Prolactin — because anxiety suppresses anterior pituitary secretion
B. Oxytocin — because emotional stress inhibits the let-down (milk ejection) reflex
C. Oestrogen — because postnatal oestrogen fall prevents milk synthesis
D. Cortisol — because stress raises cortisol which destroys milk protein
Reveal Answer
Answer: B. Oxytocin — because emotional stress inhibits the let-down (milk ejection) reflex
Oxytocin is released from the posterior pituitary in response to suckling and conditioned stimuli; emotional stress, pain, and anxiety inhibit its release via hypothalamic dopaminergic and noradrenergic pathways. The result is a failure of the let-down (milk ejection) reflex — the breast fills but milk cannot be expelled. Prolactin drives synthesis but not ejection. Oestrogen fall after delivery is what enables lactation (removes inhibition). Cortisol does not destroy milk protein.
Types of Breast Milk: Colostrum, Transitional, and Mature Milk
Breast milk is not a static fluid — it changes dramatically in composition over the first weeks of life to match the evolving nutritional and immunological needs of the newborn. The newborn at birth has a gastric capacity of only 5–7 mL, a gut that has never encountered oral nutrition, and an immune system with virtually no prior antigen exposure. Each phase of milk production is specifically calibrated for this developmental trajectory: the dense, small-volume colostrum of the first days matches the tiny stomach capacity and delivers maximal immunological payload precisely when neonatal immunity is most vulnerable; the rising volume and fat content of transitional milk mirrors the rapid growth rate of the first two weeks; and the more dilute foremilk-to-concentrated-hindmilk progression within each mature feed provides both hydration and energy in a single, elegant delivery mechanism. Understanding this temporal progression is clinically important because interrupting it at any stage — by prelacteal feeds, formula supplementation, or premature weaning — disrupts a finely tuned biological sequence. Three temporally distinct types are recognised:
1. Colostrum (days 1–3 postpartum): Colostrum is the thick, yellowish, high-protein fluid secreted in the immediate postnatal period. It is produced in small volumes (30–40 mL/day on day 1, rising to 150–300 mL/day by day 3), which is appropriate for the newborn's tiny gastric capacity (~5–7 mL). Its defining features are:
• Very high secretory IgA (sIgA) concentration — the single most important immune factor; coats the neonatal gut mucosa and prevents pathogen adherence
• High lactoferrin (iron-binding, bacteriostatic) and lysozyme (bacteriolytic enzyme)
• High protein content, predominantly whey fraction, easily digested
• Growth factors (EGF, IGF-1) — promote gut epithelial maturation and intestinal villi development
• Lower fat and lactose than mature milk — suitable for immature gut enzyme capacity
• Mild laxative effect — promotes passage of meconium, reducing neonatal jaundice
• Vitamin K — substantial amounts protect against haemorrhagic disease of the newborn
Colostrum has been called the 'first vaccine' — its immunological value cannot be replicated by any formula. Discarding colostrum on cultural grounds (the 'bad first milk' belief) deprives the infant of this protection at the most vulnerable window.
2. Transitional milk (days 3–14): As milk volume increases rapidly (to 500–750 mL/day by day 7), composition shifts toward mature milk. sIgA concentration falls as volume rises, but total sIgA output remains constant or increases. Fat and lactose content rises; protein falls.
3. Mature milk (after 14 days): Mature milk has lower protein than colostrum but higher fat and lactose (energy density ~0.65–0.70 kcal/mL). Within a single feed, foremilk (milk at the start of a feed) is watery and high in lactose; hindmilk (late-feed milk) is rich in fat and delivers the majority of the energy. This is why ensuring the infant empties one breast before switching ensures adequate fat and calorie delivery — cutting feeds short leaves the infant hungry despite adequate volume.
Neuroendocrine Control of Lactation