Page 5 of 21
PE7.1-3 | Breastfeeding Physiology and Milk Composition — SDL Guide (Part 2)
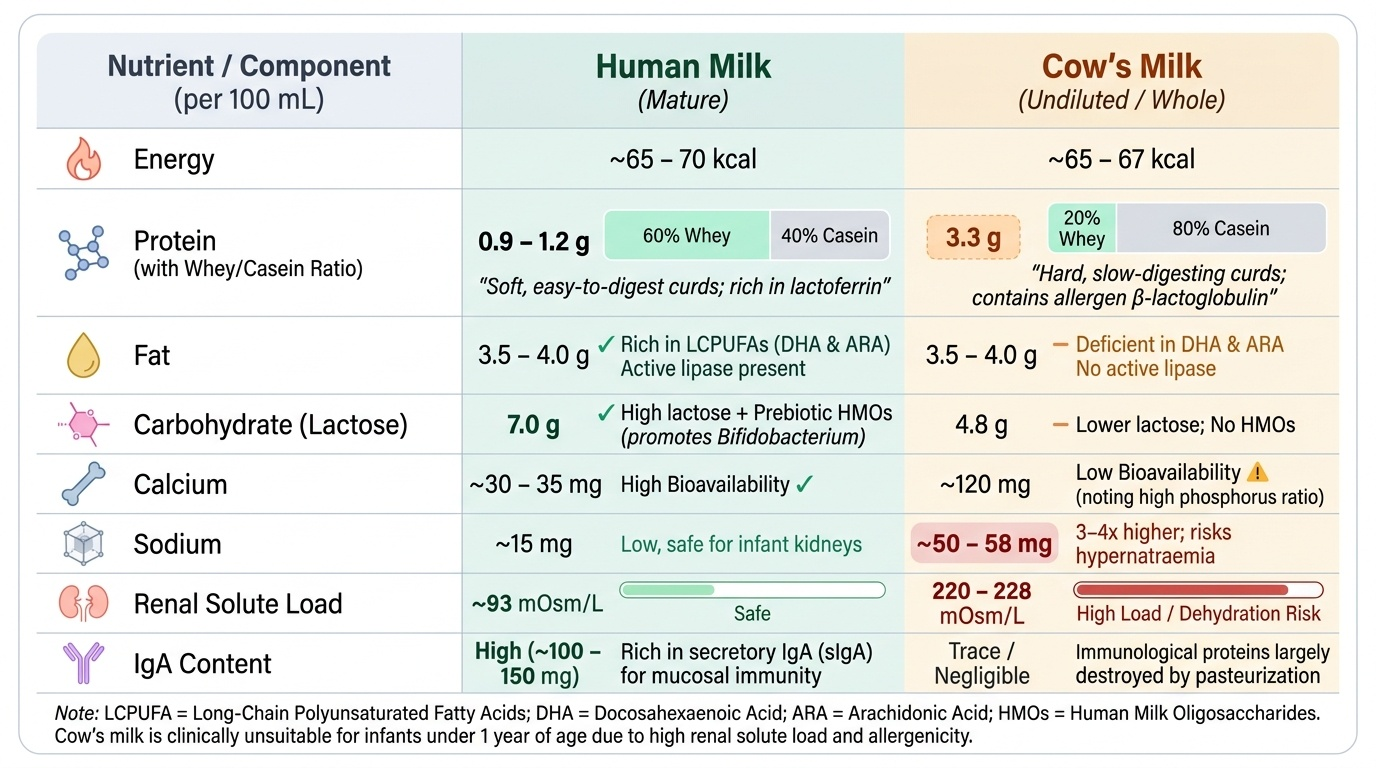
Composition of Human Milk vs Cow's Milk
Understanding the compositional differences between human milk and cow's milk is clinically essential because cow's milk — undiluted or as formula — is frequently introduced prematurely in India, and it carries specific harms when given to infants under one year of age. The differences span every macronutrient category and immunological fraction.
Provided image
Protein: Human milk contains 0.9–1.2 g/100 mL protein with a whey:casein ratio of approximately 60:40 in mature milk (rising to 90:10 in colostrum). Whey proteins (α-lactalbumin, lactoferrin, sIgA, lysozyme) are soft, rapidly digestible, and largely immunologically active. Cow's milk has 3.3 g/100 mL protein with a casein:whey ratio of 80:20 — forming hard, slow-digesting curds and presenting a high renal solute load. The specific amino acid profile of human whey is optimised for neonatal metabolism; cow's whey contains β-lactoglobulin, which is a common allergen absent from human milk.
Fat: Both milks contain ~3.5–4 g/100 mL total fat, but the fatty-acid profile differs critically. Human milk is rich in long-chain polyunsaturated fatty acids (LCPUFAs) — especially docosahexaenoic acid (DHA) and arachidonic acid (ARA) — which are essential for retinal and brain myelination. Human milk also contains bile-salt-stimulated lipase, which initiates fat digestion in the duodenum even before pancreatic lipase is fully active. Cow's milk is deficient in DHA/ARA.
Carbohydrate: Human milk contains 7 g/100 mL lactose — higher than cow's milk (4.8 g/100 mL) — providing the primary energy source and promoting calcium absorption. Human milk additionally contains human milk oligosaccharides (HMOs) — over 200 complex oligosaccharide structures that act as prebiotics, promoting Bifidobacterium colonisation of the gut microbiome and blocking pathogen adhesion. HMOs are not present in cow's milk.
Minerals: Cow's milk has 3–4 times the sodium, potassium, chloride, calcium, and phosphorus of human milk. While absolute calcium is higher in cow's milk, its bioavailability is lower due to the high phosphorus ratio. The high renal solute load of cow's milk (220–228 mOsm/L vs ~93 mOsm/L for human milk) overwhelms the immature neonatal kidney's concentrating capacity, increasing risk of dehydration, hypernatraemia, and metabolic acidosis.
Iron: Human milk contains only 0.3 mg/L iron — but its bioavailability is 50–70%, compared with only 4–10% from cow's milk, due to lactoferrin and the acid-whey pH. Cow's milk also causes occult intestinal blood loss via direct mucosal irritation, contributing to iron-deficiency anaemia in infants given cow's milk before 12 months.
Immunological factors: Human milk contains sIgA, IgM, IgG, lactoferrin, lysozyme, complement components, macrophages, lymphocytes, and neutrophils. Cow's milk lacks these in bioactive form and provides no passive immune benefit to the infant.
| Component | Human milk (per 100 mL) | Cow's milk (per 100 mL) |
|---|---|---|
| Energy (kcal) | 65–70 | 67 |
| Protein (g) | 0.9–1.2 | 3.3 |
| Whey:Casein | 60:40 | 20:80 |
| Fat (g) | 3.5–4.0 | 3.7 |
| Carbohydrate (g) | 7.0 | 4.8 |
| Calcium (mg) | 34 | 120 |
| Sodium (mg) | 15 | 55 |
| Renal solute load (mOsm/L) | ~93 | ~220–228 |
| Secretory IgA | Present (high) | Absent (bioactive) |
The clinical bottom line: cow's milk is not recommended for infants under 12 months — it causes iron-deficiency anaemia, renal solute overload, and allergic sensitisation, and lacks the neurodevelopmental fatty acids and immune factors of human milk.
Advantages of Breastfeeding
The advantages of breastfeeding are multi-dimensional — they span infant nutrition, immunological protection, neurodevelopment, the mother's health, and wider socioeconomic benefits. Knowing this evidence base allows you to counsel with specificity rather than platitudes.
Nutritional advantages:
Human milk is uniquely formulated for the human infant — it provides all macronutrients and micronutrients in optimal amounts and bioavailability for the first six months of life without any supplementation. Its composition adapts dynamically: milk from mothers of preterm infants has higher protein and sodium for the specific needs of the premature gut; the fat content of each feed rises progressively from foremilk to hindmilk, naturally regulating energy intake.
Immunological advantages:
Every feed delivers a complex of immunoprotective factors. Secretory IgA provides passive mucosal immunity against enteric pathogens, significantly reducing the incidence of diarrhoea and acute respiratory infections. Lactoferrin chelates iron, depriving pathogens of a critical growth factor, and has direct bactericidal and antiviral activity. Lysozyme disrupts bacterial cell walls. Human milk oligosaccharides function as decoy receptors and as prebiotics, promoting a protective microbiome dominated by Bifidobacterium. Live macrophages and lymphocytes provide cellular immunity. These factors work synergistically — formula provides none of them. Evidence from large Indian cohorts shows that exclusive breastfeeding for six months reduces diarrhoea incidence by ~50% and pneumonia mortality by ~15%.
Neurodevelopmental advantages:
DHA and ARA in human milk are incorporated into neuronal cell membranes and retinal photoreceptors during the critical window of brain growth in the first year of life. Multiple meta-analyses associate breastfeeding duration with modestly higher cognitive scores (IQ benefit ~3–4 points in observational studies, with dose-response by duration), better visual acuity, and reduced risk of childhood ADHD. The physical act of suckling at the breast also promotes orofacial muscle development and jaw growth.
Reduced risk of disease:
Breastfed infants have substantially lower rates of: otitis media, necrotising enterocolitis (NEC — especially in preterm infants, where exclusive breastfeeding reduces NEC risk by ~4-fold), urinary tract infections, bacteraemia, Haemophilus influenzae meningitis, and in later life, asthma, eczema, type 1 diabetes, inflammatory bowel disease, and obesity. Sudden infant death syndrome (SIDS) risk is also reduced.
Maternal advantages:
• Uterine involution: Oxytocin released during suckling causes myometrial contraction, reducing postpartum haemorrhage and accelerating return to pre-pregnancy uterine size.
• Lactational amenorrhoea (LAM): Elevated prolactin suppresses GnRH pulsatility, inhibiting ovulation — providing approximately 98% contraceptive efficacy if the infant is exclusively breastfed, <6 months old, and menses have not returned. This natural child-spacing benefit has significant public-health implications in India.
• Weight loss: Lactation requires approximately 500 kcal/day above baseline — supporting return to pre-pregnancy weight.
• Reduced cancer risk: Breastfeeding is associated with reduced lifetime risk of breast and ovarian cancer, with each 12 months of cumulative breastfeeding reducing breast cancer risk by approximately 4.3% (Collaborative Group on Hormonal Factors in Breast Cancer).
• Psychological bonding: The oxytocin released during breastfeeding promotes maternal-infant attachment and reduces rates of postpartum depression.
Economic and public-health advantages:
Breastfeeding eliminates the cost of formula (~₹1,500–3,000/month for standard formula in India), reduces healthcare expenditures from prevented illnesses, and is accessible without clean water or refrigeration. At a population level, optimal breastfeeding could prevent an estimated 820,000 child deaths per year globally.
CLINICAL PEARL
The foremilk-hindmilk principle in clinical practice: A common reason for poor weight gain in an apparently well-latched breastfed baby is premature switching — the mother moves the baby to the second breast before the first is adequately drained. The fat-rich hindmilk remains in the first breast; the infant gets the high-lactose, low-calorie foremilk from two breasts and is calorically underfed. The clinical fix is simple: advise the mother to feed from one breast until it feels soft and empty before offering the second. If the second breast is not taken, offer it at the next feed. This alone often resolves perceived 'insufficient milk supply.'
Cultural Beliefs and Breastfeeding Practices in India
India's diverse cultural landscape has generated numerous traditional beliefs around infant feeding, many of which are harmful. As a paediatrician, you will encounter these at every level of practice — from urban tertiary-care nurseries to rural primary-health centres. The clinical approach is non-judgmental acknowledgement followed by factual, respectful education.
Common harmful practices and their evidence-based counter-arguments:
1. Discarding colostrum ('bad milk / dirty milk'): Widely believed in many Indian communities to be too concentrated, too yellow, or unsafe. In reality, colostrum is the most immunologically active milk ever produced — the sIgA, lactoferrin, and growth factors in colostrum during the first 2–3 days are irreplaceable. Withholding it strips the newborn of passive gut immunity at the most critical window. Counter with: 'The first yellow milk is the baby's first vaccine — it lines the gut and protects against infection.'
2. Prelacteal feeds (honey, glucose water, cow's milk, janam ghuti, goat milk, sugar water): Given on the first day 'before the milk comes in.' These are harmful in multiple ways: honey carries the risk of infant botulism (Clostridium botulinum spores); cow's milk causes sensitisation and iron-deficiency anaemia; glucose water fills the stomach and reduces suckling frequency, impairing milk-supply establishment; all prelacteal feeds carry infection risk if prepared with contaminated water. They also delay the frequency of suckling needed to establish prolactin-driven milk supply. Counter with physiology: 'The baby's stomach holds only 5–7 mL on day 1 — the small amount of colostrum is exactly right.'
3. Restricting certain foods for the mother ('hot foods' harm milk): Maternal dietary restrictions — avoiding lentils, citrus, tomato, eggs, certain spices — are extremely common and lead to maternal malnutrition. Human milk composition is remarkably stable across maternal diets; a well-nourished mother eating a varied diet does not need food restrictions. Flavour molecules do pass into milk (garlic, onion) but these do not harm the infant and may actually improve later food acceptance. The mother's caloric and hydration adequacy matters far more than specific food avoidance.
4. Early introduction of cow's milk or cereal ('mother's milk is not enough' after 2–3 months): This belief often drives premature weaning in Indian households. Reassure that exclusive breastfeeding provides all nutrition for the first 6 months — hunger cues and frequent night waking are developmentally normal, not signs of inadequate milk. Complementary foods should start at exactly 6 months (not earlier).
5. Maternal illness or stress as a reason to stop: Minor maternal illness (upper respiratory tract infection, mild fever, mastitis) is NOT a contraindication to breastfeeding — in fact, continuing breastfeeding during mild maternal infection transmits protective antibodies to the infant. The exceptions are few and specific: untreated active tuberculosis with sputum-positive disease, HIV in settings with safe formula access per NACO guidelines, and certain cytotoxic drugs. Reassure mothers that stress does not 'spoil' milk — but it may inhibit the let-down reflex, which resolves with relaxation.
BFHI Ten Steps — the policy framework: The BFHI mandates that all birthing facilities support breastfeeding through its Ten Steps, which include: initiating skin-to-skin contact within one hour of birth, helping mothers with positioning and latch, rooming-in, feeding on demand, and not giving pacifiers or prelacteal feeds. Knowing these steps helps you advocate for them in your clinical environment.