Page 14 of 21
PE8.1-5 | Complementary Feeding Practice — SDL Guide
Learning Objectives
- Define complementary feeding and explain why it must begin at exactly 6 months
- Apply the WHO IYCF complementary feeding attributes (timely, adequate, safe, appropriate) to practical feeding decisions
- Enumerate common Indian complementary foods by food group and identify strategies to improve energy density and dietary diversity
- Elicit a structured complementary feeding history from a caregiver, identifying red flags for inadequate feeding
- Counsel a mother on complementary feeding best practices using structured, culturally sensitive messages
INSTRUCTIONS
Complementary feeding is the clinical skill that bridges exclusive breastfeeding and family foods — a transition that begins at exactly six months and spans the most rapid phase of post-natal growth and brain development. Getting this transition right is consequential: early introduction (before 6 months) increases infection and allergy risk before gut maturity; late introduction (after 6–8 months) causes energy and iron-zinc deficiency at the very moment these demands are highest; poor-quality complementary foods — the thin gruels and watered-down porridges that are the default in many Indian households — cause stunting and wasting even in breastfed infants. This module builds your complementary feeding skill set: understanding the governing principles, knowing what to feed when, taking a structured feeding history, and counselling effectively. These skills are used at every 6-month and subsequent well-baby visit, and in every assessment of a child with growth faltering or malnutrition.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 7 — Infant Feeding (textbook)
- WHO/UNICEF Global Strategy for Infant and Young Child Feeding, 2003 (guideline)
- IAP Guidelines on Complementary Feeding, 2022 (guideline)
- WHO IYCF Indicators Manual, 2021 (food group and meal frequency definitions) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Eight-month-old Priya is brought to the outpatient clinic with poor weight gain. She weighed 6.8 kg at 6 months; today she weighs 6.9 kg — essentially no gain in two months. Her mother says she is breastfeeding well, 'as much as before.' On dietary history, the mother reveals she started giving Priya thin rice-water (kanji) twice a day at 6 months. The kanji is watery with no dal, no oil, no vegetables. Priya refuses more than 2–3 teaspoons. The mother is surprised: 'I thought breastfeeding plus rice water is enough — that's what my mother did for me.' What is wrong with Priya's complementary feeding, and how do you counsel her mother specifically and practically?
WHY THIS MATTERS
Complementary feeding errors are the single most common proximate cause of stunting and wasting in Indian children aged 6–24 months — the most nutritionally vulnerable window after birth. The consequences of getting it wrong are not just short-term (growth faltering, anaemia, infection) but lifelong: stunting in the first two years is largely irreversible, is associated with reduced adult height, lower educational attainment, reduced earning capacity, and — crucially — with stunted mothers delivering low-birth-weight infants who begin the cycle again. The NFHS-5 data are unambiguous: only 11.3% of Indian children 6–23 months achieve minimum dietary diversity and only 42.7% receive the minimum meal frequency. In this context, every well-child contact between 6 and 24 months is an opportunity to assess and correct complementary feeding — and every graduating doctor should be able to take a feeding history, identify the errors, and deliver targeted counselling. This is not abstract public health — it is a bedside skill you will use at every paediatric outpatient clinic.
RECALL
From the IYCF module: complementary feeding is IYCF Practice 3 — starting solid/semi-solid/liquid foods at 6 months alongside continued breastfeeding. From the breastfeeding physiology module: breast milk contributes 50–70% of energy at 6–12 months but cannot alone meet the infant's iron and zinc requirements after 6 months — breast milk iron, while highly bioavailable, is insufficient in volume. From community medicine and NHM: ICDS Anganwadi Workers and ASHA workers are the frontline counsellors for complementary feeding in India — knowing what they teach (and where the gaps are) helps you calibrate your clinical messages. From previous clinical postings: wasting (weight-for-height <-2 SD) and stunting (height-for-age <-2 SD) are the two key growth parameters affected by complementary feeding quality. Hold these — they are the clinical stakes of this skill module.
Clinical Indication and Relevance of Complementary Feeding
Complementary feeding is indicated at exactly 6 months of age (26 completed weeks; corrected age for preterm infants). The clinical rationale rests on three converging lines of evidence: nutritional need, gut maturity, and neurodevelopmental readiness. Understanding all three is essential for counselling — a mother who understands why 6 months is the threshold is far more likely to adhere than one who is simply told 'the rules.'
Nutritional indication — the energy and iron gap: Breast milk alone provides sufficient energy for full-term infants up to 6 months. After 6 months, the rapidly growing infant's energy requirements begin to exceed what breast milk can supply at realistic feeding frequencies. More critically, breast milk iron — while 50–70% bioavailable — is present in concentration of only 0.3 mg/L; by 6 months, the infant has depleted foetal iron stores (laid down in the third trimester of pregnancy) and requires dietary iron to support haemoglobin synthesis for the expanding red cell mass. An infant exclusively breastfed beyond 6 months without iron-rich complementary foods will develop iron-deficiency anaemia. Zinc follows a similar pattern. The first complementary foods therefore need to specifically target these deficits — iron-rich foods (meat, egg, iron-fortified cereals, dal) and zinc-containing foods (meat, legumes) take priority.
Gut maturity — the 6-month readiness: Before 6 months, the infant gut has increased intestinal permeability ('leaky gut') and insufficient digestive enzyme maturity (amylase, proteases) to handle solid foods safely. Early introduction of solids increases the risk of food sensitisation and allergy because intact food antigens cross the immature gut epithelium more readily. After 6 months, gut-associated lymphoid tissue (GALT) matures, intestinal permeability decreases, and digestive enzyme capacity increases, making the gut ready for a wider range of foods.
Neurodevelopmental readiness — the 6-month window: The infant at approximately 6 months has developed the neuromuscular capacity to accept and process semisolid foods: ability to sit with support (trunk stability), disappearance of the extrusion/tongue-thrust reflex (which previously pushed any solid objects out of the mouth), development of the gag reflex suppression sufficient for semi-solids, and beginning of voluntary hand-to-mouth movements. These milestones coincide with the 6-month biological window.
Why not before 6 months? Starting before 6 months (even at 4–5 months) is associated with: increased gut permeability and allergy risk, displacement of breast milk leading to reduced suckling and supply, and premature exposure to foods before digestive readiness. Why not after 6–7 months? Delayed introduction beyond 6–8 months causes energy and iron deficiency, increases wasting risk, and misses the critical texture-acceptance window — infants introduced to lumpy textures only after 9–10 months are significantly more likely to develop feeding difficulties and food refusal.
WHO IYCF Attributes of Complementary Feeding
Principles and Governing Attributes of Complementary Feeding
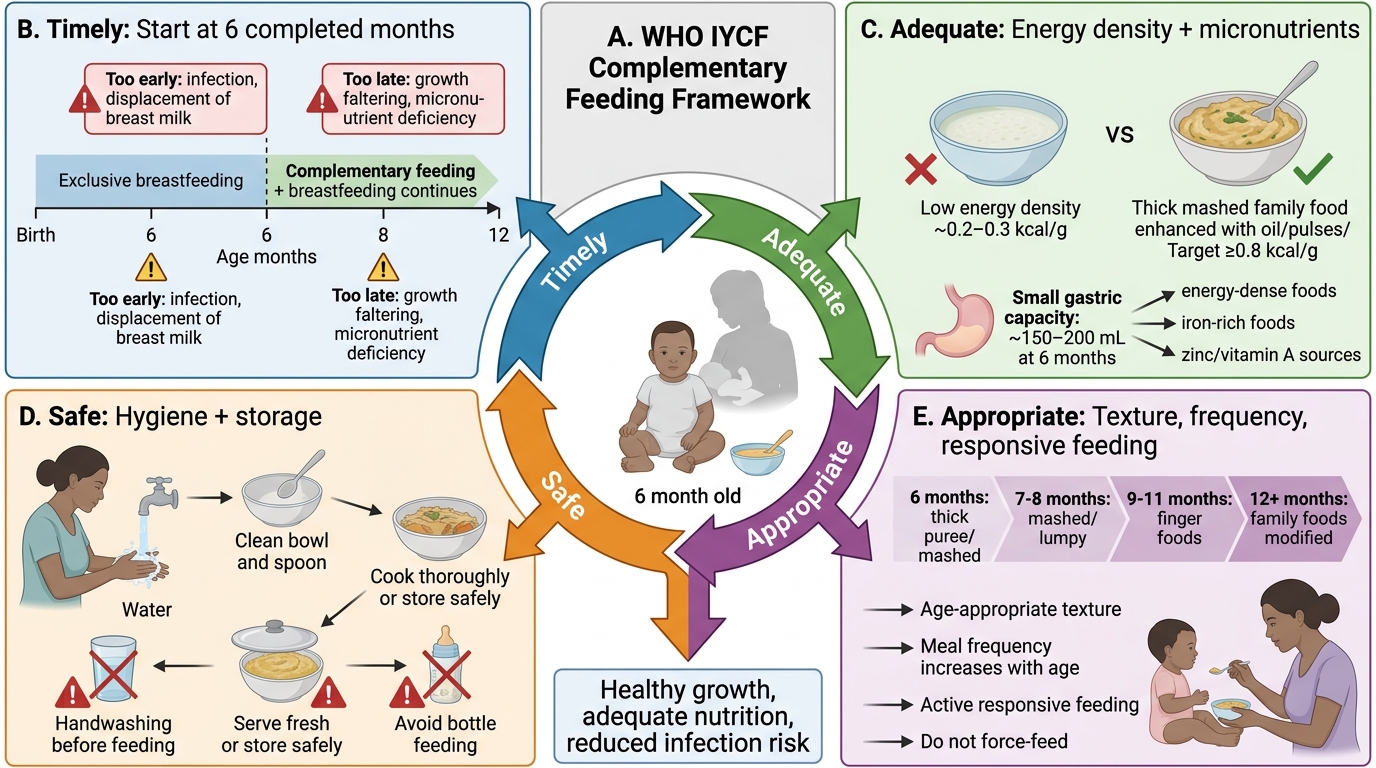
The WHO/IAP IYCF framework defines optimal complementary feeding through four governing attributes. These attributes are not aspirational ideals — they are measurable, teachable, and the basis of structured counselling. A complementary feeding practice that violates any one of these attributes causes harm, even if the others are correct.
1. Timely: Complementary feeding must start at 6 months — not before (see above), not delayed beyond 6–8 months. 'Timely' is the single threshold that anchors all other guidance.
2. Adequate: The foods given must meet the infant's energy and micronutrient needs in appropriate amounts. Two sub-components are critical:
Energy density: Infants have small gastric capacity (~150–200 mL at 6 months, rising to ~300 mL by 12 months). They can only eat small volumes per feed. Therefore, the energy density of complementary foods must be high enough to deliver adequate calories in a small volume. WHO recommends a minimum energy density of approximately 0.8 kcal/g for complementary foods in developing-country contexts. A thin rice-water (kanji) has approximately 0.2–0.3 kcal/g — one-quarter of the required density; an infant eating 100 g of kanji gets only 20–30 kcal, whereas the same volume of well-cooked khichdi with oil gets 80–100 kcal. Adding oil (1–2 teaspoons of cooking oil or ghee per feed), thick consistency (not watered-down), and energy-dense foods (legumes, egg, meat) is the primary strategy to increase energy density.
Micronutrient content: Diversity is the practical proxy for micronutrient adequacy. The WHO IYCF minimum dietary diversity indicator requires foods from ≥4 of 8 food groups in 24 hours. The 8 groups are: (1) breast milk; (2) grains/roots/tubers; (3) legumes/nuts; (4) dairy (other than breast milk); (5) flesh foods (meat, fish, chicken); (6) eggs; (7) Vitamin A-rich fruits/vegetables; (8) other fruits/vegetables. A child eating only rice and thin dal meets only 2 groups (grains + legumes) — dietary diversity of 2, well below the ≥4 threshold. Iron-rich flesh foods (especially egg and fish in Indian diets) are the highest-priority food group to add after grains/legumes.
3. Safe: Complementary foods must be prepared and stored safely to prevent diarrhoeal illness. Key hygiene messages: wash hands with soap before food preparation and feeding; use clean utensils; prepare food fresh (within 2 hours of serving in hot weather); store remaining food in a covered container in a cool place; do not feed from a bottle (bottle teats are difficult to clean and harbour pathogens — use a cup and spoon); avoid street food and packaged snacks with high sugar/salt content for children under 2 years.
4. Appropriate: Appropriateness encompasses consistency, frequency, volume, and responsiveness:
Texture/consistency progression: Begin with smooth, well-cooked, finely mashed or puréed foods at 6 months; progress to soft lumpy mashed foods at 7–8 months (when lateral tongue movement develops); soft pieces and finger foods at 9–11 months (when pincer grasp develops, around 8–9 months); and soft family foods by 12 months. Never give hard foods (raw carrot, whole grapes, whole nuts) that are choking hazards before adequate chewing capacity develops.
Meal frequency (WHO standard):
• Breastfed infants 6–8 months: 2 meals per day (+ breast milk on demand)
• Breastfed infants 9–23 months: 3 meals per day (+ 1–2 snacks; breast milk on demand)
• Non-breastfed infants 6–23 months: 4 meals per day (+ 1–2 snacks)
Responsive feeding: Feed slowly and patiently; encourage but do not force; if the child refuses, try again later or with a different texture; maintain eye contact and interaction during feeding; make feeding a positive, distraction-free experience.
SELF-CHECK
A 9-month-old breastfed infant is being given only thin rice porridge twice a day. His mother says she cannot afford meat or eggs. Which TWO changes would most effectively improve the energy and nutritional adequacy of his complementary feeding at low cost?
A. Add 1–2 tsp of cooking oil to the porridge and introduce mashed dal or legumes
B. Stop breastfeeding and switch to full-cream cow's milk three times daily
C. Give vitamin supplements and continue thin porridge twice daily
D. Introduce finger biscuits and powdered formula to increase calorie intake
Reveal Answer
Answer: A. Add 1–2 tsp of cooking oil to the porridge and introduce mashed dal or legumes
The two highest-impact, lowest-cost changes are: (1) adding cooking oil or ghee to increase the energy density of the porridge from ~0.2 kcal/g to ~0.6–0.8 kcal/g, and (2) adding mashed dal (lentils/legumes) to provide protein, zinc, and iron — locally available, inexpensive, and culturally familiar. Stopping breastfeeding at 9 months is harmful — breast milk continues to provide significant nutrition and immunity; it should not be replaced with cow's milk in this age group. Vitamin supplements without dietary change do not address energy or protein deficiency. Finger biscuits and powdered formula are expensive and nutritionally inferior to home-prepared foods with appropriate energy density. The meal frequency for a breastfed 9-month-old should also be increased to 3 meals per day.
Common Complementary Foods and Dietary Diversity
Complementary feeding guidance must be culturally grounded and economically realistic. Recommending foods that are nutritionally ideal but unavailable, unaffordable, or culturally unacceptable guarantees non-compliance. India's diverse culinary landscape, combined with a predominantly vegetarian tradition in many communities, requires food recommendations that are practical, locally available, and adapted to what families actually cook. The following covers the main food categories, their nutritional contributions, and specific strategies for the Indian context.
Provided image
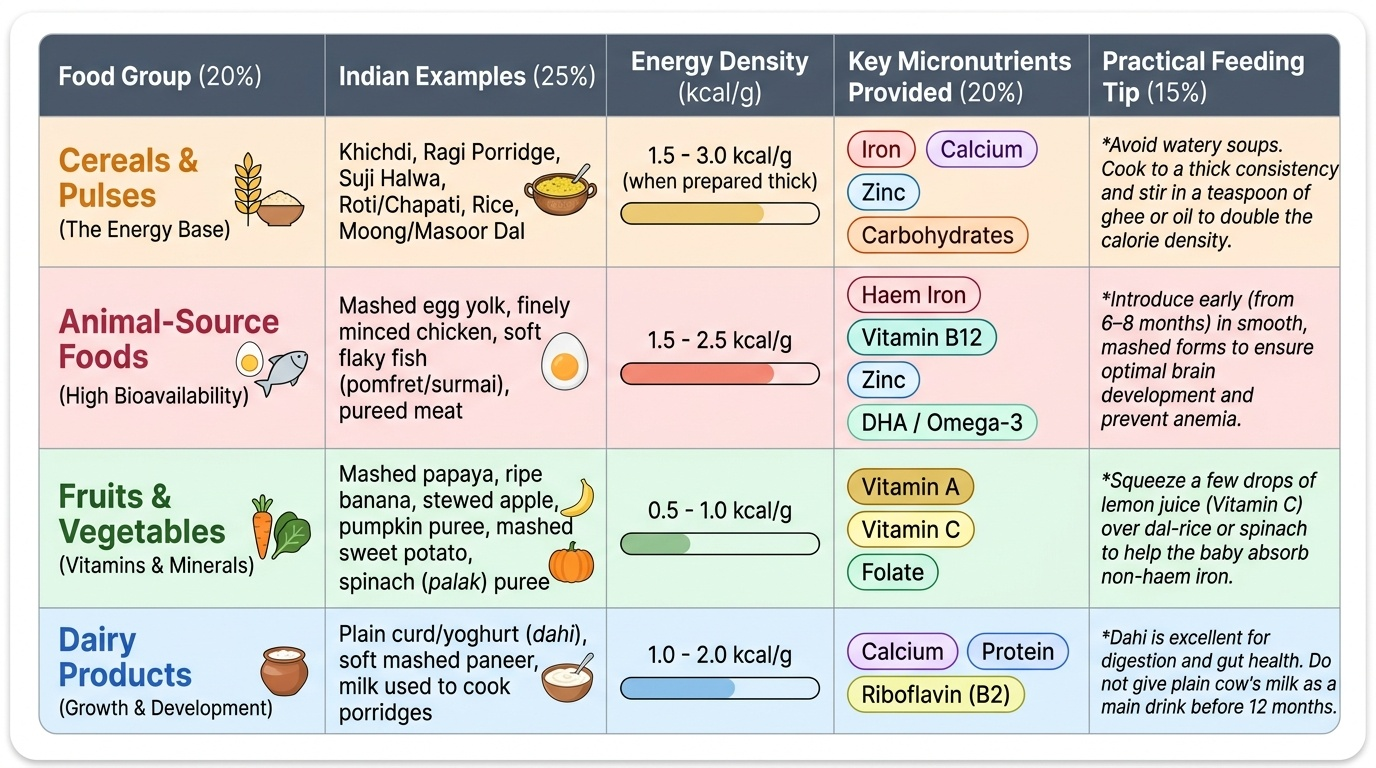
Grains, roots and tubers (energy base): Rice, wheat (roti/chapati), ragi, jowar, bajra, suji (semolina), potato, yam. These provide the primary energy and carbohydrate base of the diet. Cereal-based porridges (khichdi, ragi porridge, suji halwa) are the most common first foods. Their energy density must be improved by cooking to thick consistency and adding fat. Ragi (finger millet) is particularly valuable in South India — it is calcium-rich (344 mg/100 g), iron-containing, and can be made into a thick porridge or sprout-flour.
Legumes and pulses (protein, iron, zinc): Dal (lentils, moong, masoor, toor), rajma, chana, soybean. These are the primary protein and non-haem iron source in vegetarian diets. Non-haem iron absorption is enhanced by Vitamin C-containing foods (tomato, lemon juice, amla) served with the same meal. Preparing thick dal and mixing with rice/khichdi is an ideal high-protein, energy-dense combination.
Animal-source foods — highest priority for micronutrients: Egg, fish, chicken, meat. These are the most bioavailable sources of haem iron, zinc, B12, and DHA in complementary diets. A single egg provides 6 g protein, haem iron, zinc, and Vitamin B12. IAP (2022) recommends introducing eggs at 6 months; evidence does not support delaying egg introduction for allergy prevention in non-high-risk infants. Fish provides DHA essential for brain development. Chicken and meat provide haem iron with high bioavailability. In communities that do not eat meat/egg, achieving adequate iron and zinc through plant foods alone requires careful dietary planning and is more difficult.
Vitamin A-rich fruits and vegetables: Mango, papaya, carrot, sweet potato, pumpkin, green leafy vegetables (spinach, palak, methi, drumstick leaves). These provide Vitamin A (as β-carotene), folate, iron, and fibre. Green leafy vegetables are iron-containing but absorption is reduced by phytates and oxalates — combining with Vitamin C foods improves uptake.
Dairy (other than breast milk): Full-fat curd (dahi), paneer, ghee. Cow's milk as a main drink remains contraindicated under 12 months (see breastfeeding physiology module), but small amounts of full-fat dairy as an ingredient in complementary foods (curd mixed with rice, paneer in khichdi) are acceptable from 6 months.
Foods to avoid (under 2 years):
• Salt (avoid added salt; infant kidneys cannot handle high sodium loads; taste preferences established early)
• Sugar and jaggery (avoid in excess; promotes dental caries, displaces nutrient-dense foods)
• Honey (absolute — infant botulism risk from Clostridium botulinum spores)
• Ultra-processed packaged snacks, biscuits, chips — high in salt/sugar/trans fats, low nutrient density
• Unpasteurised animal milks
• Choking hazards: whole grapes, whole nuts, raw hard vegetables before adequate chewing development
| Food group | Indian examples | Approx. energy density | Key nutrients |
|---|---|---|---|
| Grains/cereals | Rice, ragi, khichdi, roti | 0.3–0.9 kcal/g (cooked) | Energy, B vitamins |
| Legumes/pulses | Dal, moong, rajma | 0.5–1.0 kcal/g (cooked) | Protein, iron (non-haem), zinc |
| Eggs | Whole egg, scrambled | ~1.5 kcal/g | Protein, haem iron, B12, DHA |
| Fish/chicken/meat | Fish, chicken, mutton | ~1.5–2.0 kcal/g | Haem iron, zinc, B12, DHA |
| Vitamin A veg/fruit | Carrot, papaya, mango | 0.3–0.6 kcal/g | β-carotene, folate, Vit C |
| Full-fat dairy (as ingredient) | Curd, paneer, ghee | 1.0–7.0 kcal/g | Calcium, protein, fat |
CLINICAL PEARL
The energy density trap — 'kanji problem': In large parts of India, the default first complementary food is a thin cereal gruel — kanji (rice water), thin ragi porridge, or diluted suji. These have an energy density of 0.2–0.3 kcal/g — less than a quarter of the WHO minimum. A 9-month-old with a gastric capacity of ~250 mL, fed kanji twice a day, may be receiving only 100–150 kcal from complementary foods, while her energy requirement is ~600–700 kcal/day (partially met by breast milk at ~400–500 kcal, leaving a gap). The fix is startlingly simple and cheap: thicken the porridge (use less water), add 1–2 teaspoons of oil or ghee, and add mashed dal. These changes cost nothing in a household already using these ingredients and can triple the energy density. When counselling, demonstrate the difference visually: 'a thin porridge that pours like water versus a thick one that drops off the spoon.'