Page 15 of 21
PE8.1-5 | Complementary Feeding Practice — SDL Guide (Part 2)
Eliciting a Complementary Feeding History
Taking a complementary feeding history is a clinical skill that requires structured inquiry across six domains. A vague 'what does the baby eat?' question typically elicits 'normal food' — which is not clinically useful. You must ask specifically, with probing questions designed to expose the most common errors in complementary feeding practice. This structured approach takes 5–7 minutes and is applicable at every well-child visit from 6 to 24 months, and at every assessment of a child with growth faltering, anaemia, or malnutrition.
The six-domain complementary feeding history:
1. Age of introduction: 'At what age did you first give your baby any food other than breast milk?' — This establishes whether introduction was timely (at 6 months), early (<6 months), or late (>6–8 months).
2. Current diet (24-hour recall): 'Can you tell me everything your baby ate and drank yesterday — starting from the first morning feed?' This is the most informative question. For each item, clarify: what it was, how it was prepared (thick or thin), how much (in household measures), and how often it was given. Count the food groups to calculate dietary diversity.
3. Meal frequency: 'How many times a day do you give your baby solid or semi-solid food?' Compare with WHO standards (breastfed 6–8 mo: 2×/day; 9–23 mo: 3×/day). A breastfed 9-month-old receiving solid food only once a day has inadequate meal frequency regardless of food quality.
4. Texture and consistency: 'Is the food smooth, lumpy, or in small pieces? Does the baby chew or just swallow?' Match texture to developmental stage. A 10-month-old still receiving only smooth purée may miss the texture-acceptance window. An 8-month-old receiving unmashed pieces of hard food is at choking risk.
5. Feeding behaviour and appetite: 'How does the baby behave at feeds? Does she open her mouth eagerly, or turn away? How long does each feed take? Does she finish what you give her?' Persistent refusal, very long feeding times, or total volume <50% of expected may indicate feeding aversion, illness, or inadequate palatability.
6. Feeding practices during illness: 'When the baby had diarrhoea/fever last month, what did you change about the feeding?' Identifying feeding withdrawal during illness is a key red flag — food restriction during illness worsens nutritional status and delays recovery.
Red flags in the complementary feeding history:
• Age of introduction <4 months or >7–8 months
• Only 1–2 food groups in 24-hour recall (no animal source, no fruits/vegetables)
• Meal frequency below WHO standards for age
• Thin gruel/watery consistency only (energy density concern)
• Feeding withdrawal during illness
• Bottle feeding (infection and overfeeding risk)
• Honey given (botulism risk)
• Added salt or excessive sugar in infant foods
Counselling Mothers on Complementary Feeding Best Practices
Effective complementary feeding counselling is structured, specific, non-judgmental, and action-oriented. The goal is not to overwhelm a mother with all possible messages simultaneously but to identify the two or three most important changes for her specific child and deliver them with clarity and practical demonstration. The following provides the framework for structured CF counselling, aligned with IAP and WHO IYCF guidance.
The five-message CF counselling framework:
Message 1 — When to start: 'Start solid foods at exactly 6 months — not earlier, not later. Before 6 months, the baby's gut is not ready. After 6–8 months, the baby needs more energy than breast milk alone can give.' For a mother with a 5-month-old asking when to start: give the exact date based on the child's birth date. For a mother whose 8-month-old was never given solids: reassure that starting now is still beneficial, but emphasise urgency.
Message 2 — What to give (first foods and variety): 'Start with one new food at a time, wait 3 days before introducing the next — this lets you see if the baby tolerates it. First foods: soft, well-cooked rice or ragi or suji with dal mashed together, or mashed banana, or cooked carrot purée. Add an egg (boiled and mashed) from 6 months — it is inexpensive and very nutritious. After the first 2–3 weeks, add fish or chicken if your family eats these.' Demonstrate the consistency: 'thick enough to drop off the spoon, not pour like water.'
Message 3 — How much and how often: 'Start with 2–3 teaspoons twice a day at 6 months. Gradually increase over the next few weeks to 2–3 tablespoons, then to half a small bowl. By 9 months, give solid food three times a day. By 12 months, the baby should be eating from the family pot at every family mealtime.' Provide a visual: use local measures (katori/bowl sizes) rather than grams.
Message 4 — Improve energy density — the key practical message for most Indian families: 'Add 1–2 teaspoons of cooking oil or ghee to the porridge or khichdi at each meal. This doubles the energy the baby gets from the same volume of food. You do not need to buy expensive foods — well-cooked khichdi (rice + dal + a little oil) is one of the best first foods.' This message directly addresses the kanji-problem and is immediately actionable for nearly every Indian family.
Message 5 — Continue breastfeeding and feed responsively: 'Keep breastfeeding as much as the baby wants — breast milk is still very important. Do not replace breastfeeds with solid food. Feed the baby when she shows hunger cues: reaching for food, mouth opening. Do not force-feed. If she refuses, wait 30 minutes and try again. Make feeding a quiet, calm, face-to-face experience — not while watching TV or while you are on the phone.' This message addresses the common misconception that starting solids means stopping breastfeeding, and introduces responsive feeding as a principle.
Counselling pitfalls to avoid:
• Using technical language (energy density, dietary diversity) without translating to practical actions
• Recommending expensive foods (commercial baby food, formula) when cheap home-prepared foods are equally adequate
• Giving so many messages that none are retained — prioritise the 2–3 most relevant to the specific mother's current practice
• Judging or criticising the current practice — acknowledge effort, then redirect: 'You are doing well with breastfeeding. Let's also add one more thing that will help Priya grow even better.'
• Forgetting to ask about the family's food preferences and budget constraints before recommending specific foods
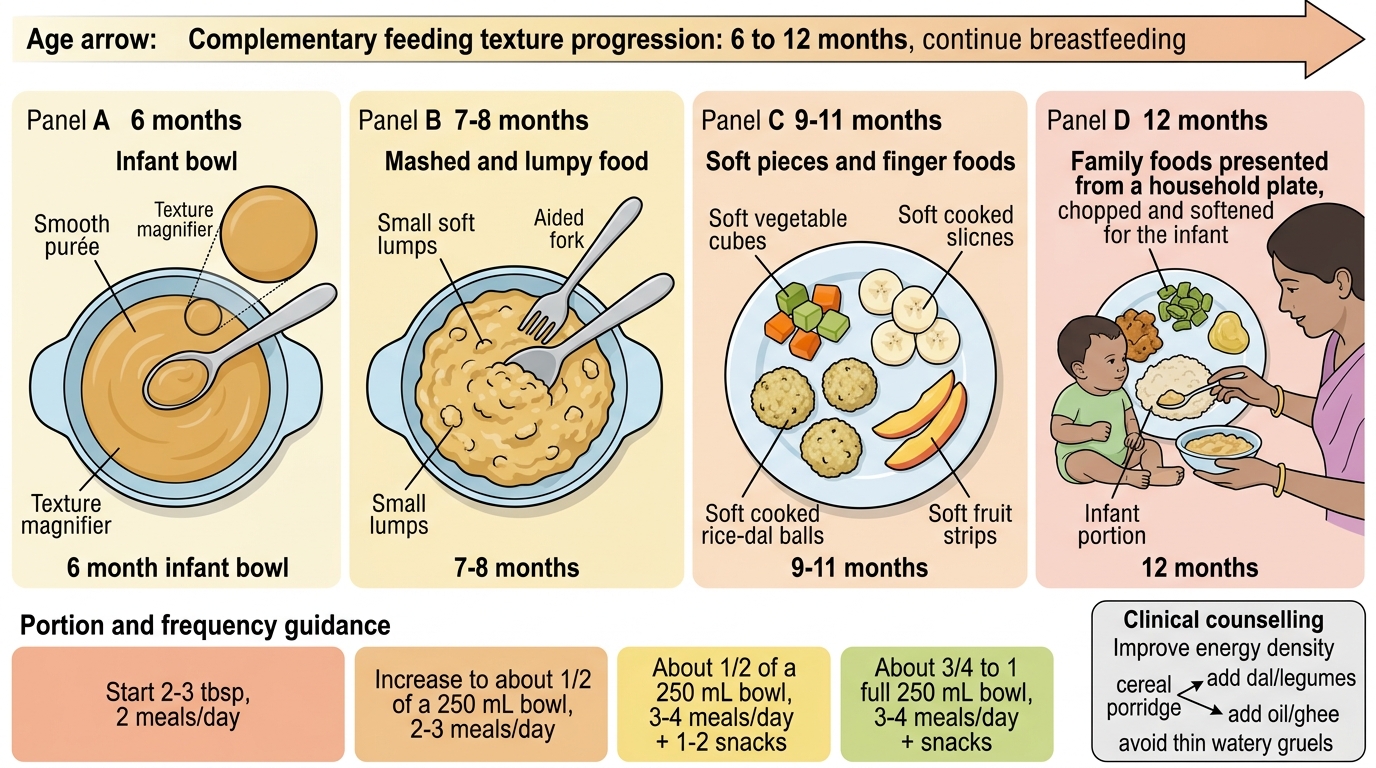
Texture Progression in Complementary Feeding
Self-Assessment
Complementary feeding practice spans definition (PE8.1), governing principles (PE8.2), food knowledge (PE8.3), history-taking (PE8.4), and counselling (PE8.5) — a skill arc that runs from understanding to application. The clinical heart of this arc is the ability to sit with a caregiver, take a structured 24-hour dietary recall that counts food groups and estimates meal frequency, identify the specific errors, and translate them into two or three targeted, practical, affordable actions. The governing framework — timely at 6 months, adequate energy density (≥0.8 kcal/g), safe preparation, appropriate texture and meal frequency — provides the structure for both assessment and counselling. The most impactful single intervention in most Indian households is improving the energy density of cereal porridge by adding fat and legumes — simple, cheap, and immediately actionable. The worst foods to recommend are honey (botulism risk), added salt, thin watery gruels, and ultra-processed snacks. Test yourself on the key parameters with the questions below.
SELF-CHECK
A 7-month-old breastfed infant has been given complementary foods for 4 weeks. On dietary recall, the mother reports giving mashed banana and thin rice water once a day. What is the primary deficiency in this feeding practice?
A. Age of introduction is too early — solid foods should not begin until 8 months
B. Meal frequency is inadequate (should be 2×/day at 7 months) and energy density is low (thin rice water ≈ 0.2 kcal/g)
C. The food groups are adequate — banana and rice together provide all necessary nutrients
D. Breastfeeding should be stopped now that solids have been introduced
Reveal Answer
Answer: B. Meal frequency is inadequate (should be 2×/day at 7 months) and energy density is low (thin rice water ≈ 0.2 kcal/g)
At 7 months (breastfed), the WHO recommends at least 2 meals of solid food per day; this infant is receiving only 1. Additionally, thin rice water has an energy density of approximately 0.2 kcal/g — well below the WHO minimum of ~0.8 kcal/g. While banana provides energy and potassium, the diet lacks protein (no legumes or animal-source food), iron (no iron-rich foods), and micronutrient diversity. Age of introduction at 6 months is correct (not too early). Banana and rice together do not provide adequate protein, iron, or dietary diversity — they count as only 2 food groups (grain + fruit) against the ≥4 required for minimum dietary diversity. Breastfeeding must continue alongside complementary foods until 2 years.