Page 8 of 21
PE7.6 | Infant and Young Child Feeding Principles — SDL Guide
Learning Objectives
- Describe the WHO Global Strategy for Infant and Young Child Feeding and its five core practice recommendations
- Define each IYCF practice precisely, including thresholds for exclusive breastfeeding duration and complementary feeding initiation
- Explain IYCF recommendations in special circumstances: preterm infants, HIV-exposed infants, and working mothers
- Identify India's key IYCF delivery platforms (ICDS, BFHI, POSHAN Abhiyaan) and interpret the WHO standard IYCF indicator set
- Correlate suboptimal IYCF practices with their consequences for child survival, growth, and development in the Indian context
INSTRUCTIONS
Infant and young child feeding (IYCF) practices are among the most powerful determinants of child survival, growth, and development in the first two years of life — a period the WHO designates the 'window of opportunity' for nutrition. In India, where under-five malnutrition (stunting 35.5%, wasting 19.3% per NFHS-5) remains a major public-health challenge, suboptimal IYCF practices — particularly low exclusive breastfeeding rates and inappropriate complementary feeding — are key modifiable risk factors. As a graduating doctor you will encounter IYCF at every level: counselling a postnatal mother on the maternity ward, advising on complementary feeding at the six-month well-baby visit, managing a malnourished toddler in the paediatric ward, and supporting ASHA workers in community outreach. This module gives you the conceptual framework — the WHO five practices — and the programmatic context to operationalise it in India.
References
- WHO/UNICEF Global Strategy for Infant and Young Child Feeding, 2003 (guideline)
- Ghai Essential Pediatrics, 9th ed., Ch. 7 — Infant Feeding (textbook)
- IAP Policy on Infant and Young Child Feeding, 2023 (guideline)
- NFHS-5 (2019–21): India IYCF Indicators, Ministry of Health & Family Welfare (report)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At a community health camp in a rural block, an ASHA worker brings you her register. Of 12 infants aged 0–5 months seen this week, she has noted: 7 are receiving cow's milk or formula alongside breast milk; 3 were given janam ghuti (a traditional herbal preparation) on the first day; 2 are already receiving rice porridge at 4 months. Only 2 are exclusively breastfed. The block nutritionist says 'mothers know they should breastfeed, but they don't know what that actually means.' What framework guides your response — and what specific, actionable messages would you deliver to correct each practice?
WHY THIS MATTERS
IYCF principles are not merely academic — they are the operational specification for preventing childhood malnutrition at the population level. The Lancet Nutrition Series estimates that optimal breastfeeding alone could prevent 13% of all under-five deaths globally; adding appropriate complementary feeding raises the preventable fraction substantially. In India, the consequences of suboptimal IYCF are starkly visible: early weaning contributes to wasting and stunting; premature introduction of complementary foods increases diarrhoea and infection risk before the gut immune system matures; cow's milk given before 12 months causes iron-deficiency anaemia and renal solute overload. For you as a clinician, knowing the IYCF framework precisely means you can give specific, evidence-based advice rather than vague recommendations — you can explain not just 'breastfeed' but exactly when, how, for how long, and what to do when circumstances complicate the ideal.
RECALL
From the previous module on breastfeeding physiology: exclusive breastfeeding requires that no additional fluid or food be given — not even water. Prolactin-driven milk supply is demand-dependent; supplementation reduces suckling frequency and undermines supply. Colostrum is the immunologically critical first milk; discarding it is harmful. From community medicine (CM): the ICDS (Integrated Child Development Services) provides supplementary nutrition and health services through Anganwadi Centres; ASHA workers are community-level health volunteers conducting home visits and counselling. From the National Immunization Schedule: infants are seen at 6, 10, 14 weeks and again at 9–12 months — each contact is an IYCF counselling opportunity. Hold these links — IYCF is both a clinical recommendation and a programme.
Orientation: IYCF as a Global and National Priority
The WHO Global Strategy for Infant and Young Child Feeding (2003), developed jointly with UNICEF, established the evidence-based framework that all member states, including India, have adopted as policy. The strategy arose from recognition that malnutrition — not infectious disease — is the underlying cause of more than half of all child deaths under age five, and that the period from birth to 24 months represents the most critical window for nutritional intervention, with consequences that are partially irreversible if missed. 'Infant' refers to the child from birth to 12 months; 'young child' refers to 12–36 months; together, IYCF covers the entire period when feeding practices most powerfully shape lifetime health outcomes.
Provided image
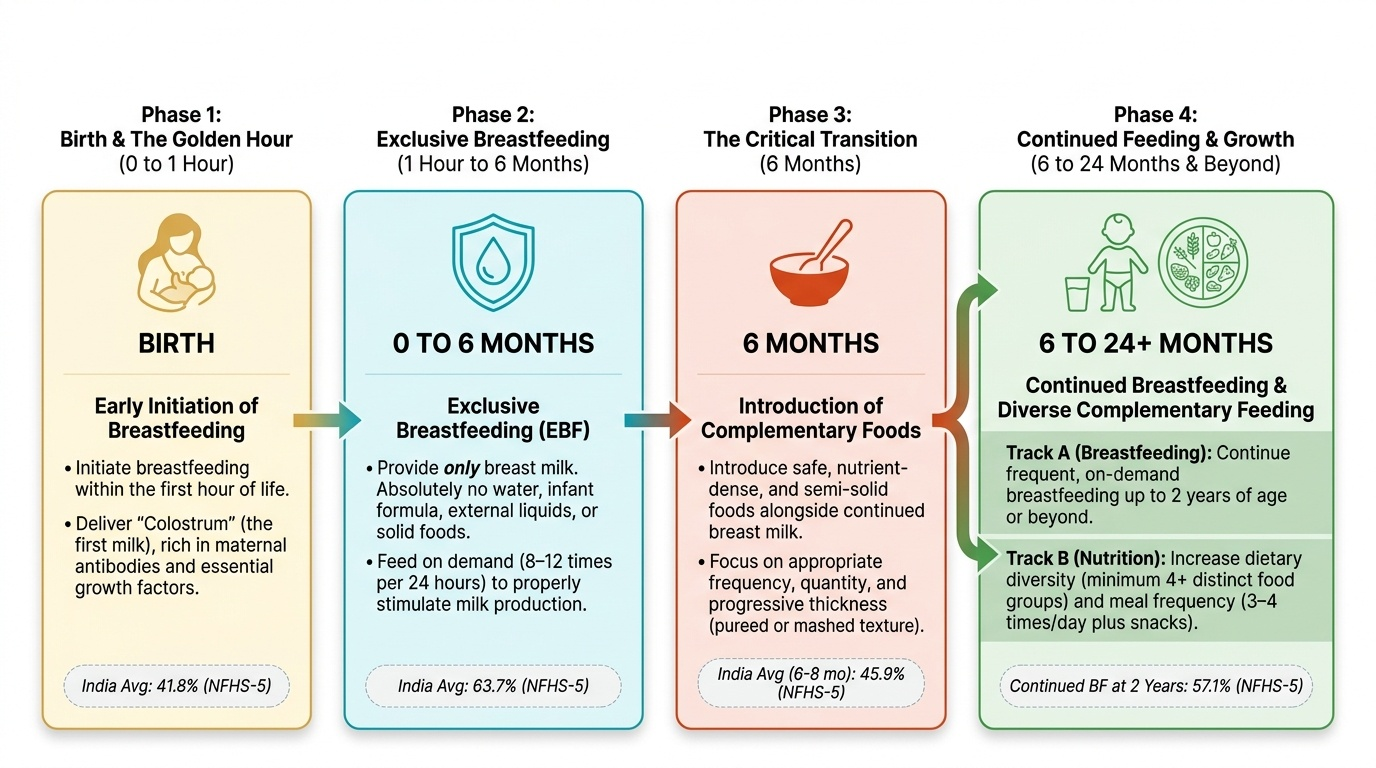
In India, the burden of suboptimal IYCF is quantified through the National Family Health Survey (NFHS-5, 2019–21). Key indicators reveal persistent gaps:
• Early initiation of breastfeeding (within 1 hour of birth): 41.8% — meaning more than half of newborns miss the first-hour colostrum window.
• Exclusive breastfeeding under 6 months: 63.7% — substantial improvement from NFHS-4 (54.9%) but still below the 80% target.
• Timely introduction of complementary foods (6–8 months): 45.9% — suggesting many infants receive foods too early or too late.
• Continued breastfeeding at 2 years: 57.1%.
These figures reflect enormous heterogeneity across states (Kerala >80% exclusive BF; some BIMARU states <50%), urban-rural divides, and maternal education gradients. The POSHAN Abhiyaan (National Nutrition Mission), launched in 2018, targets improvement of IYCF indicators as one of its six priority areas, delivered through convergence of ICDS, NHM, and food security programmes.
Understanding this epidemiological landscape is the first step: when you counsel a mother, you are not correcting individual behaviour in isolation — you are working against deeply embedded cultural practices that the IYCF programme aims to shift at scale.
The Five Core IYCF Practices
The WHO/IAP IYCF framework is built around five core, sequential, inter-dependent practices. Each is precisely defined — the specific thresholds matter clinically and programmatically, and common errors (confusing months or adding qualifiers) undermine both individual counselling and programme measurement.
Practice 1 — Early initiation of breastfeeding: The first breastfeed should occur within one hour of birth (WHO/IAP recommendation). This practice delivers: the first dose of colostrum (maximum immunological payload); skin-to-skin contact that stabilises neonatal temperature, blood glucose, and heart rate; establishment of the prolactin reflex at its most responsive window; and colonisation of the neonatal gut with maternal microbiota before environmental organisms. The BFHI Step 4 operationalises this: 'Help mothers initiate breastfeeding within a half-hour of birth' (original wording) — current WHO guidance specifies one hour. Caesarean section is not a contraindication; skin-to-skin and breastfeeding initiation in the recovery room within the first hour is feasible and recommended.
Practice 2 — Exclusive breastfeeding for the first six months: Exclusive breastfeeding (EBF) is defined as giving only breast milk — no water, no juice, no other fluids, no solids, no other milks — for the full first 6 months of life. The only acceptable additions are oral rehydration salts, drops, and syrups (vitamins, minerals, medicines) when medically indicated. This definition is absolute; even giving water ('the baby is thirsty in summer') violates exclusivity. Water given before 6 months displaces breast milk, introduces infection risk, and reduces suckling frequency. The 6-month threshold is based on evidence that: (a) breast milk alone fully meets nutritional and immunological needs until 6 months in full-term infants; (b) the gut is not mature enough to handle solids before 6 months (intestinal permeability, inadequate digestive enzyme capacity); and (c) early introduction of solids (before 6 months) increases risk of infection, allergy, and later obesity.
Practice 3 — Timely introduction of complementary foods at 6 months: Starting at exactly 6 months (corrected age for preterm infants), complementary foods — solid, semi-solid, or liquid foods given alongside breast milk — should be introduced. These foods should be: adequate in energy density and micronutrient content; given in appropriate texture and consistency for the infant's developmental stage; introduced with increasing frequency as the child grows; and prepared and stored with hygiene. Critically, breastfeeding continues alongside complementary foods — complementary feeding does NOT mean weaning. This practice is detailed further in the PE8 complementary feeding module.
Practice 4 — Continued breastfeeding up to two years or beyond: Breast milk continues to contribute 50–70% of the energy intake of infants aged 6–12 months, and approximately one-third of energy intake at 12–24 months. In the second year, breast milk remains a valuable source of protein, fat, calcium, and immunological factors, and the act of breastfeeding continues to provide maternal-infant bonding and emotional security. The WHO/IAP recommendation is breastfeeding to 2 years or beyond — not merely to 1 year. Premature cessation at 12 months is a common practice in India and is not evidence-based.
Practice 5 — Responsive and appropriate feeding during illness: The feeding relationship between caregiver and child should be responsive — feeding on demand, watching for hunger and satiation cues, avoiding force-feeding, and maintaining a nurturing environment. During illness (diarrhoea, respiratory infections, fever), breastfeeding should be continued and increased (not stopped): breast milk provides hydration, passive immunity, and energy at a time when appetite for solids is reduced. Restricting feeds during illness ('giving the gut a rest') is a harmful cultural practice — it worsens dehydration, delays recovery, and reduces milk supply. After illness, catch-up feeding should be encouraged.
The five practices are interdependent: a failure at Practice 1 (delayed initiation) reduces colostrum delivery and impairs supply establishment; a failure at Practice 2 (early introduction of water or solids) reduces suckling and undermines Practice 4 (continued breastfeeding duration); a failure at Practice 3 (late or inappropriate complementary foods) causes malnutrition even in breastfed infants.
SELF-CHECK
A mother of a 4-month-old asks if she can give boiled water to her baby during a heatwave. The baby is being exclusively breastfed. What is the correct advice?
A. Allow water up to 60 mL/day as breast milk alone cannot hydrate in heat
B. Exclusive breastfeeding means NO water; breast milk is 88% water and fully adequate for hydration
C. Allow water only if the baby has more than 8 wet nappies per day
D. Water is safe after 3 months as the kidneys can handle the extra solute load
Reveal Answer
Answer: B. Exclusive breastfeeding means NO water; breast milk is 88% water and fully adequate for hydration
Exclusive breastfeeding (EBF) is defined as giving only breast milk — no water, no juice, no other fluids — for the full first 6 months. Breast milk is approximately 88% water and fully meets hydration needs even in hot climates, as demonstrated by studies in sub-Saharan Africa and South Asia. Giving water before 6 months displaces breast milk, reduces suckling frequency, impairs supply, introduces infection risk, and violates the definition of EBF. The appropriate response to infant heat stress is increased breastfeeding frequency, not water supplementation.
IYCF in Special Circumstances
The five IYCF practices are the ideal for term, healthy infants with healthy, well-nourished mothers. Clinical practice frequently involves circumstances that require adaptation — but the principles remain the same: breast milk is the optimal food for infants, and the bar for recommending against breastfeeding is high. The following situations are encountered in Indian paediatric practice and require specific IYCF guidance.
Preterm and low-birth-weight (LBW) infants: For preterm or LBW infants who cannot suckle directly, expressed breast milk should be provided by cup or nasogastric tube. Preterm mother's own milk has higher protein and sodium content than term milk, matched to the preterm infant's greater needs. For very-low-birth-weight (<1500 g) infants, human milk fortifiers may be added to meet caloric and protein needs for catch-up growth. Donor pasteurised human milk from a human milk bank (HMB) is the recommended alternative when the mother's own milk is insufficient. Formula should be a last resort. Breastfeeding should be initiated (or re-established via kangaroo mother care) as soon as the infant is stable.
HIV-exposed infants: In India, the National AIDS Control Organisation (NACO) guidelines recommend that HIV-positive mothers on antiretroviral therapy (ART) breastfeed exclusively for 6 months and continue breastfeeding up to 12 months. The rationale is that in India's context, the risks of not breastfeeding (diarrhoea, pneumonia, malnutrition) are greater than the residual transmission risk when the mother is on effective ART with a suppressed viral load. Replacement feeding (formula) is recommended only when it is AFASS — acceptable, feasible, affordable, sustainable, and safe — criteria that are rarely met at the community level in India. This guidance differs from high-income country recommendations where formula is safe and accessible.
Working mothers: Return to work is a major reason for premature weaning in India. Key strategies include: expression and storage of breast milk (expressed milk can be stored at room temperature for 4–6 hours, in a refrigerator for 3–5 days, or frozen for up to 6 months); reverse-cycle feeding (more frequent feeds when with the mother, stored milk during separation); advocacy for workplace crèches and breastfeeding breaks (the Maternity Benefit (Amendment) Act 2017 requires crèche facilities in workplaces with ≥50 employees). Educate mothers about expression technique before return to work.
Contraindications to breastfeeding (rare and specific): True contraindications are few: (a) infant with galactosaemia (rare metabolic disorder — cannot metabolise galactose in lactose); (b) active untreated pulmonary tuberculosis in the mother (sputum-positive) — breastfeeding is stopped until the mother is non-infectious; (c) maternal cytotoxic chemotherapy — contraindicated during treatment; (d) maternal use of certain medications (amiodarone, radioactive iodine — individual assessment). Maternal HIV is NOT an absolute contraindication in India (see above). Maternal hepatitis B is NOT a contraindication — the infant should receive hepatitis B vaccine and HBIG at birth per NIS. Mastitis, cracked nipples, and minor illness are NOT contraindications.
CLINICAL PEARL
The exclusive breastfeeding 'water trap' in summer: In India, the belief that breastfed babies need water during hot weather is one of the most common reasons for failure of exclusive breastfeeding. A well-meaning grandmother filling a 2-month-old's stomach with boiled water before each feed can destroy a mother's milk supply within weeks — the full stomach reduces suckling frequency, prolactin falls, and supply dwindles, 'confirming' the family's belief that the mother's milk was insufficient. When you encounter this practice, explain the physiology directly: 'Breast milk is 88% water. When the baby suckles more frequently in heat, the mother's body produces more watery foremilk — a beautifully automatic hydration mechanism. Adding water interferes with this system.'