Page 9 of 21
PE7.6 | Infant and Young Child Feeding Principles — SDL Guide (Part 2)
India's IYCF Delivery Platforms and Indicators
IYCF practices are not changed through individual clinical encounters alone — they require a systematic, population-level delivery infrastructure that reaches every mother, every village, and every birthing facility. India has invested substantially in building this infrastructure over five decades, from the launch of ICDS in 1975 through the 2018 POSHAN Abhiyaan — a layered system that places a trained community health worker within walking distance of virtually every household in the country. Understanding this infrastructure matters clinically in two ways. First, it tells you what exists: when you discharge a mother from the maternity ward, you are handing her to an ASHA worker and an Anganwadi Centre that should reinforce your counselling — knowing their mandate and limitations helps you calibrate your expectations. Second, it empowers you to advocate: when a facility practice (permitting formula samples, separating mother and baby) undermines IYCF, knowing BFHI standards and government policy gives you the language to push for change. A doctor who understands the delivery ecosystem is a more effective IYCF advocate than one who sees feeding counselling as a purely individual interaction.
Provided image
Key IYCF delivery platforms in India:
• ICDS (Integrated Child Development Services): India's flagship programme for child nutrition and development (launched 1975). Delivered through approximately 1.4 million Anganwadi Centres (AWCs), reaching children 0–6 years and pregnant/lactating women. Anganwadi Workers (AWWs) provide supplementary nutrition, growth monitoring, health and nutrition education including IYCF counselling, and immunisation support.
• ASHA (Accredited Social Health Activist): Community-level frontline health workers conducting home visits, especially around delivery and the postnatal period. ASHA workers are trained to counsel on early initiation, EBF, and complementary feeding initiation, and to refer high-risk cases.
• BFHI (Baby-Friendly Hospital Initiative): WHO/UNICEF programme certifying birthing facilities that implement the Ten Steps to Successful Breastfeeding. In India, operationalised through the Breastfeeding Promotion Network of India (BPNI) and Ministry of Health. BFHI hospitals prohibit distribution of formula company marketing materials and require trained staff for lactation support.
• POSHAN Abhiyaan (National Nutrition Mission, launched 2018): Targets reducing stunting, wasting, anaemia, and LBW; IYCF improvement is a core strategy. Includes community-based events (POSHAN Maah — September), real-time monitoring through the ICDS-CAS app, and convergence across ICDS, NHM, and food security schemes.
• Mother Absolute Affection (MAA) Programme: A nationwide programme specifically promoting breastfeeding; focuses on early initiation, EBF, and counselling at all levels of health facilities.
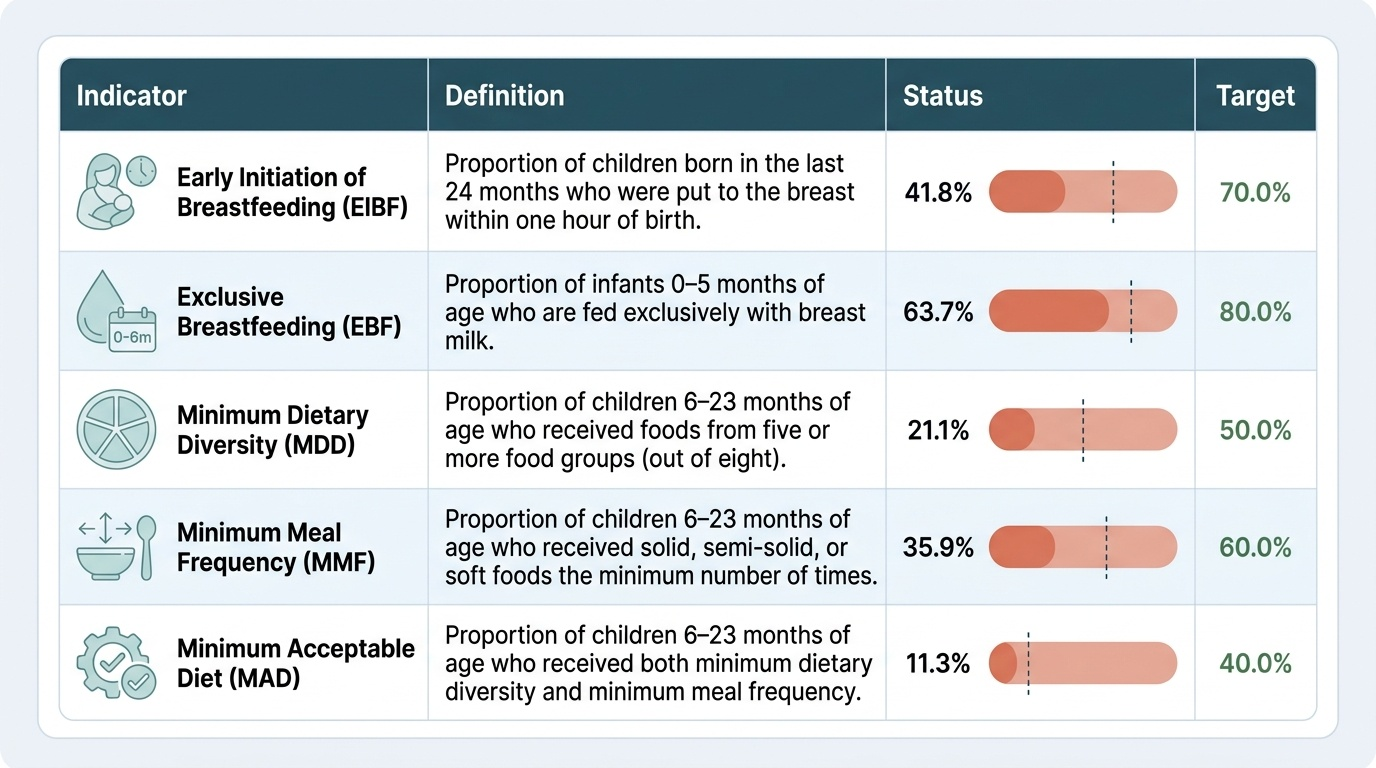
WHO standard IYCF indicators are used for programme monitoring and research. Key indicators include:
| Indicator | Definition | India NFHS-5 |
|---|---|---|
| Early initiation of BF | Breastfed within 1 hour of birth | 41.8% |
| Exclusive breastfeeding (<6 mo) | Only breast milk in last 24 h (0–5 mo) | 63.7% |
| Continued BF at 1 year | Breastfed at 12–15 months | 76.0% |
| Continued BF at 2 years | Breastfed at 20–23 months | 57.1% |
| Timely CF introduction (6–8 mo) | Solid/semi-solid food in last 24 h | 45.9% |
| Minimum dietary diversity | ≥4 food groups (6–23 mo) | 11.3% |
| Minimum meal frequency | Age-appropriate frequency (6–23 mo) | 42.7% |
These indicators reveal that while breastfeeding initiation and exclusivity have improved, the quality of complementary feeding (diversity and frequency) remains critically low — fewer than 1 in 8 Indian children 6–23 months achieves minimum dietary diversity.
Self-Assessment
The IYCF framework provides a precise, evidence-based specification for optimal infant feeding from birth to two years. Its five practices are sequential and interdependent: early initiation establishes the physiological foundation; exclusive breastfeeding for exactly 6 months protects against infection during the vulnerable period of gut immaturity; timely complementary feeding at 6 months prevents growth faltering as breast milk alone can no longer meet energy needs; continued breastfeeding to 2 years provides ongoing nutritional and immunological benefits; and responsive feeding throughout supports both nutrition and psychosocial development. In India, the programme infrastructure to deliver these messages — through ICDS, ASHA, BFHI, MAA, and POSHAN Abhiyaan — exists at scale, but persistent cultural practices and inadequate counselling quality limit impact. As a doctor, your role spans both individual clinical counselling and advocacy for IYCF-supporting policies within your institution and community. The WHO indicator set gives you the language to measure progress and identify which practices in your patient population need the most reinforcement. Test your understanding with the following questions.
SELF-CHECK
An HIV-positive mother on ART with an undetectable viral load delivers a healthy term infant in a district hospital in rural Chhattisgarh. Formula is not reliably available in her village. According to current NACO guidelines, what is the recommended feeding practice?
A. Exclusive formula feeding from birth — HIV is an absolute contraindication to breastfeeding
B. Exclusive breastfeeding for 6 months, then complementary foods with continued breastfeeding to 12 months, while maintaining ART
C. Mixed feeding (breast milk and formula) to reduce HIV transmission risk per feed
D. Expressed and heat-treated breast milk only, avoiding direct breastfeeding to prevent transmission
Reveal Answer
Answer: B. Exclusive breastfeeding for 6 months, then complementary foods with continued breastfeeding to 12 months, while maintaining ART
NACO guidelines in India recommend that HIV-positive mothers on ART who have an undetectable viral load should breastfeed exclusively for 6 months and continue breastfeeding to 12 months alongside complementary foods. This recommendation reflects the AFASS framework: in rural India, replacement feeding with formula is rarely affordable, feasible, acceptable, sustainable, and safe. The risk of diarrhoea, pneumonia, and malnutrition from not breastfeeding exceeds the residual HIV transmission risk (which is very low with effective ART and viral suppression). Mixed feeding — breast milk and formula — is the WORST option as it increases gut permeability and transmission risk. This guidance is India-specific and context-dependent; high-income country guidance differs.