Page 15 of 25
PE11.1-2 | Childhood Obesity Risk and Prevention — SDL Guide
Learning Objectives
- Describe the aetiology and pathophysiology of childhood obesity including primary and secondary causes
- Identify the clinical features, comorbidities, and metabolic consequences of obesity in children
- Apply IAP/WHO BMI-for-age criteria to classify overweight and obesity
- Discuss the risk approach to obesity and outline evidence-based prevention strategies
- Outline the principles of management of childhood obesity including lifestyle, pharmacological, and surgical approaches
INSTRUCTIONS
Childhood obesity has reached epidemic proportions in India and globally. It is no longer a condition confined to affluent families — urbanisation, changing dietary patterns, and screen-time have driven rates across all socioeconomic strata. The obese child is at risk of becoming the obese adult, carrying comorbidities that shorten life and reduce its quality. As a clinician you will encounter obese children in every paediatric setting; understanding the aetiology, recognising the metabolic consequences, and counselling families on prevention and management are core skills for any practitioner.
References
- Ghai Essential Pediatrics, 9th ed, Ch 7 (Nutrition & Obesity) (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 60 (Overweight and Obesity) (textbook)
- IAP Guidelines on Childhood Obesity, 2015 (guideline)
- WHO Growth Reference Charts, 2007 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rohan is a 10-year-old boy brought by his mother to the outpatient clinic because his school nurse flagged him as overweight. His mother insists he is 'just healthy' and eats well. On examination, you notice his collar is darker than his face — a velvety brown discolouration creeping across the back of his neck. His weight is 52 kg, height 138 cm, and his BMI plots at the 97th percentile for his age. He is breathless after climbing one flight of stairs. His father has type 2 diabetes. What is going on — and what is at stake if you simply reassure the family and send them home?
WHY THIS MATTERS
Childhood obesity is the most common nutritional disorder in Indian children today, with prevalence estimates ranging from 5% to 20% in urban school-age children (IAP 2015). It is not benign weight gain — it is a chronic disease with metabolic, cardiovascular, orthopaedic, and psychosocial sequelae that begin in childhood and compound over decades. More than 60% of obese children remain obese as adults. The paediatrician is in a unique position: intervening early — before insulin resistance progresses to type 2 diabetes, before arteries have stiffened, before a child's self-image has been permanently damaged — can change the entire trajectory of a life. Prevention starts before a single kilogram of excess fat has accumulated, with a risk-stratified approach to at-risk families.
RECALL
Before proceeding, recall from your growth and development modules: (1) how to plot BMI-for-age using IAP/WHO growth charts, and what the 50th, 85th, and 95th percentile lines represent; (2) the concept of adipose tissue as an endocrine organ producing adipokines including leptin, adiponectin, and resistin; (3) the role of insulin in glucose metabolism and how receptor resistance develops; (4) the physiological basis of energy balance: energy intake (diet) minus energy expenditure (basal metabolic rate + physical activity + thermogenesis). These concepts underpin every aspect of the clinical content that follows.
Clinical Presentation of Childhood Obesity
The clinical presentation of childhood obesity ranges from an incidental finding on routine health checks to an acute presentation of a complication such as sleep apnoea or orthopaedic pain. Most obese children are brought in by concerned parents or referred by school health programmes. On history, parents often report a pattern of high-calorie food preferences, excessive screen time (>2 hours/day), low physical activity, and difficulty with peer interactions. Family history is positive for obesity, type 2 diabetes, or dyslipidaemia in a first-degree relative in a substantial proportion of cases, reflecting the polygenic basis of primary obesity.
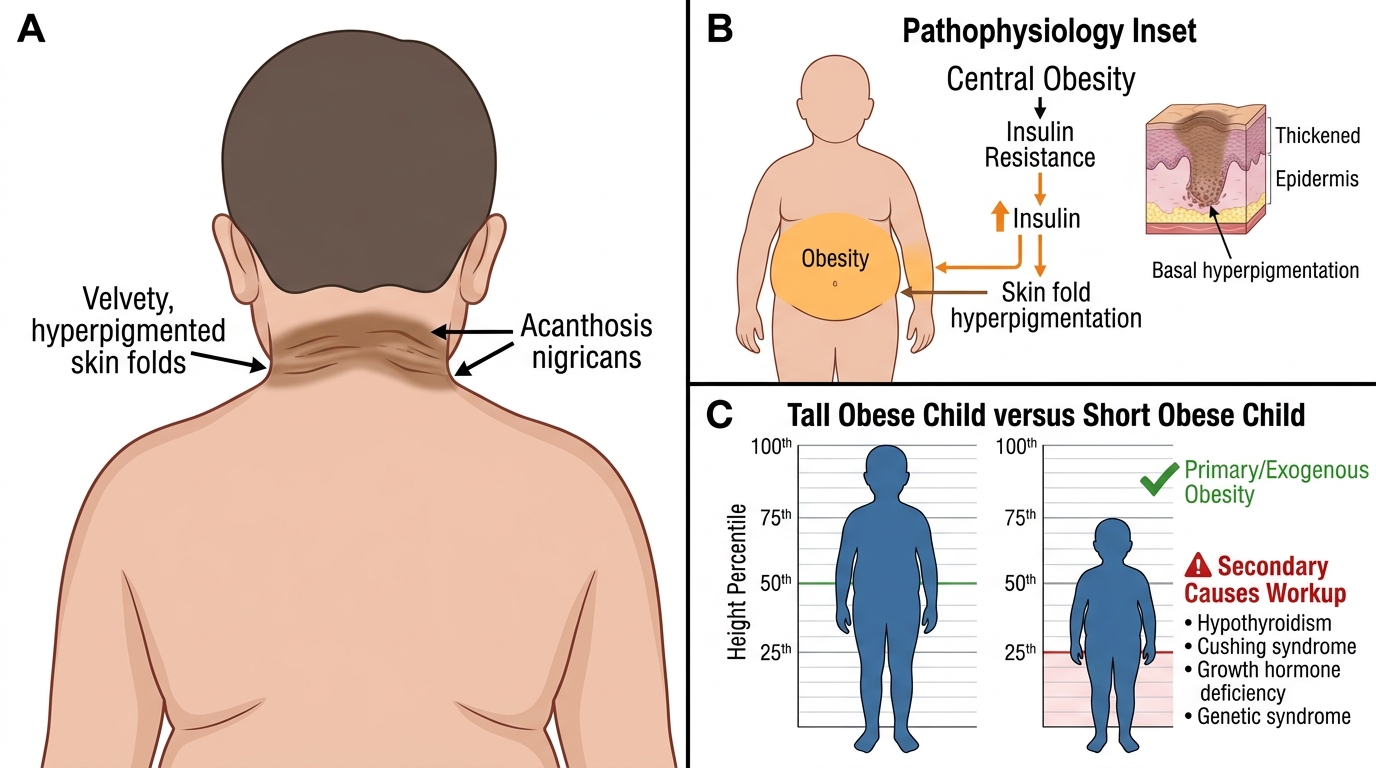
On general examination the most immediately visible feature is generalised adiposity, with excess fat deposition in the face, neck, trunk, and proximal limbs giving a characteristic rounded appearance. Acanthosis nigricans — a velvety, hyperpigmented, thickened skin change — is the single most important cutaneous marker of insulin resistance and must be specifically sought at the nape of the neck, axillae, and groin. Its presence should always prompt investigation for glucose intolerance. Striae distensae (stretch marks), most commonly over the thighs, lower abdomen, and upper arms, reflect rapid skin stretching from adipose expansion. Pseudogynaecomastia (fatty breast enlargement without true glandular tissue) is common in obese boys and must be distinguished from true gynaecomastia caused by hormonal imbalance. In obese girls, signs of polycystic ovary syndrome (PCOS) — hirsutism, acne, irregular menstruation — may emerge in adolescence.
Symptoms referable to comorbidities include: snoring and witnessed apnoeas (obstructive sleep apnoea, OSA); knee pain and gait abnormality (Blount's disease, slipped capital femoral epiphysis); fatigue and exercise intolerance; low mood, social withdrawal, or school refusal (psychosocial impact). Children with secondary causes present additional features: a short child with obesity suggests hypothyroidism or growth-hormone deficiency; a child with facial moonsign, central obesity, hypertension, and purple striae suggests Cushing syndrome; dysmorphic features with hypotonia and hyperphagia from infancy suggest Prader-Willi syndrome.
Pathophysiology and Aetiology
Understanding the aetiology of childhood obesity requires distinguishing between primary (exogenous/simple) obesity — which accounts for over 95% of cases — and secondary obesity due to an identifiable underlying cause. This distinction has direct therapeutic implications.
Primary (exogenous) obesity arises from a sustained positive energy balance: energy intake chronically exceeds energy expenditure. In Indian children, the drivers include high-calorie, energy-dense diets (refined carbohydrates, fried snacks, sugar-sweetened beverages), progressive reduction in physical activity, prolonged screen time, and changes in sleep patterns (short sleep duration is independently associated with obesity through ghrelin/leptin dysregulation). Genetic susceptibility amplifies these environmental exposures: first-degree relatives of obese individuals carry a 2–3-fold increased risk. Polygenic variants in genes regulating satiety (MC4R, FTO) confer a predisposition but do not cause obesity independently of the obesogenic environment. Epigenetic factors — maternal obesity, gestational diabetes, early formula feeding, antibiotic exposure — programme adiposity in early life.
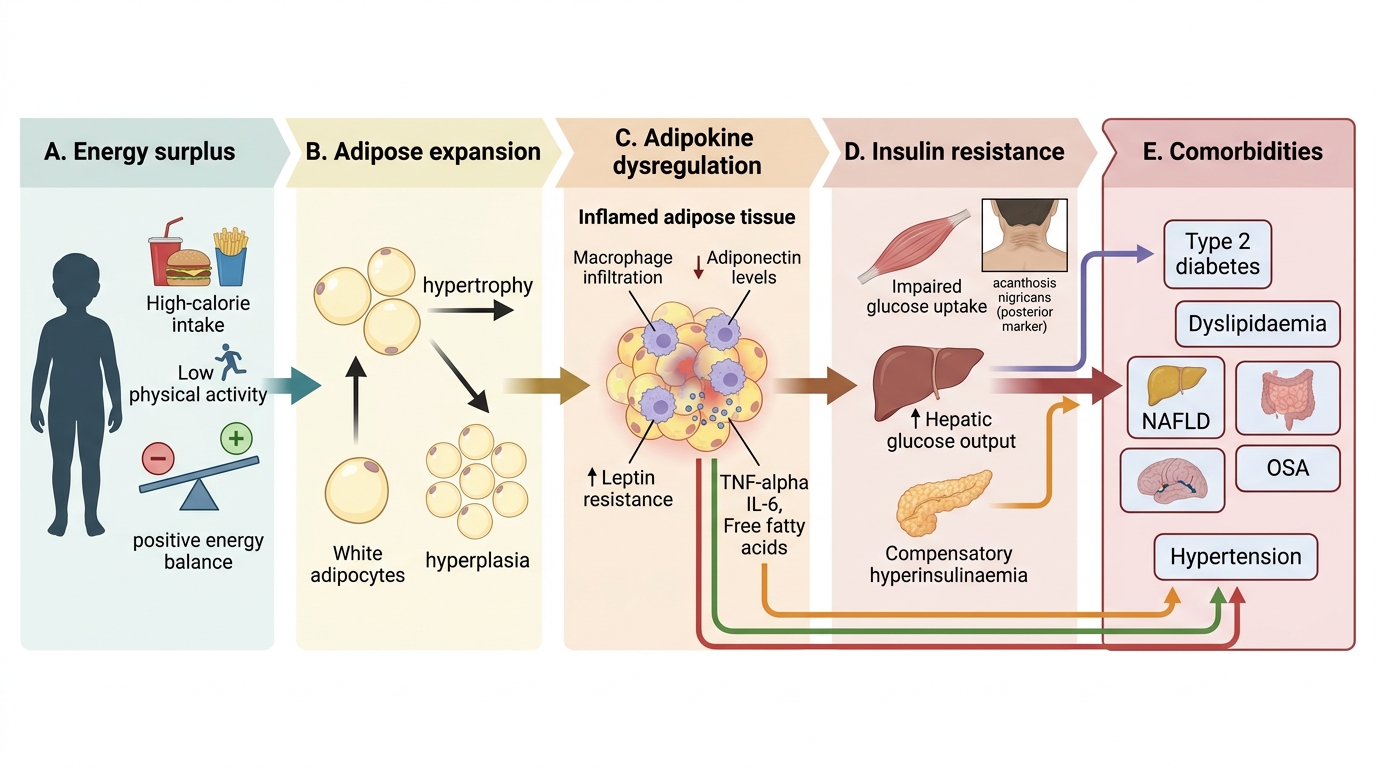
At the cellular level, adipose tissue expansion in primary obesity is initially adaptive, but beyond a threshold, adipocytes become dysfunctional: they secrete excess pro-inflammatory adipokines (TNF-α, IL-6, resistin) and reduced adiponectin (which normally sensitises muscle and liver to insulin). The resulting insulin resistance triggers compensatory hyperinsulinaemia, driving further lipogenesis and weight gain in a vicious cycle.
Secondary obesity must be actively excluded in children who are short (not tall, as in primary obesity), have developmental delay, dysmorphic features, or whose obesity has had a rapid onset at a young age:
- Endocrine causes: hypothyroidism (short stature, constipation, goitre, slow reflexes, dry skin); Cushing syndrome (central obesity, growth failure, hypertension, purple striae, buffalo hump — note: striae in primary obesity are silver/white, not purple); growth-hormone deficiency (short stature, central adiposity); PCOS in adolescent girls.
- Genetic syndromes: Prader-Willi syndrome (hypotonia + hyperphagia + short stature + hypogonadism + characteristic facial features, confirmed by FISH/methylation analysis on chromosome 15q11-q13); Bardet-Biedl syndrome (obesity + retinal dystrophy + polydactyly + intellectual disability + renal anomalies); single-gene defects in leptin, leptin receptor, or melanocortin-4 receptor (MC4R) pathway (rare, severe, early-onset).
- Iatrogenic: prolonged corticosteroids, atypical antipsychotics, valproate.
The South Asian phenotype is clinically critical: Indian children develop insulin resistance, visceral adiposity, and metabolic complications at a lower absolute BMI than Caucasian children. A child at the 85th BMI percentile may already harbour significant metabolic risk that would not be apparent from BMI alone — hence waist circumference and metabolic screening are essential alongside BMI.
Pathophysiology of Childhood Obesity
SELF-CHECK
A 9-year-old overweight girl is noted to have velvety, hyperpigmented skin on the nape of her neck. What is the MOST likely metabolic derangement this sign indicates?
A. Hypothyroidism
B. Insulin resistance
C. Cushing syndrome
D. Iron deficiency anaemia
Reveal Answer
Answer: B. Insulin resistance
Acanthosis nigricans is a cutaneous marker of insulin resistance, which occurs due to hyperinsulinaemia driving increased keratinocyte and fibroblast proliferation via insulin-like growth factor (IGF-1) receptors. It is strongly associated with obesity, type 2 diabetes risk, and metabolic syndrome in children. Hypothyroidism and Cushing syndrome cause obesity but do not characteristically cause acanthosis nigricans. Iron deficiency causes pallor, not skin thickening.
Comorbidities and Metabolic Consequences
Childhood obesity is not a cosmetic issue — it is a multi-system disease that affects virtually every organ system, and the consequences begin accumulating in the first decade of life, long before they become clinically apparent. The insidious nature of early metabolic and cardiovascular damage is precisely what makes obesity dangerous: a 10-year-old with elevated triglycerides, insulin resistance, and early left-ventricular hypertrophy has no symptoms and may present to you simply as a 'heavy child'. Unless the clinician actively screens for these complications at every encounter with an obese child, the window for effective early intervention will be missed. Understanding the full spectrum of comorbidities — and the investigations needed to detect them — is therefore not optional background knowledge but a clinical necessity. The comorbidities of childhood obesity are most usefully grouped by organ system, since this maps directly onto a systematic clinical and investigation approach.
Metabolic complications form the most dangerous cluster:
- Insulin resistance and impaired glucose tolerance affect up to 25% of obese adolescents; full type 2 diabetes mellitus occurs in 2–4%. The acanthosis nigricans and family history of T2DM are the key clinical pointers.
- Dyslipidaemia: elevated triglycerides and LDL, reduced HDL are common. This pattern tracks into adulthood and drives premature atherosclerosis.
- Non-alcoholic fatty liver disease (NAFLD): excess hepatic fat deposition, which may progress to non-alcoholic steatohepatitis (NASH) with fibrosis. Elevated transaminases (ALT > AST) are the biochemical signature. NAFLD is now the leading cause of chronic liver disease in paediatric age groups.
- Paediatric metabolic syndrome (IDF criteria for ≥10 years): waist circumference >90th percentile for age and sex, PLUS ≥2 of — triglycerides ≥150 mg/dL, HDL <40 mg/dL (boys)/<50 mg/dL (girls), blood pressure ≥130/85 mmHg, fasting plasma glucose ≥100 mg/dL.
Cardiovascular complications: left-ventricular hypertrophy, early carotid intima-media thickening, hypertension (using age/sex/height-adjusted paediatric blood pressure percentiles — >95th = hypertension in children).
Respiratory complications: obstructive sleep apnoea (OSA) is present in up to 25–40% of obese children; it causes fragmented sleep, daytime somnolence, behavioural issues, and pulmonary hypertension if untreated. Obesity hypoventilation syndrome is a more severe form.
Orthopaedic complications: Blount's disease (tibia vara — bowing due to excess medial tibial epiphyseal load), slipped capital femoral epiphysis (SCFE) (hip pain + limping in an obese adolescent = orthopaedic emergency), and flat feet are all increased in obese children.
Psychosocial complications: obesity carries a significant psychosocial burden — bullying, social isolation, poor body image, depression, and anxiety are common, and further reduce motivation for physical activity, creating a worsening cycle.
| Comorbidity | Key Feature | Investigation |
|---|---|---|
| Insulin resistance / T2DM | Acanthosis nigricans, FHx T2DM | Fasting glucose, 2-h OGTT, HbA1c |
| Dyslipidaemia | Often asymptomatic | Fasting lipid profile |
| NAFLD | Hepatomegaly, elevated ALT | LFTs, liver USG |
| OSA | Snoring, apnoeas, daytime sleepiness | Polysomnography |
| Hypertension | Headache, or incidental | BP (age/sex/height-corrected percentiles) |
| Blount's disease | Knee pain, gait abnormality | Knee X-ray |
| PCOS (girls) | Irregular menses, hirsutism | LH/FSH, testosterone, pelvic USG |
Acanthosis Nigricans and Growth Pattern in Childhood Obesity
CLINICAL PEARL
The 'tall obese child' vs 'short obese child' distinction is the first branch-point in aetiological diagnosis. Primary (exogenous) obesity causes children to grow TALL for their age — excess insulin and IGF-1 drive linear growth, and these children are typically above the 50th height percentile. Any obese child who is SHORT (below the 25th height percentile) must be investigated for a secondary cause (hypothyroidism, Cushing syndrome, growth-hormone deficiency, or a genetic syndrome). Applying this rule early avoids the costly and harmful error of attributing secondary obesity to overeating.