Page 16 of 25
PE11.1-2 | Childhood Obesity Risk and Prevention — SDL Guide (Part 2)
Diagnosis and Classification
The diagnosis of obesity in children requires age- and sex-adjusted reference standards, because body composition changes substantially throughout childhood and adolescence. A 12-year-old boy and a 6-year-old girl with the same absolute BMI value occupy very different positions on the population distribution for their respective ages and sexes. Using adult BMI cut-offs (≥25 for overweight, ≥30 for obese) is entirely inappropriate for paediatric patients: applying these adult thresholds to children will simultaneously miss significant obesity in younger age groups (where BMI naturally runs lower) and over-diagnose it in adolescents who are in a physiological phase of BMI rise. The correct approach is always to express the child's BMI as a percentile relative to age- and sex-matched peers, using validated national or international growth charts. In India, this means the IAP 2015 charts for school-age children and the WHO 2007 reference for under-fives.
BMI-for-age is the recommended screening tool. BMI (weight in kg ÷ height in m²) is calculated and then plotted on age- and sex-specific growth charts:
- Overweight: BMI-for-age ≥85th percentile (and <95th percentile)
- Obese: BMI-for-age ≥95th percentile
- Severely obese: BMI-for-age ≥99th percentile (or ≥120% of the 95th percentile value)
In India, the IAP growth charts (2015 revision) and WHO growth reference charts (2007) are used. For children aged 0–5 years, the WHO growth standards (multicountry) apply; for 5–18 years, the IAP 2015 charts (based on Indian data) are preferred.
Waist circumference is an essential complementary measure because BMI does not distinguish between visceral and subcutaneous fat. Waist circumference >90th percentile for age and sex indicates abdominal obesity and directly reflects the visceral fat load that drives metabolic risk. In the South Asian phenotype, waist circumference provides better metabolic risk discrimination than BMI alone at the same percentile.
Waist-to-height ratio >0.5 is an emerging simple cut-off for cardiometabolic risk applicable across ethnicities.
Differential diagnosis of obesity in children:
- Primary exogenous: normal/tall stature, no dysmorphism, positive family and dietary history
- Hypothyroidism: goitre, constipation, bradycardia, slow reflexes, short stature → TSH, T4
- Cushing syndrome: central distribution, purple striae, hypertension, moon face, buffalo hump → 24-h urinary free cortisol, midnight salivary cortisol
- Growth-hormone deficiency: short stature, central adiposity → IGF-1, GH stimulation test
- Prader-Willi: hypotonia in infancy → hyperphagia, hypogonadism, dysmorphism → methylation analysis
Investigations for newly diagnosed obese child (IAP recommended): fasting lipid profile; fasting glucose and 2-hour OGTT (in ≥10 yr with risk factors); HbA1c; liver enzymes (AST, ALT); thyroid function; blood pressure with correct cuff size; liver USG if ALT elevated.
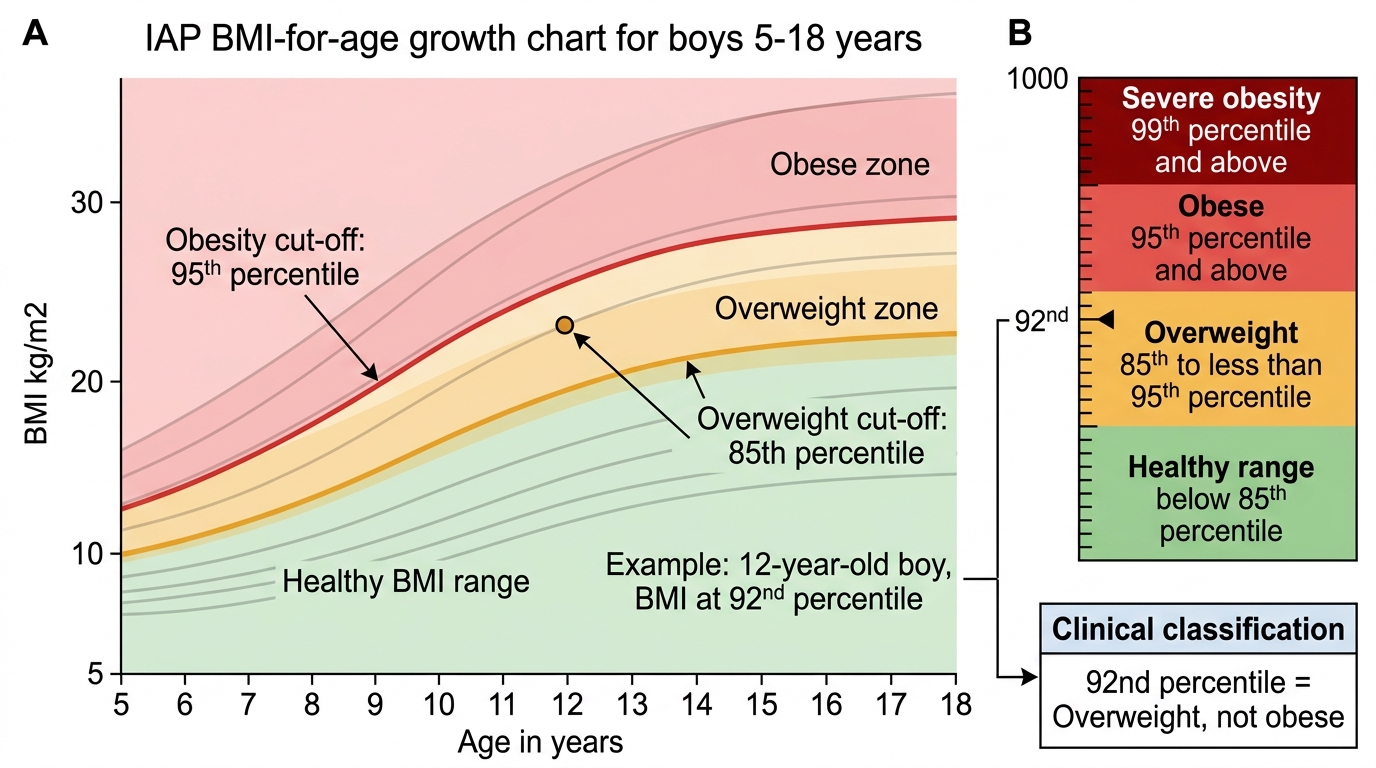
IAP BMI-for-Age Cut-offs for Boys
SELF-CHECK
A 12-year-old boy has a BMI that plots at the 92nd percentile for his age and sex on the IAP growth chart. How would you classify his weight status?
A. Normal weight (within the healthy range)
B. Overweight (≥85th but <95th percentile)
C. Obese (≥95th percentile)
D. Severely obese (≥99th percentile)
Reveal Answer
Answer: B. Overweight (≥85th but <95th percentile)
Per IAP/WHO criteria for children, overweight is defined as BMI-for-age at or above the 85th percentile but below the 95th percentile. Obese is ≥95th percentile. Since this child is at the 92nd percentile he is classified as overweight, not obese. This distinction matters for management intensity and counselling urgency.
Risk Factors and Prevention Strategies
Prevention of childhood obesity requires a systematic risk-stratified approach because interventions must be matched to the level of risk. Trying to apply intensive therapeutic interventions to the entire population wastes resources; equally, waiting for obesity to become established before acting means missing the optimal prevention window. The risk approach categorises children and families by their burden of predisposing factors and targets interventions accordingly. This is not merely a theoretical framework — it has direct practical consequences for every clinical encounter. At a well-child visit for a normal-weight 4-year-old whose both parents are obese and who watches television for four hours a day, the risk-stratified approach demands a brief, targeted counselling intervention that would not be warranted for a child with no such risk profile. Identifying and communicating modifiable risk factors is therefore as important a clinical skill as diagnosing established obesity, because the prevention dividend is far greater than any treatment benefit. In the Indian context, risk stratification must account for the South Asian phenotype — metabolic risk begins at a lower BMI and waist circumference than in Western populations, so the threshold for concern is correspondingly lower.
Provided image
Key modifiable risk factors for childhood obesity:
- Dietary: high-energy-density foods (ultra-processed snacks, fried foods, refined carbohydrates); sugar-sweetened beverages; large portion sizes; skipping breakfast; eating out frequently
- Physical activity: sedentary lifestyle; >2 hours/day screen time; lack of structured physical education; unsafe neighbourhood environments reducing outdoor play
- Sleep: short sleep duration (<9–10 h in school-age children) is independently associated with obesity through ghrelin/leptin dysregulation
- Family/parental factors: obese parents (genetic + shared environment risk); permissive feeding practices; lack of parental food literacy
- Early-life factors: excessive gestational weight gain; gestational diabetes; infant formula feeding vs breastfeeding; rapid infant weight gain (catch-up growth); early introduction of solid foods
- Socioeconomic: urbanisation, availability of unhealthy cheap food, reduced safe outdoor space
Non-modifiable risk factors: family history of obesity/T2DM, South Asian ethnicity (higher metabolic risk at given BMI), male sex (higher visceral adiposity).
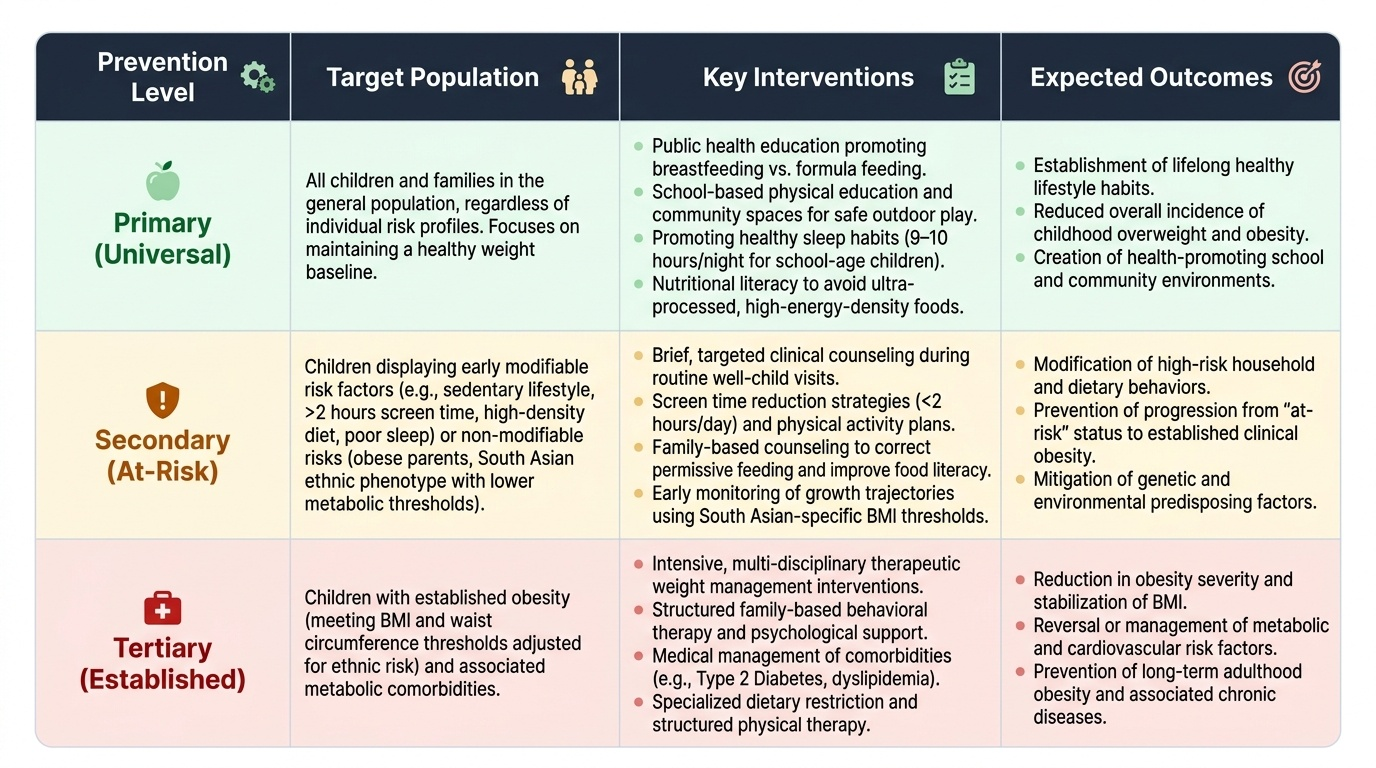
Prevention strategies (three tiers):
Primary prevention (universal — whole-population approach):
- Promotion of exclusive breastfeeding for 6 months (protective against childhood obesity)
- Complementary feeding guidance from 6 months — home-cooked, diverse, low-sugar foods
- Physical activity guidelines: ≥60 minutes of moderate-to-vigorous activity daily for children ≥5 years
- Screen-time restrictions: no screen time for <2 years; <1 hour/day for 2–5 years; <2 hours/day for school-age children
- School-based programmes: healthy canteen policies, physical education mandates, nutritional education
- Community/municipal-level: safe playgrounds, green spaces, front-of-pack food labelling (FSSAI Eat Right movement)
Secondary prevention (high-risk groups — risk approach):
- Identify children with ≥2 risk factors (obese parent + sedentary + dietary excess): targeted counselling at well-child visits
- Regular BMI monitoring from 2 years of age at every health contact
- Family-based dietary counselling: traffic-light food system, portion guidance, cooking demonstrations
- Active referral of 'at risk' children to structured lifestyle programmes before obesity develops
Tertiary prevention (established obesity — prevent complications):
- Intensive, multidisciplinary management (see below)
- Screen and manage comorbidities: dyslipidaemia, hypertension, insulin resistance, OSA
- Psychosocial support: anti-bullying programmes, mental health screening
Management Principles
The management of childhood obesity is multidisciplinary, family-centred, and long-term. It is fundamentally different from adult obesity management in two respects: first, the goal is usually weight maintenance rather than weight loss, because a growing child who maintains weight while gaining height will normalise their BMI percentile over time; and second, children cannot implement behaviour change independently — the family unit must be the primary target of any intervention. The primary goal for most obese children is weight maintenance (allowing BMI to normalise as the child grows taller); for severely obese children or those with significant comorbidities such as metabolic syndrome, a modest weight reduction target of 0.5–1 kg per month is appropriate. Crash dieting, very-low-calorie diets, and restrictive approaches are harmful in growing children because they compromise linear growth, micronutrient sufficiency, and long-term relationship with food, and must be explicitly avoided. Effective management requires the simultaneous engagement of the child, both parents, and often the school environment — no single-discipline intervention achieves durable results in isolation. The stepped-care model begins with lifestyle modification for all and escalates to pharmacotherapy or surgery only when lower steps have been genuinely attempted and failed.
1. Lifestyle modification — the foundation of all treatment:
- Dietary change: reduce energy-dense foods; increase fruits, vegetables, whole grains, and pulses; eliminate sugar-sweetened beverages; use smaller plates and structured meal times; involve the family (if only the child is counselled, compliance is poor)
- Physical activity: minimum 60 minutes of moderate-to-vigorous activity daily; reduce sedentary screen time; both structured exercise AND unstructured outdoor play contribute
- Behavioural strategies: goal-setting, self-monitoring (food diary, step counter), stimulus control (removing unhealthy food from the home environment), positive reinforcement
2. Family-centred approach: Since dietary patterns and physical activity habits are family phenomena, treating the child alone is ineffective. Parents must be co-enrolled in behaviour-change programmes. Motivational interviewing techniques are recommended.
3. Pharmacotherapy is indicated only for adolescents (≥12–16 years depending on the agent) with severe obesity AND comorbidities who have failed 6 months of lifestyle modification:
- Orlistat (pancreatic lipase inhibitor; reduces fat absorption): approved in adolescents ≥12 years; dose 120 mg with each fat-containing meal; adverse effects include steatorrhoea and fat-soluble vitamin malabsorption
- Metformin is sometimes used off-label for obese adolescents with insulin resistance or impaired glucose tolerance; it reduces hepatic glucose output and may modestly reduce weight
- Newer agents (GLP-1 receptor agonists such as liraglutide/semaglutide) are emerging in adolescent studies but are not currently standard practice in India for routine obesity management
4. Bariatric surgery is rarely indicated in paediatric practice in India; criteria include: BMI ≥40 (or ≥35 with severe comorbidities), completion of physiological maturity (Tanner stage ≥4), failure of ≥6 months of supervised lifestyle intervention, absence of uncontrolled psychiatric illness, and full informed consent from patient AND parents. Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy are the commonest procedures.
5. Management of comorbidities: treat dyslipidaemia, hypertension, insulin resistance, OSA, and orthopaedic complications concurrently — do not wait for weight loss to normalise them, especially if severe.
SELF-CHECK
A 14-year-old girl with BMI at the 98th percentile and acanthosis nigricans has a fasting glucose of 108 mg/dL. After 6 months of supervised lifestyle modification, her BMI remains at the 97th percentile. Which pharmacological agent is MOST appropriate to consider next?
A. Orlistat 60 mg three times daily
B. Metformin for insulin resistance
C. Liraglutide subcutaneous injection
D. Atorvastatin for dyslipidaemia
Reveal Answer
Answer: B. Metformin for insulin resistance
This adolescent has obesity with insulin resistance (acanthosis nigricans + impaired fasting glucose ≥100 mg/dL). After 6 months of failed lifestyle modification, metformin is a reasonable off-label option for insulin-resistant obese adolescents in India — it targets the underlying insulin resistance and may provide modest weight benefit. Orlistat is an option (approved ≥12 yr) but is more appropriate where dietary fat excess is the primary driver; it does not address insulin resistance directly. Liraglutide has limited evidence in Indian adolescents and is not standard of care. Atorvastatin treats dyslipidaemia, not the current priority of insulin resistance.
Self-Assessment
The following scenarios are designed to test your ability to integrate the clinical, diagnostic, and preventive concepts covered in this module. For each case, work through your reasoning before reading the answer. These are the kinds of clinical decision points you will encounter in paediatric outpatient settings, where rapid pattern recognition — distinguishing primary from secondary obesity, applying the correct classification cut-offs, and deciding when to escalate — directly affects patient outcomes. Approach each question as if you are at the bedside: generate your differential, apply the relevant criteria, and commit to a management action. Try each question without looking at the answer first; active retrieval practice and self-testing are far more powerful consolidation strategies than passive re-reading of notes.
- An 8-year-old boy presents with rapid-onset obesity over 6 months. He was previously thin. His mother notes he has been unusually tired, constipated, and has not grown much recently. On examination he has dry skin, slow deep-tendon reflexes, and a resting heart rate of 58. His BMI plots at the 93rd percentile. What is the MOST likely diagnosis and how would you confirm it?
Answer: Secondary obesity due to hypothyroidism. The short duration of onset, fatigue, constipation, dry skin, bradycardia, and slow reflexes all point to hypothyroidism. Confirm with serum TSH (elevated) and free T4 (low). Treatment with levothyroxine will restore normal growth velocity and BMI.
- A 10-year-old girl (BMI 97th percentile) is found to have a waist circumference at the 92nd percentile, triglycerides 178 mg/dL, HDL 36 mg/dL, and fasting glucose 104 mg/dL. Her blood pressure is 128/82 mmHg. Does she meet the IDF criteria for paediatric metabolic syndrome?
Answer: Yes. IDF criteria for ≥10 years require waist circumference >90th percentile (she has 92nd percentile) PLUS ≥2 of: TG ≥150 mg/dL ✓ (178), HDL <50 mg/dL in girls ✓ (36), BP ≥130/85 mmHg (she has 128/82 — just below), FPG ≥100 mg/dL ✓ (104). She has the mandatory waist criterion plus 3 out of 4 metabolic criteria — she meets metabolic syndrome criteria even without hypertension reaching the threshold.
- Counselling point: a mother asks why breastfeeding her new baby could matter for obesity prevention. What would you tell her?
Answer: Breastfeeding is associated with a 15–25% reduction in childhood obesity risk. Breast milk contains hormones (leptin, adiponectin) that programme satiety and fat metabolism; breastfed infants self-regulate intake better than formula-fed infants (who may be encouraged to 'finish the bottle'); and formula feeding is associated with faster early weight gain (a known obesity risk factor). WHO/IAP recommend exclusive breastfeeding for the first 6 months of life.