Page 16 of 33
PE12.8 | Vitamin C — SDL Guide
Learning Objectives
- State the RDA for vitamin C across paediatric age groups and identify the richest dietary sources in the Indian context
- Describe the specific biochemical functions of vitamin C including collagen synthesis, iron absorption, and antioxidant activity
- Explain the mechanisms by which vitamin C deficiency develops in infants and children
- Recognise the clinical features of scurvy in infants (Barlow's disease) and older children including characteristic X-ray findings
- Outline the management of scurvy with correct treatment and prevention strategies
INSTRUCTIONS
Vitamin C (ascorbic acid) deficiency causing scurvy is a preventable nutritional emergency that continues to be reported in Indian children, particularly infants exclusively fed boiled cow's milk and children on monotonous diets without fresh fruits or vegetables. Despite being historically associated with the pre-modern era, scurvy remains a diagnostic challenge today because its features — painful limbs, bleeding gums, and failure to thrive — mimic more common conditions. This module covers the RDA, food sources, biochemical roles, and the full clinical picture of scurvy, equipping you to diagnose and treat it confidently.
References
- Ghai Essential Pediatrics, 9th ed, Ch 8 — Nutrition (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 63 — Vitamin Deficiencies (textbook)
- ICMR/NIN Dietary Reference Values for Indians, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 10-month-old male infant is brought to the OPD with a 3-week history of severe irritability, refusal to move his legs, and fever. The mother reports that he has been exclusively fed boiled cow's milk since age 4 months. On examination, the infant screams when either leg is touched and holds both legs in a characteristic flexed and externally rotated posture (frog-leg position). There is no obvious swelling, but the thighs feel tense. The gums appear normal as the child has no teeth. What single nutritional deficiency explains this infant's extreme pain on limb movement, failure to thrive, and exclusive feeding history of boiled cow's milk?
WHY THIS MATTERS
Scurvy was the first nutritional deficiency to be treated by diet modification, yet it persists in India and globally, often misdiagnosed as osteomyelitis, child abuse, leukaemia, or viral arthritis. In infants, the hallmark subperiosteal haemorrhage causes exquisite pain that mimics septic arthritis or fracture. Understanding the biochemical basis of vitamin C's role in collagen synthesis explains not just scurvy but also the micronutrient interactions that matter in general paediatric health — vitamin C powerfully enhances non-haem iron absorption, meaning that vitamin C deficiency compounds iron deficiency anaemia. As a final-year student you will encounter infants and children from food-insecure households where fresh produce is unaffordable; recognising scurvy can prevent unnecessary invasive investigations and promptly reverse a condition that responds dramatically to supplementation within days.
RECALL
Before you proceed, recall from Biochemistry:
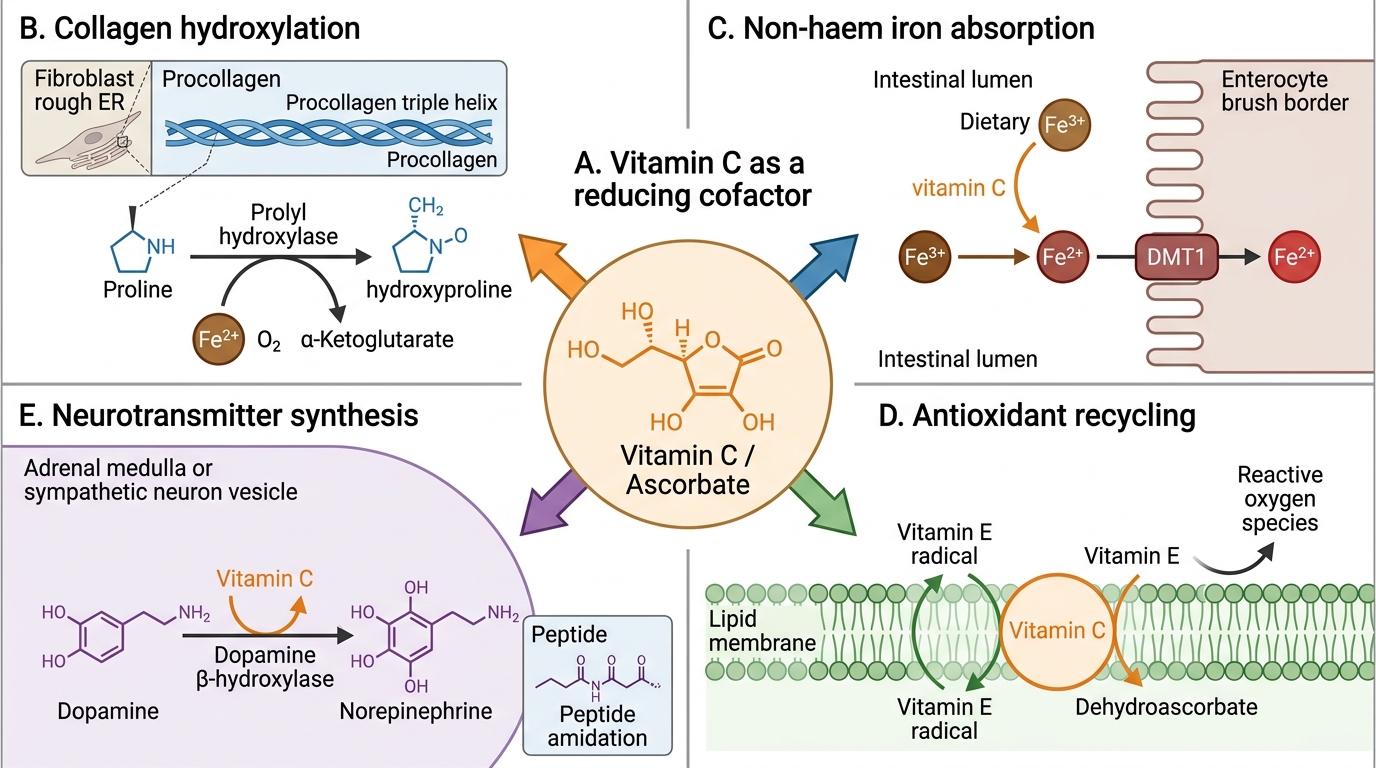
• Collagen is the most abundant structural protein in the body; its triple helix stability depends on hydroxyproline and hydroxylysine residues formed by post-translational hydroxylation of proline and lysine by prolyl and lysyl hydroxylases — enzymes that require vitamin C as an essential cofactor.
• Non-haem iron absorption is dependent on the reduction of dietary Fe³⁺ to Fe²⁺ in the acid environment of the duodenum; vitamin C is the most potent physiological reducing agent that facilitates this conversion.
• Antioxidant cascade: vitamin E (tocopherol) is regenerated from its oxidised radical form by vitamin C; this interdependence makes vitamin C a key component of the cellular antioxidant network.
• Water-soluble vitamins have limited storage; dietary supply must be continuous — in infants, breast milk or fortified formula is the primary source.
Vitamin C: Orientation and Clinical Significance
Vitamin C (ascorbic acid) is a water-soluble micronutrient that occupies a unique position in human biochemistry because — unlike most mammals — humans and other primates cannot synthesise it endogenously due to a mutation in the L-gulonolactone oxidase gene. This evolutionary loss makes continuous dietary intake essential. Vitamin C exists in two physiologically active redox forms: L-ascorbic acid (reduced, fully active) and dehydroascorbic acid (oxidised; absorbed and reduced back to ascorbate intracellularly). The body pool in adults is approximately 1500 mg, distributed primarily in adrenal glands, leucocytes, pituitary, brain, and eye; tissue saturation is reached at intakes of approximately 100 mg/day. In Indian paediatric practice, vitamin C deficiency producing scurvy (also called infantile scurvy or Barlow's disease when it occurs in infants) remains a reportable nutritional condition, particularly in:
• Exclusively breastfed infants of mothers with severe dietary restriction (though breast milk from a well-nourished mother contains ~50–70 mg/L of vitamin C).
• Infants fed exclusively boiled cow's milk — boiling destroys approximately 70–90% of vitamin C, and cow's milk naturally contains only ~1–2 mg/100 mL even before cooking.
• Older children on monotonous diets lacking fresh fruits and vegetables, particularly during droughts or food insecurity.
• Children with malabsorption syndromes (inflammatory bowel disease, short bowel syndrome).
Biochemical Roles of Vitamin C
RDA, Dietary Sources, and Biochemical Functions
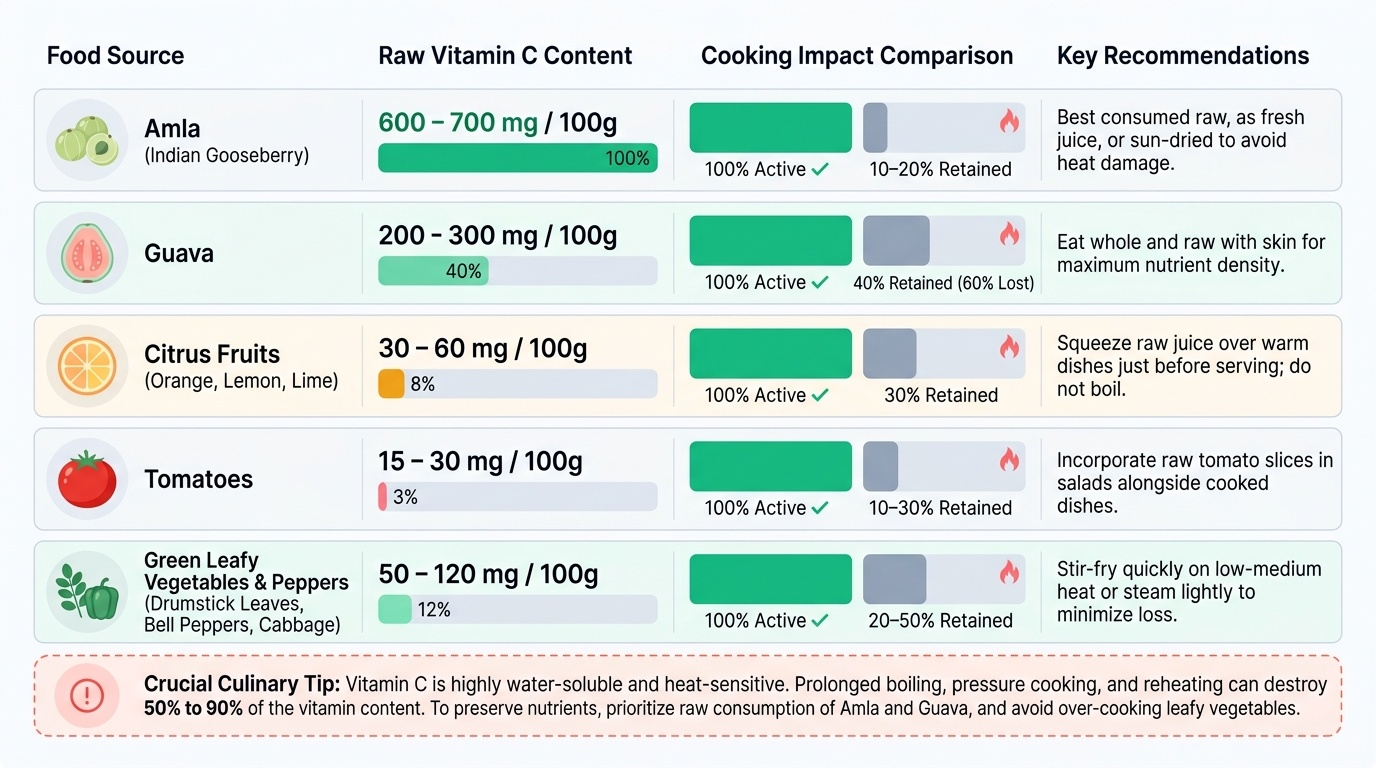
The Recommended Dietary Allowance (RDA) for vitamin C in India, as set by the ICMR/NIN (2020), is 40 mg/day for infants (0–12 months) and children (1–9 years), rising to 65 mg/day for adolescents (10–17 years). These values reflect the amount needed to maintain tissue saturation above the scurvy threshold (approximately 10 mg/day is the minimum to prevent scurvy) while accounting for the bioavailability of dietary ascorbate. India is fortunate in having some of the world's richest vitamin C sources available locally at low cost: amla (Indian gooseberry) contains 600–700 mg/100 g, making it the single richest natural source globally; guava contains 200–300 mg/100 g; citrus fruits (orange, lime, lemon) provide 30–60 mg/100 g; and bell peppers, tomatoes, drumstick leaves, and raw cabbage are accessible seasonal sources. The critical problem is heat instability — vitamin C is oxidised and destroyed by cooking; boiling, pressure cooking, and prolonged reheating reduce content by 50–90%. Foods consumed raw (guava, amla) retain their full vitamin C content.
Provided image
Biochemical functions of vitamin C — specific mechanisms:
1. Collagen biosynthesis: Prolyl hydroxylase and lysyl hydroxylase, the enzymes responsible for post-translational hydroxylation of proline and lysine residues in procollagen, require ascorbate as an electron donor to keep the active-site Fe²⁺ in its reduced state. Without vitamin C, these enzymes become inactive, collagen chains lack hydroxyproline cross-links, and the triple helix is thermally unstable at body temperature — structural integrity of blood vessels, bone matrix, cartilage, skin, and connective tissue all fail simultaneously.
2. Non-haem iron absorption: In the acid environment of the proximal duodenum, dietary Fe³⁺ (the predominant form in plant foods and fortified foods) must be reduced to Fe²⁺ to be transported across the enterocyte by divalent metal transporter 1 (DMT1). Vitamin C reduces Fe³⁺ to Fe²⁺ directly in the gut lumen, acting as the most potent enhancer of non-haem iron absorption; 50 mg of vitamin C with a meal can increase non-haem iron absorption by 2–4 fold.
3. Antioxidant function: Ascorbate donates electrons to scavenge superoxide, hydrogen peroxide, and hydroxyl radicals; it also regenerates alpha-tocopherol (vitamin E) from the tocopheroxyl radical, thereby recycling the lipid-phase antioxidant.
4. Neurotransmitter and hormone synthesis: Dopamine beta-hydroxylase, which converts dopamine to noradrenaline, requires vitamin C; carnitine biosynthesis (from lysine/methionine) requires vitamin C-dependent hydroxylases.
5. Immune function: High concentrations of ascorbate in leucocytes support chemotaxis, phagocytosis, and killing of pathogens; vitamin C deficiency impairs immune responses.
SELF-CHECK
A mother asks why her 8-month-old infant, who has been drinking boiled cow's milk, is not getting enough vitamin C. Which is the most accurate explanation?
A. Cow's milk naturally contains no vitamin C
B. Boiling destroys most of the small amount of vitamin C present in cow's milk
C. Cow's milk vitamin C is poorly absorbed in infants
D. The infant's kidneys excrete vitamin C more rapidly than adults
Reveal Answer
Answer: B. Boiling destroys most of the small amount of vitamin C present in cow's milk
Cow's milk naturally contains approximately 1–2 mg/100 mL of vitamin C — an already small amount compared to the infant RDA of 40 mg/day. Boiling destroys 70–90% of this residual vitamin C through heat oxidation and exposure to oxygen. The result is that boiled cow's milk provides virtually no vitamin C to the infant. Breast milk from a well-nourished mother provides ~50–70 mg/L, meeting infant needs. Cow's milk does contain small amounts of vitamin C (making option A incorrect), and absorption and renal excretion are not the primary issue.
Mechanisms Leading to Vitamin C Deficiency
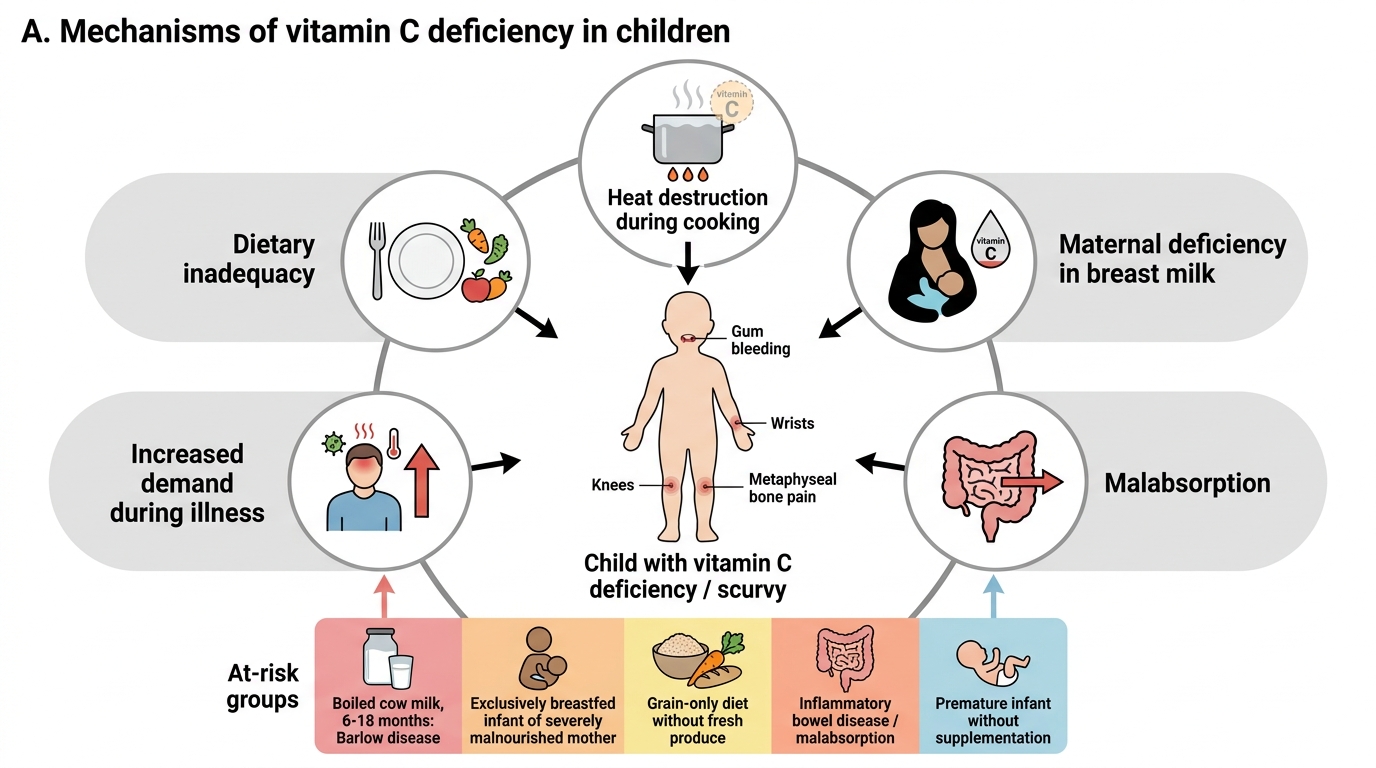
Vitamin C deficiency arises when dietary intake consistently falls below the minimum threshold (approximately 10 mg/day) for a period of 1–3 months, depleting tissue stores. In paediatric practice, several specific pathways lead to this state. The most important in infancy is exclusive feeding on boiled or processed cow's milk: cow's milk has naturally low vitamin C content (~1–2 mg/100 mL), which is almost entirely destroyed by the boiling routinely practised in Indian households for safety reasons. An infant subsisting on this alone cannot meet the 40 mg/day RDA; scurvy develops by 6–18 months of age. Breast milk from a well-nourished mother provides adequate vitamin C, but if the mother herself is severely deficient — as may occur in food-insecure households — breast milk concentrations are reduced. Dietary monotony is the second major cause: older children who eat very restricted diets (predominantly cereals and dal without fresh fruits or vegetables) gradually become depleted; droughts and food shortages in rural areas can precipitate outbreaks. Heat and oxidation during food preparation are significant: vitamin C is not only destroyed by boiling and pressure cooking but is also oxidised by exposure to air during chopping and storing cut produce. Traditional Indian cooking methods — prolonged boiling of vegetables with reheating across meals — dramatically reduce residual vitamin C. Malabsorption from Crohn's disease, celiac disease, or short bowel syndrome impairs absorption. Increased demand during febrile illness (infections increase metabolic use of vitamin C) and in prematurity (premature infants have lower tissue stores and higher requirements).
Mechanisms of Vitamin C Deficiency in Children
- At-risk groups:
- Infants on boiled cow's milk (6–18 months age) — Barlow's disease
- Exclusively breastfed infants of severely malnourished mothers
- Children on grain-only diets without fresh produce
- Children with inflammatory bowel disease or malabsorption
- Premature infants without adequate supplementation