Page 17 of 33
PE12.8 | Vitamin C — SDL Guide (Part 2)
Scurvy: Clinical Features, Diagnosis, and Management
Scurvy is the clinical syndrome of severe vitamin C deficiency; its manifestations are a direct consequence of defective collagen synthesis causing structural failure of blood vessels, bone, and connective tissue. The clinical picture differs between infants and older children.
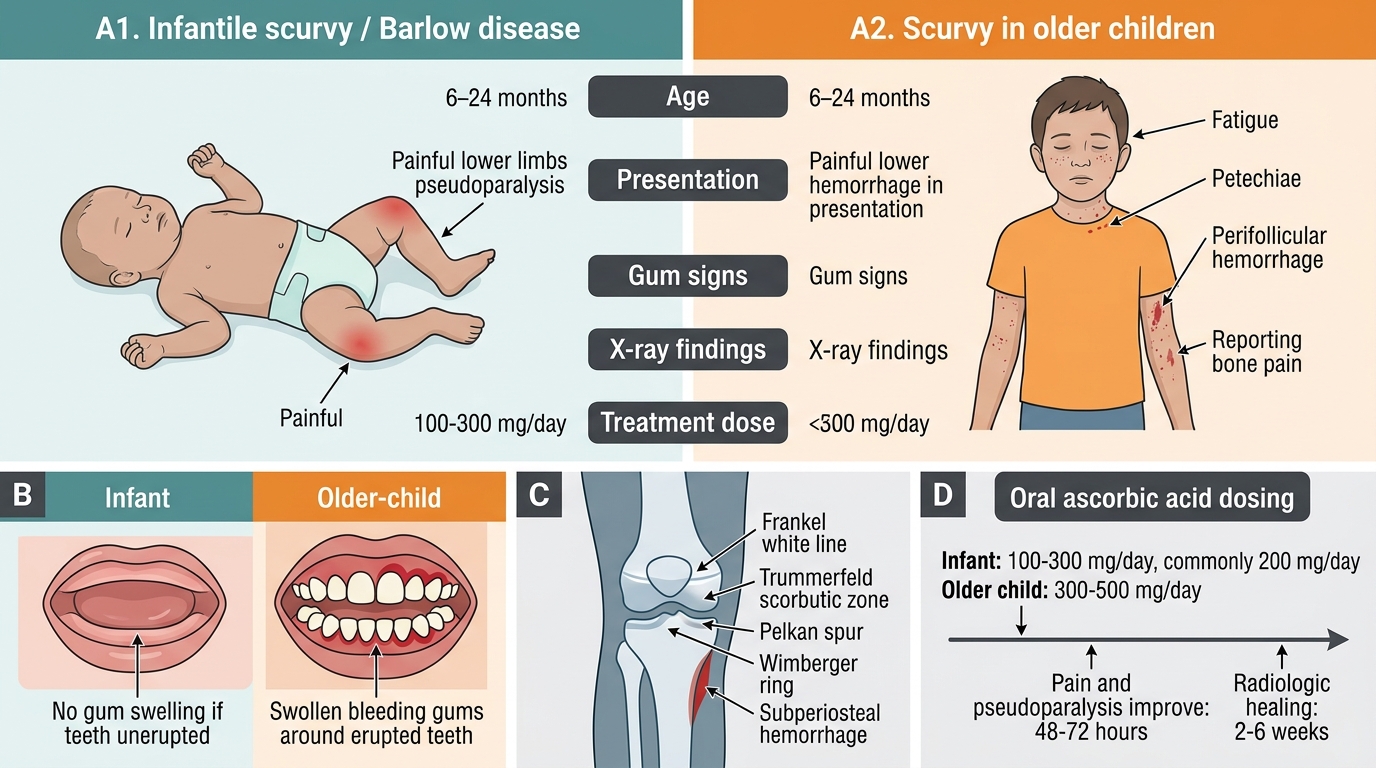
Infantile scurvy (Barlow's disease) — 6 to 18 months:
The cardinal presentation is extreme irritability and pseudoparalysis — the infant refuses to move the limbs (especially legs) and screams on handling because any movement causes intense pain from subperiosteal haemorrhages. These haemorrhages lift the periosteum from the bone (most commonly the distal femur, proximal tibia, and costochondral junctions), causing a tender, fusiform swelling felt along the bones. The infant characteristically adopts a frog-leg posture — hips flexed, abducted, and externally rotated — to minimise periosteal tension. Since most infants at this age are preverbal and have few or no teeth, the classic gum bleeding may not be present; the diagnosis must be made on the clinical picture and feeding history. Other features include perifollicular haemorrhages (fine petechiae around hair follicles), poor wound healing, low-grade fever, and anaemia (from both the haemorrhage and concurrent iron deficiency, since vitamin C deficiency also impairs iron absorption).
Scurvy in older children:
Older children present with bleeding gums — swollen, haemorrhagic, and spongy gingival tissue that bleeds on minimal contact (only where teeth are present); this is not seen in infants without teeth. Perifollicular haemorrhages and corkscrew hairs (coiled hair follicles surrounded by hyperkeratosis) on the trunk and limbs are characteristic. Splinter haemorrhages under nails, subconjunctival haemorrhage, and easy bruising reflect widespread capillary fragility from defective collagen. Wound healing is grossly impaired; old, healed wounds may re-open (dehiscence). Skeletal pain from subperiosteal haemorrhage can present as limb pain and limp. Systemic features include fatigue, irritability, and failure to thrive.
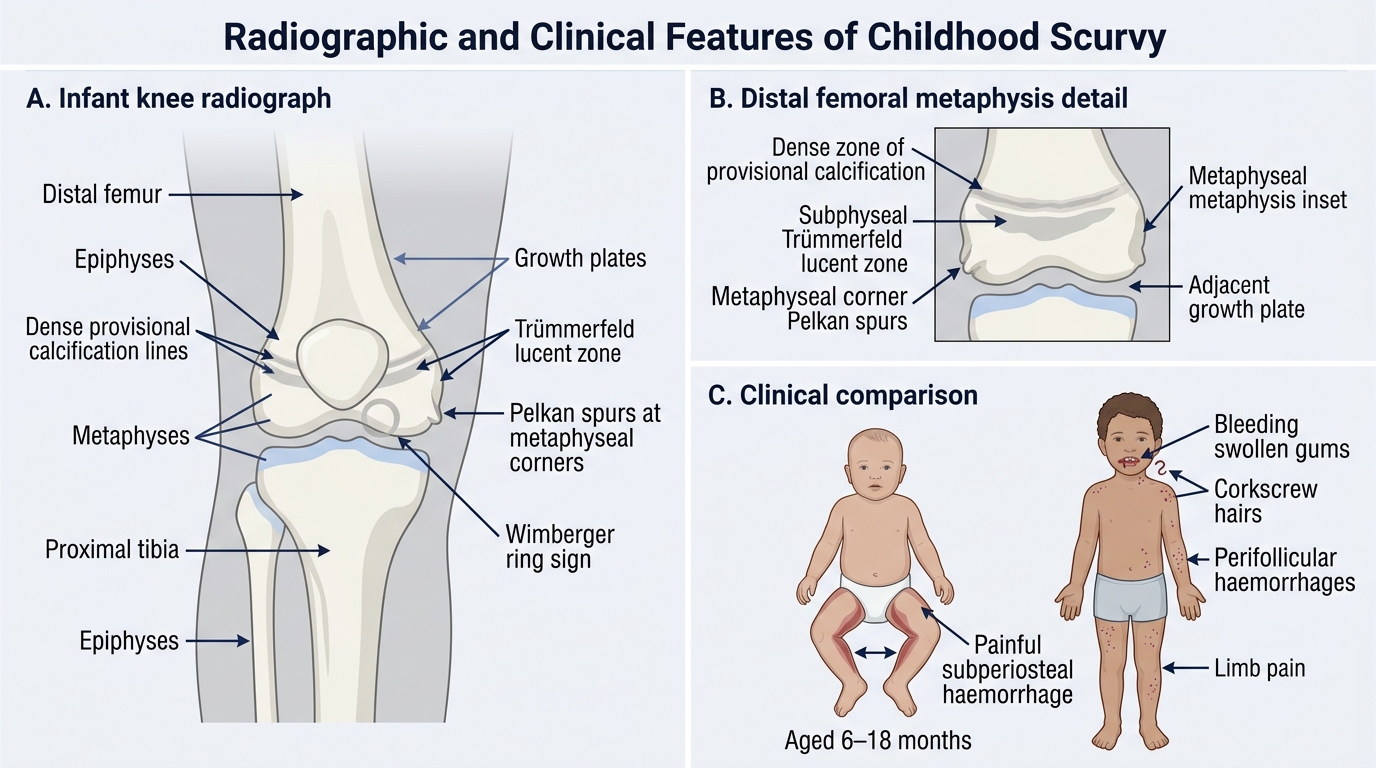
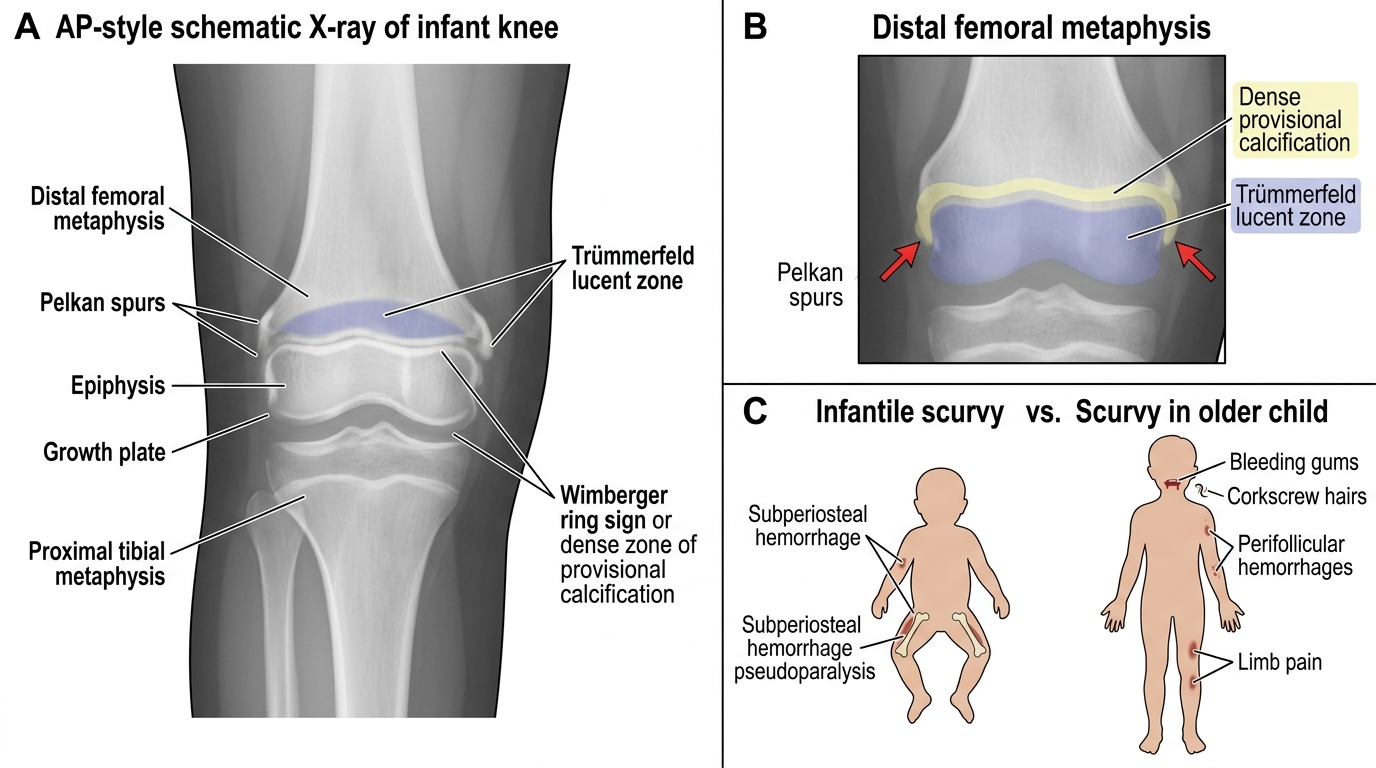
Radiological findings (X-ray long bones):
• Trümmerfeld zone: a transverse lucent band at the metaphysis reflecting osteoid failure
• Pelkan's spurs: bony spurs at the corners of the metaphysis
• Wimberger's ring sign: a dense white ring of calcification around the epiphysis (appears on healing)
• Subperiosteal haemorrhage: appears as periosteal lifting and new bone formation along the shaft on healing
Diagnosis: Clinical history (feeding history + characteristic features) + X-rays are usually sufficient. Serum ascorbate <0.2 mg/dL (11 µmol/L) is diagnostic; whole-blood ascorbate is more reliable. A therapeutic trial (clinical response within 48–72 hours of vitamin C) also confirms the diagnosis.
Management: Oral ascorbic acid 100–200 mg/day in three divided doses for infants; 300–500 mg/day for older children; continue for 2–3 weeks until tissue stores are replenished. Severe cases with IV access may receive parenteral ascorbate. Pain and irritability improve within 48–72 hours of treatment. Subperiosteal haemorrhages gradually resorb; skeletal abnormalities resolve with healing. Dietary counselling is essential: introduce fresh fruits (guava, citrus), vegetables, or supplemental vitamin C to prevent recurrence. All infants on formula or cow's milk should receive vitamin C-containing complementary foods from 6 months.
Radiographic and Clinical Features of Childhood Scurvy
Radiographic and Clinical Features of Childhood Scurvy
| Feature | Infantile scurvy (Barlow's) | Scurvy in older child |
|---|---|---|
| Age | 6–18 months | >18 months |
| Key presentation | Pseudoparalysis, frog-leg posture | Bleeding gums, corkscrew hairs |
| Bone changes | Subperiosteal haemorrhage | Subperiosteal haemorrhage, limb pain |
| Gum bleeding | Absent (no teeth yet) | Present (swollen, haemorrhagic gums) |
| Skin | Perifollicular petechiae | Perifollicular haemorrhages, corkscrew hairs |
| X-ray | Trümmerfeld zone, Pelkan spurs | Similar but less dramatic |
| Treatment | Ascorbic acid 100–200 mg/day oral | Ascorbic acid 300–500 mg/day oral |
CLINICAL PEARL
Three clinical traps in scurvy:
1. Infants with scurvy have no teeth — so no gum bleeding. The classic textbook sign of haemorrhagic gums is absent in infants under 6–8 months who are pre-dentate. Do not rule out scurvy because the gums look normal.
2. The frog-leg posture is a pain response, not a neurological sign. The infant lies with hips flexed and externally rotated to relieve periosteal tension; this is often confused with a hip or bone infection. The feeding history (boiled cow's milk) and dramatic response to vitamin C within 2–3 days are the diagnostic clues.
3. Vitamin C deficiency worsens iron deficiency anaemia. The co-existence of dietary vitamin C deficiency and iron deficiency is common; vitamin C's role in reducing Fe³⁺ to Fe²⁺ means that correcting both deficiencies together is more effective than treating iron alone. Always assess both.
Self-Assessment
Vitamin C deficiency presents in patterns that, once recognised, are clinically unmistakable — yet they are frequently misdiagnosed as orthopaedic infections, haematological malignancies, or child abuse. The key to confident diagnosis is integrating the age of the child, the feeding history, and the specific pattern of clinical signs. Use these vignettes to test your recognition skills before reviewing the summary. Apply the framework: what is the mechanism for each clinical sign? What is the earliest sign? What investigation would confirm, and what treatment would you start?
Vignette 1: A 12-month-old infant is referred from a peripheral health centre with a 4-week history of crying on being picked up, refusing to move his legs, and swelling of the thighs. He has been exclusively fed boiled buffalo milk since 5 months of age. He has no teeth. Temperature is 38.1°C. X-ray of the thigh shows periosteal lifting along the femoral shaft and a lucent transverse band at the distal femoral metaphysis.
• What is the diagnosis?
• Explain the mechanism of the pseudoparalysis.
• What treatment will you prescribe and for how long?
• What dietary advice will you give to the mother?
Vignette 2: An 8-year-old girl from a semi-arid district presents with swollen, bleeding gums, easy bruising over the legs, and small coiled hairs surrounded by redness over her trunk. Her family subsists on a diet of millet and lentils during a drought period. She appears pale.
• Name the deficiency and explain the gum finding.
• Which two conditions should you also screen for in the same dietary context?
• What is the daily dose of vitamin C for treatment in her age group?
• Name two locally available affordable foods you would recommend to prevent recurrence.
Infantile Scurvy vs Scurvy in Older Children
SELF-CHECK
A 14-month-old infant with scurvy is started on oral ascorbic acid 200 mg/day. Within what timeframe would you expect the irritability and pseudoparalysis to begin to resolve?
A. 6–8 weeks (time for collagen remodelling to complete)
B. 48–72 hours (vitamin C rapidly restores collagen synthesis and reduces pain from haemorrhage)
C. 1–2 weeks (time for subperiosteal haemorrhages to fully resorb)
D. 24 hours (immediate normalisation of bone density)
Reveal Answer
Answer: B. 48–72 hours (vitamin C rapidly restores collagen synthesis and reduces pain from haemorrhage)
Irritability and pseudoparalysis (the pain from subperiosteal haemorrhage) begin to improve within 48–72 hours of starting vitamin C, as collagen synthesis is rapidly restored and the acute inflammatory response in the periosteum begins to resolve. This rapid response is diagnostically useful — if there is no improvement within 72 hours, the diagnosis should be reconsidered. Full resolution of subperiosteal haemorrhages and radiological healing takes 2–6 weeks, but the child's pain and functional recovery are much faster. Immediate normalisation of bone density in 24 hours would not be physiologically possible.