Page 7 of 33
PE12.4 | Vitamin E — SDL Guide
Learning Objectives
- Describe the dietary sources, RDA, and absorption of Vitamin E
- Explain the antioxidant mechanism by which Vitamin E protects cell membranes and neurons
- Identify the two principal clinical groups at risk of Vitamin E deficiency in paediatric practice
- Describe the clinical features of Vitamin E deficiency in preterm infants (haemolytic anaemia, thrombocytosis, oedema)
- Describe the neurological syndrome of chronic Vitamin E deficiency (spinocerebellar degeneration, peripheral neuropathy, retinopathy)
- Outline the diagnosis and management of Vitamin E deficiency
INSTRUCTIONS
Vitamin E deficiency is uncommon in healthy, term children with adequate nutrition — making it easy to overlook. Yet in two specific groups — premature infants and children with chronic fat malabsorption — it causes serious, preventable disease. Understanding the antioxidant role of Vitamin E and the consequences of its absence at the cellular level will help you recognise haemolytic anaemia of prematurity and the progressive neurological syndrome of fat malabsorption, and prescribe appropriate supplementation.
References
- Ghai Essential Pediatrics, 9th ed., Ch 9 (Vitamins and Minerals — Vitamin E) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 64 (Vitamin E Deficiency) (textbook)
- Kliegman's Nelson Essentials of Pediatrics, Ch 11 (Nutritional Disorders) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 30-week premature infant is now 5 weeks old in the neonatal intensive care unit. He had an uncomplicated course initially but is now noted to have a declining haemoglobin (from 14 g/dL at birth to 8.5 g/dL), mild pitting oedema of the legs, and a platelet count of 720 × 10⁹/L. A peripheral smear shows fragmented red cells and acanthocytes. The infant has been receiving iron supplementation since week 2 of life. Direct Coombs test is negative. What is the most likely nutritional cause of this clinical picture, and what supplement should have been given from birth to prevent it?
WHY THIS MATTERS
Vitamin E occupies a unique niche in paediatric nutrition: it is the body's primary fat-soluble antioxidant, protecting cell membrane phospholipids from oxidative destruction by free radicals. In healthy term infants and older children, Vitamin E deficiency is extremely rare because placental transfer provides adequate stores at birth and dietary intake is sufficient thereafter. However, in two specific and clinically important groups — premature infants (who miss the third-trimester placental transfer) and children with chronic fat malabsorption (who cannot absorb fat-soluble vitamins) — Vitamin E deficiency causes distinct and serious syndromes. In premature infants, it causes haemolytic anaemia, thrombocytosis, and oedema in the first weeks of life; this may be aggravated by iron supplementation (iron generates reactive oxygen species that deplete antioxidant defences). In malabsorption disorders (abetalipoproteinaemia, cholestasis, cystic fibrosis), chronic deficiency over years leads to irreversible spinocerebellar degeneration, peripheral neuropathy, and pigmentary retinopathy. Recognising these clinical scenarios allows timely supplementation.
RECALL
From Physiology and Biochemistry (Year 1), recall the absorption of fat-soluble vitamins (A, D, E, K). They all require bile salts for emulsification in the intestinal lumen, are incorporated into mixed micelles for uptake by enterocytes, and are then packaged into chylomicrons for transport via lymphatics to the systemic circulation — bypassing the portal vein. Any condition that impairs bile formation (cholestasis), reduces intestinal absorptive surface (short bowel), or interferes with chylomicron assembly (abetalipoproteinaemia) will disrupt fat-soluble vitamin absorption. From Biochemistry, recall the concept of lipid peroxidation: reactive oxygen species (free radicals) attack the double bonds in unsaturated fatty acid chains of membrane phospholipids, creating lipid peroxyl radicals that propagate chain reactions, damaging cell membranes. Antioxidants interrupt this cycle — Vitamin E is the membrane-embedded chain-breaking antioxidant that donates a hydrogen atom to lipid peroxyl radicals, neutralising them before they can damage adjacent phospholipids.
Orientation: Why Vitamin E Matters in Paediatric Practice
Vitamin E is a group of eight fat-soluble compounds — four tocopherols (alpha, beta, gamma, delta) and four tocotrienols — of which alpha-tocopherol is the most biologically active and the form predominantly retained in human tissues. Its principal biological role is as a membrane-embedded chain-breaking antioxidant: it intercepts lipid peroxyl radicals at the phospholipid bilayer of cell membranes, halting the propagation of oxidative chain reactions that would otherwise destroy membrane integrity. This antioxidant function is especially critical in tissues with high metabolic activity, high polyunsaturated fatty acid content, or high exposure to oxidative stress — notably red blood cells (particularly in preterm infants exposed to high-oxygen environments), myelin sheaths of peripheral nerves, photoreceptors of the retina, and spinocerebellar tracts.
The clinical relevance of Vitamin E deficiency in paediatrics is concentrated in two populations:
1. Premature infants (<34 weeks gestation): Placental transfer of Vitamin E occurs predominantly in the third trimester; infants born early have low hepatic stores, thin subcutaneous fat, and immature antioxidant enzyme systems. Combined with the often-necessary administration of iron (which generates reactive oxygen species via the Fenton reaction), the red cell membrane is vulnerable to peroxidative haemolysis in the first weeks of life.
2. Children with chronic fat malabsorption: Any condition disrupting fat-soluble vitamin absorption — abetalipoproteinaemia, chronic cholestatic liver disease, cystic fibrosis with exocrine pancreatic insufficiency, short bowel syndrome — can cause progressive, and sometimes irreversible, Vitamin E deficiency affecting the nervous system and retina.
Vitamin E deficiency is not a concern in healthy, term, orally-fed infants and children — it should only be investigated when the above risk factors are present.
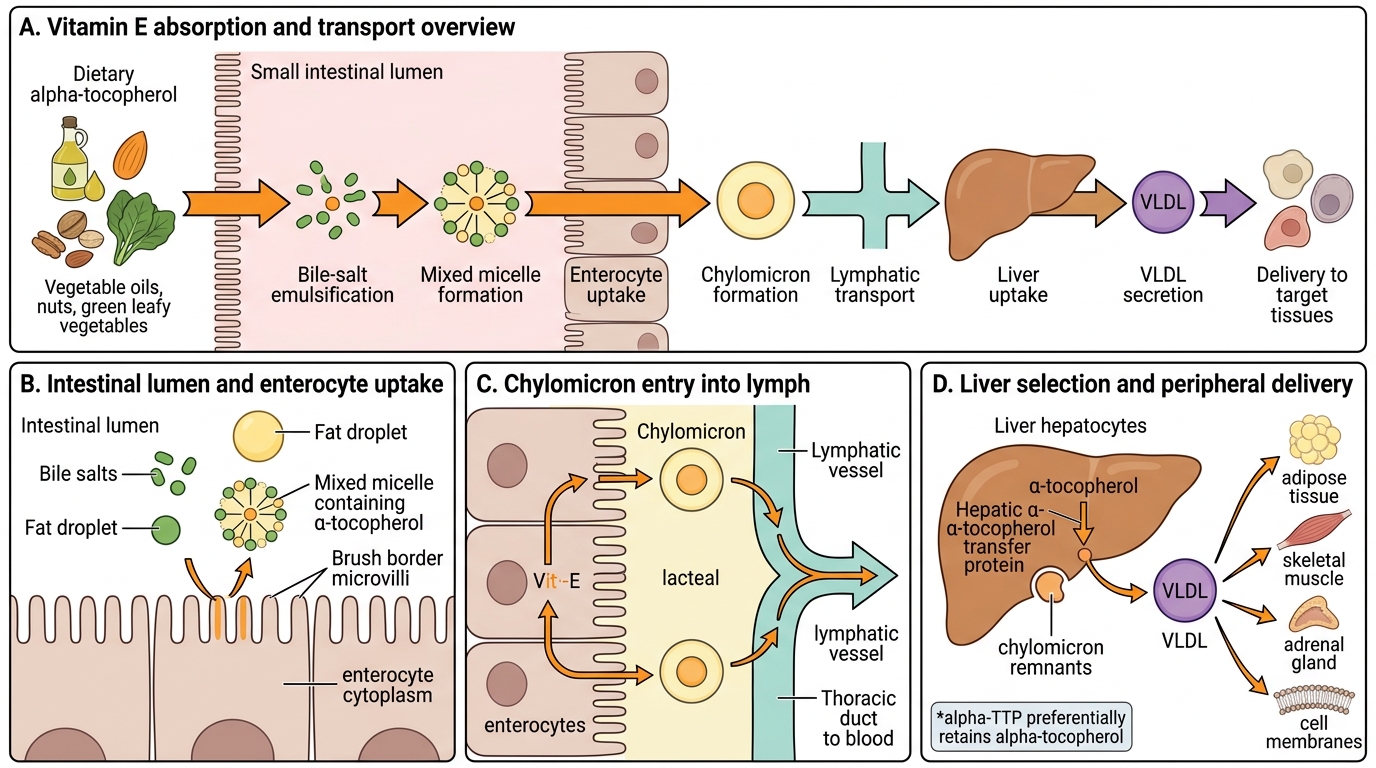
Vitamin E Absorption and Transport Pathway
Vitamin E — Sources, RDA and Absorption
The richest dietary sources of Vitamin E are vegetable and seed oils — wheat germ oil (highest), sunflower oil, safflower oil, and corn oil. Other significant sources include nuts and seeds (almonds, sunflower seeds, hazelnuts), green leafy vegetables (spinach, broccoli), and fortified cereals. Animal-source foods contain relatively little Vitamin E. Breast milk provides adequate Vitamin E for term infants; formula is typically fortified. The recommended dietary intake (ICMR) is approximately 6 mg alpha-tocopherol equivalents per day for children aged 1–3 years, increasing to 7–10 mg/day for older children, with adults requiring 7.5–10 mg/day.
Absorption follows the fat-soluble vitamin pathway: dietary Vitamin E requires bile salts for micellar solubilisation in the intestinal lumen, absorption across the brush border of enterocytes, incorporation into chylomicrons, transport via lymphatics, and delivery to the liver. The liver packages Vitamin E preferentially as alpha-tocopherol into VLDL for peripheral delivery. The preferential selection of alpha-tocopherol by the hepatic alpha-tocopherol transfer protein (alpha-TTP) explains why this is the dominant tissue form despite other tocopherols being present in the diet.
Key points for absorption adequacy:
• Adequate dietary fat required (fat-free diets impair absorption)
• Functional bile salts required (cholestasis causes deficiency)
• Intact enterocytes required (short bowel, coeliac disease impair absorption)
• Chylomicron assembly required (abetalipoproteinaemia — genetic defect in apolipoprotein B — completely blocks this step, causing severe deficiency)
SELF-CHECK
A 10-year-old child with known abetalipoproteinaemia develops progressive difficulty walking, loss of reflexes, and visual disturbance. Which pathophysiological mechanism best explains these neurological features?
A. Chronic Vitamin E deficiency causing lipid peroxidation of myelin sheaths and spinocerebellar tract neurons, leading to demyelination and axonal degeneration
B. Vitamin A deficiency from fat malabsorption causing retinal degeneration and peripheral nerve xerosis
C. Hypocalcaemia from Vitamin D deficiency causing peripheral nerve hyperexcitability and tetany
D. Iron deficiency anaemia from fat malabsorption causing cerebral hypoxia and cerebellar dysfunction
Reveal Answer
Answer: A. Chronic Vitamin E deficiency causing lipid peroxidation of myelin sheaths and spinocerebellar tract neurons, leading to demyelination and axonal degeneration
In abetalipoproteinaemia, failure of chylomicron assembly blocks fat-soluble vitamin absorption, causing severe Vitamin E deficiency. Without alpha-tocopherol to neutralise lipid peroxyl radicals, unsaturated fatty acids in the myelin sheaths of peripheral nerves and in spinocerebellar tract neurons are progressively destroyed by lipid peroxidation. This leads to a characteristic syndrome: spinocerebellar ataxia, areflexia, loss of vibration/proprioception, and pigmentary retinopathy. Early treatment with large doses of Vitamin E (in water-soluble form) can halt but not reverse established neurological damage.
Antioxidant Mechanism and Functions of Vitamin E
The primary function of Vitamin E is to serve as a chain-breaking antioxidant in cell membranes. To understand why deficiency causes the specific clinical syndromes seen in paediatric practice, it is essential to understand the mechanism at the molecular level — this transforms the clinical features from a memorised list into a logical deduction.
Lipid peroxidation and its consequences: Reactive oxygen species (ROS) — principally superoxide radical, hydroxyl radical, and hydrogen peroxide — attack the carbon-carbon double bonds of polyunsaturated fatty acids (PUFAs) in membrane phospholipids. This initiates a chain reaction of lipid peroxidation: each lipid peroxyl radical (L-OO•) abstracts a hydrogen from an adjacent PUFA, generating a new radical in a propagating cascade. Unchecked lipid peroxidation destroys the fluidity and structural integrity of the cell membrane, ultimately leading to cell lysis.
Vitamin E's interruption of the chain: Alpha-tocopherol is embedded in the phospholipid bilayer, positioned precisely to encounter lipid peroxyl radicals as they form. It donates a hydrogen atom (H•) to the peroxyl radical, converting it to a stable lipid hydroperoxide and generating a tocopheroxyl radical (vitamin E•). The tocopheroxyl radical is relatively stable (it does not propagate the chain) and can be regenerated to active Vitamin E by Vitamin C (ascorbic acid) in the aqueous phase — explaining the synergism between Vitamins C and E in antioxidant defence.
Why specific tissues are most vulnerable in deficiency:
• Red blood cells — have high PUFA content in their membranes and are continuously exposed to oxygen; in premature infants, concurrent iron supplementation generates hydroxyl radicals (Fenton reaction), accelerating membrane peroxidation → haemolytic anaemia
• Peripheral nerve myelin — myelin sheaths are lipid-rich; peroxidation leads to progressive demyelination → peripheral neuropathy (loss of vibration sense, areflexia)
• Spinocerebellar tracts — axons in the posterior columns and cerebellar pathways are highly sensitive → spinocerebellar ataxia
• Retinal photoreceptors — outer segments contain the highest PUFA concentration of any tissue → pigmentary retinopathy
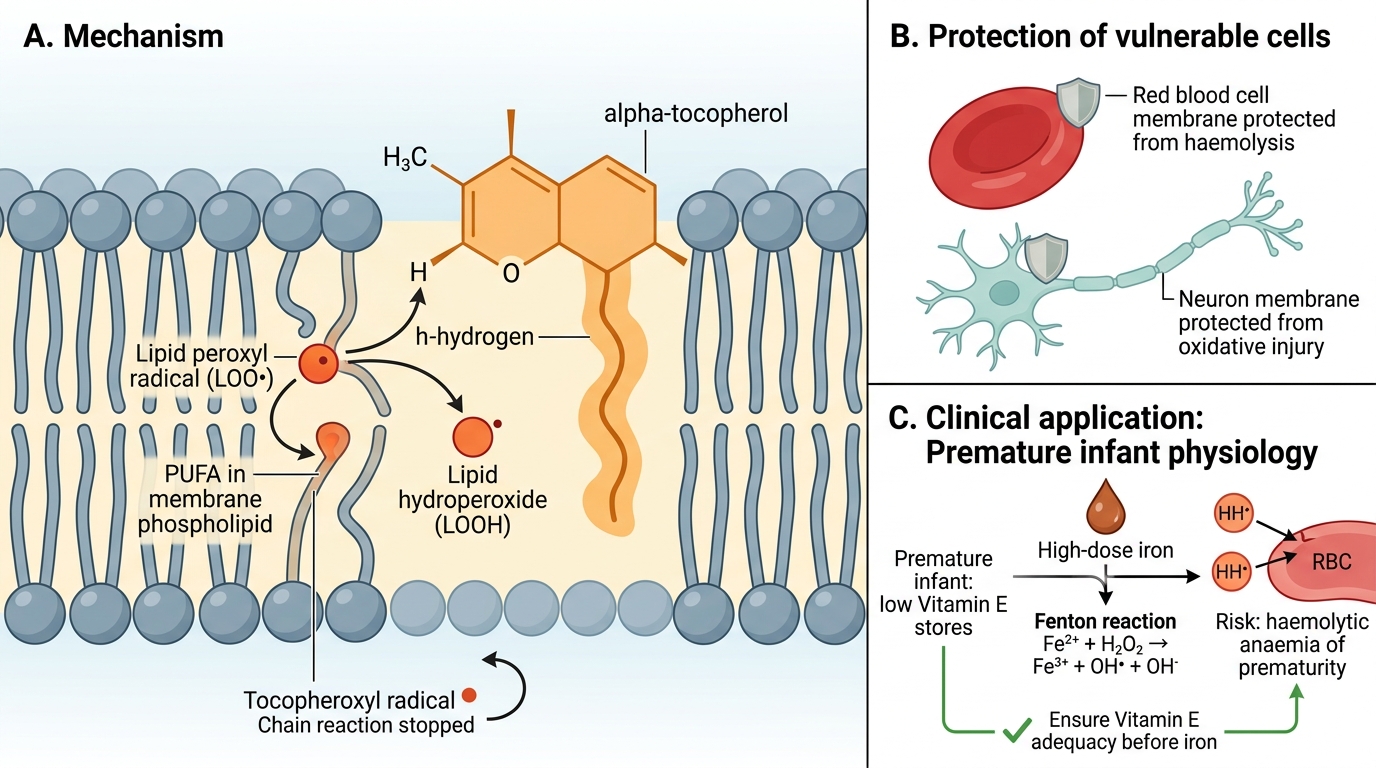
Vitamin E Terminates Membrane Lipid Peroxidation
CLINICAL PEARL
Never give high-dose iron supplementation to a premature infant without ensuring adequate Vitamin E status. Iron generates hydroxyl radicals via the Fenton reaction (Fe²⁺ + H₂O₂ → Fe³⁺ + OH• + OH⁻), which directly attack red cell membranes. In the premature infant with low Vitamin E stores, this combination is the classic trigger for haemolytic anaemia of prematurity. Standard neonatal practice in most centres delays or reduces iron supplementation until Vitamin E stores are adequate (usually after 2–4 weeks of vitamin supplementation), or gives Vitamin E concurrently.