Page 8 of 33
PE12.4 | Vitamin E — SDL Guide (Part 2)
Causes, Clinical Features and Diagnosis of Vitamin E Deficiency
Vitamin E deficiency in paediatric practice manifests through two distinct clinical syndromes, each driven by different underlying mechanisms. Understanding both syndromes — and their relationship to the antioxidant function of Vitamin E — allows the clinician to diagnose them accurately and initiate treatment before irreversible damage occurs. The two groups differ importantly in their age of onset, presenting features, and potential for recovery, which has implications for both the urgency and the approach to management. It is worth emphasising that these syndromes are virtually never seen in healthy, well-nourished term children — the clinical suspicion should be triggered specifically by the presence of prematurity or a documented fat malabsorption disorder, not by non-specific symptoms in the general paediatric population.
Provided image
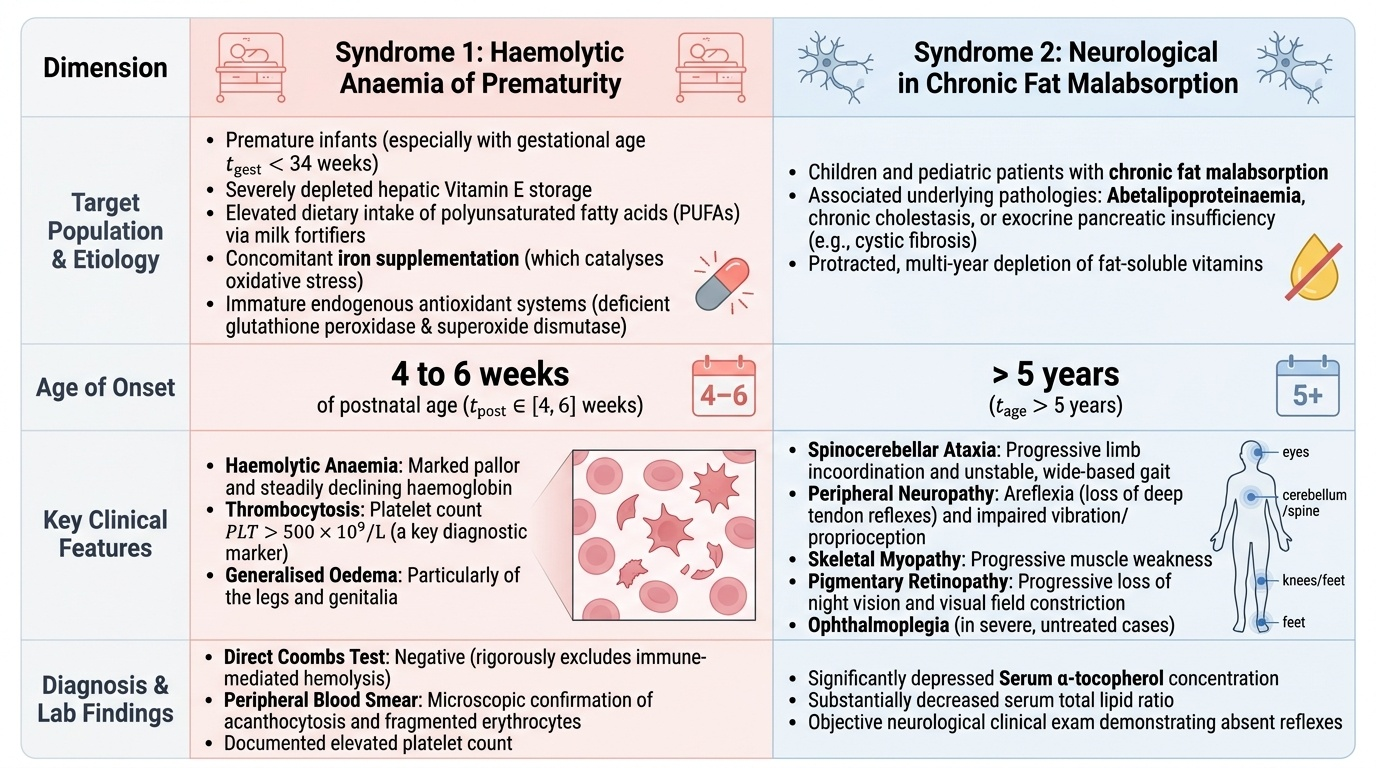
Syndrome 1: Haemolytic anaemia of prematurity (Vitamin E deficiency in premature infants)
Premature infants (especially <34 weeks gestation) have:
• Low hepatic Vitamin E stores (third-trimester placental transfer not completed)
• Relatively high intake of polyunsaturated fatty acids in human milk fortifiers
• Often receive supplemental iron (which generates oxidative stress)
• Immature glutathione peroxidase and superoxide dismutase systems
Clinical features (typically at 4–6 weeks of postnatal age):
• Haemolytic anaemia: pallor, falling haemoglobin; peripheral smear shows acanthocytes and fragmented red cells
• Thrombocytosis: elevated platelet count (>500 × 10⁹/L) — a useful marker
• Generalised oedema: particularly of the legs and genitalia
• Direct Coombs test is negative (not immune-mediated)
Syndrome 2: Neurological degeneration in chronic fat malabsorption
In children with abetalipoproteinaemia, chronic cholestasis, or exocrine pancreatic insufficiency, years of fat malabsorption lead to progressive Vitamin E depletion. The neurological syndrome typically begins after age 5 years if untreated:
• Spinocerebellar ataxia: progressive incoordination, gait disturbance
• Peripheral neuropathy: loss of deep tendon reflexes (areflexia), loss of vibration and proprioception
• Skeletal muscle weakness (myopathy)
• Pigmentary retinopathy: loss of night vision, eventual visual field loss
• Ophthalmoplegia in severe abetalipoproteinaemia
Diagnosis:
• Serum alpha-tocopherol (normal 5–12 mg/L; deficiency <3.5 mg/L in children; in preterm, levels <3.5 mg/L with clinical features are diagnostic)
• Serum tocopherol/total lipid ratio preferred (as hyperlipidaemia falsely elevates absolute tocopherol)
• Peripheral smear: acanthocytes (spiky red cells) in abetalipoproteinaemia; fragmented cells in haemolytic anaemia of prematurity
SELF-CHECK
A premature infant (28 weeks gestation) at 5 weeks of age develops haemolytic anaemia with thrombocytosis. Direct Coombs test is negative. The attending paediatrician suspects Vitamin E deficiency haemolytic anaemia. Which concurrent supplement may have exacerbated the haemolysis in this infant?
A. Iron supplementation (generates hydroxyl radicals via Fenton reaction, oxidising red cell membrane lipids)
B. Vitamin D supplementation (causes hypercalcaemia, which disrupts red cell membranes)
C. Vitamin A supplementation (competes with Vitamin E for chylomicron transport)
D. Calcium supplementation (causes membrane rigidity through calcium overload)
Reveal Answer
Answer: A. Iron supplementation (generates hydroxyl radicals via Fenton reaction, oxidising red cell membrane lipids)
Iron in the ferrous form (Fe²⁺) reacts with hydrogen peroxide in the Fenton reaction to generate highly reactive hydroxyl radicals. In a premature infant with low Vitamin E stores, these radicals attack the unsaturated fatty acids in red cell membranes, causing oxidative haemolysis. This is the classic mechanism of haemolytic anaemia of prematurity when iron supplementation is introduced before adequate Vitamin E is established. Standard practice is to supplement Vitamin E from birth in premature infants to protect against this.
Management of Vitamin E Deficiency
The management of Vitamin E deficiency depends critically on whether the underlying problem is nutritional deficiency in a premature infant or fat malabsorption in an older child, because the two groups require different supplementation approaches. In both cases, however, the core principle is the same: restore tissue Vitamin E levels to protect cell membranes from ongoing oxidative damage, and address the underlying cause where possible. A key practical consideration is that standard oral alpha-tocopherol requires bile for absorption — in patients with fat malabsorption, the water-soluble form of Vitamin E (tocopherol polyethylene glycol succinate, TPGS) is necessary for reliable absorption. Timing matters: for the neurological syndrome of fat malabsorption, intervention before the onset of ataxia and neuropathy can prevent these deficits entirely, whereas treatment after their onset can only arrest but not reverse established neurological damage.
Treatment of Vitamin E deficiency in premature infants:
• Oral alpha-tocopherol (water-soluble formulation): 25 IU/day starting from the first days of life for all premature infants <34 weeks gestation
• In established haemolytic anaemia: therapeutic doses of 100 IU/day, with concurrent iron dose reduction or suspension until haemolysis resolves
• Do not give high-dose iron until Vitamin E status is adequate
• Transfuse if haemoglobin critically low with symptoms
Treatment of Vitamin E deficiency in fat malabsorption:
• Water-soluble Vitamin E (TPGS): the standard oral alpha-tocopherol capsule is poorly absorbed when bile is absent; TPGS is absorbed by a bile-independent mechanism
• Doses: 15–25 IU/kg/day for abetalipoproteinaemia; dose varies by condition and severity
• Neurological damage from chronic deficiency may be irreversible — early supplementation before neurological symptoms appear is critical
• Treat the underlying cause (e.g., ursodeoxycholic acid for cholestasis; pancreatic enzyme replacement for exocrine pancreatic insufficiency in CF)
| Group | Form | Dose | Goal |
|---|---|---|---|
| Premature infant (<34 wk) | Water-soluble oral | 25 IU/day from birth | Prevent haemolytic anaemia |
| Fat malabsorption (abetalipoproteinaemia, cholestasis) | TPGS (water-soluble) | 15–25 IU/kg/day | Prevent/halt neurological degeneration |
| Healthy term infant | Formula or breast milk | Adequate diet | No supplementation needed |
Self-Assessment
Returning to the opening case: the 30-week premature infant at 5 weeks of age has haemolytic anaemia of prematurity due to Vitamin E deficiency. The negative Coombs test excludes immune-mediated causes (ABO incompatibility, Rh disease). The thrombocytosis (720 × 10⁹/L) and oedema complete the classic triad. The acanthocytes on peripheral smear reflect the oxidative membrane damage. Iron supplementation initiated at week 2 is the exacerbating factor — iron generates hydroxyl radicals via the Fenton reaction, which attacked the already-vulnerable Vitamin E-depleted red cell membranes. This case also illustrates the importance of routine Vitamin E prophylaxis from birth in premature infants — a preventable complication that occurred because supplementation was not initiated at delivery. Had the infant received 25 IU/day of oral water-soluble Vitamin E from the first days of life, the antioxidant protection would have been sufficient to prevent haemolysis even when iron supplementation was started.
Immediate management:
• Reduce or suspend iron supplementation
• Initiate oral water-soluble Vitamin E (alpha-tocopherol) at therapeutic dose
• Transfuse packed red cells if symptomatic anaemia requires it
• From birth in all premature infants: prophylactic Vitamin E 25 IU/day
Key examination recall points:
• Vitamin E deficiency in preterm infants → haemolytic anaemia + thrombocytosis + oedema (4–6 weeks of life)
• Aggravated by iron supplementation (Fenton reaction → hydroxyl radicals)
• Vitamin E deficiency in fat malabsorption → spinocerebellar ataxia + peripheral neuropathy + retinopathy
• Neurological damage in chronic deficiency may be irreversible
• Abetalipoproteinaemia = failure of apolipoprotein B synthesis → no chylomicrons → severe fat-soluble vitamin deficiency
• Water-soluble Vitamin E (TPGS) required for absorption in cholestasis/malabsorption
• Diagnosis: serum alpha-tocopherol <3.5 mg/L (children)
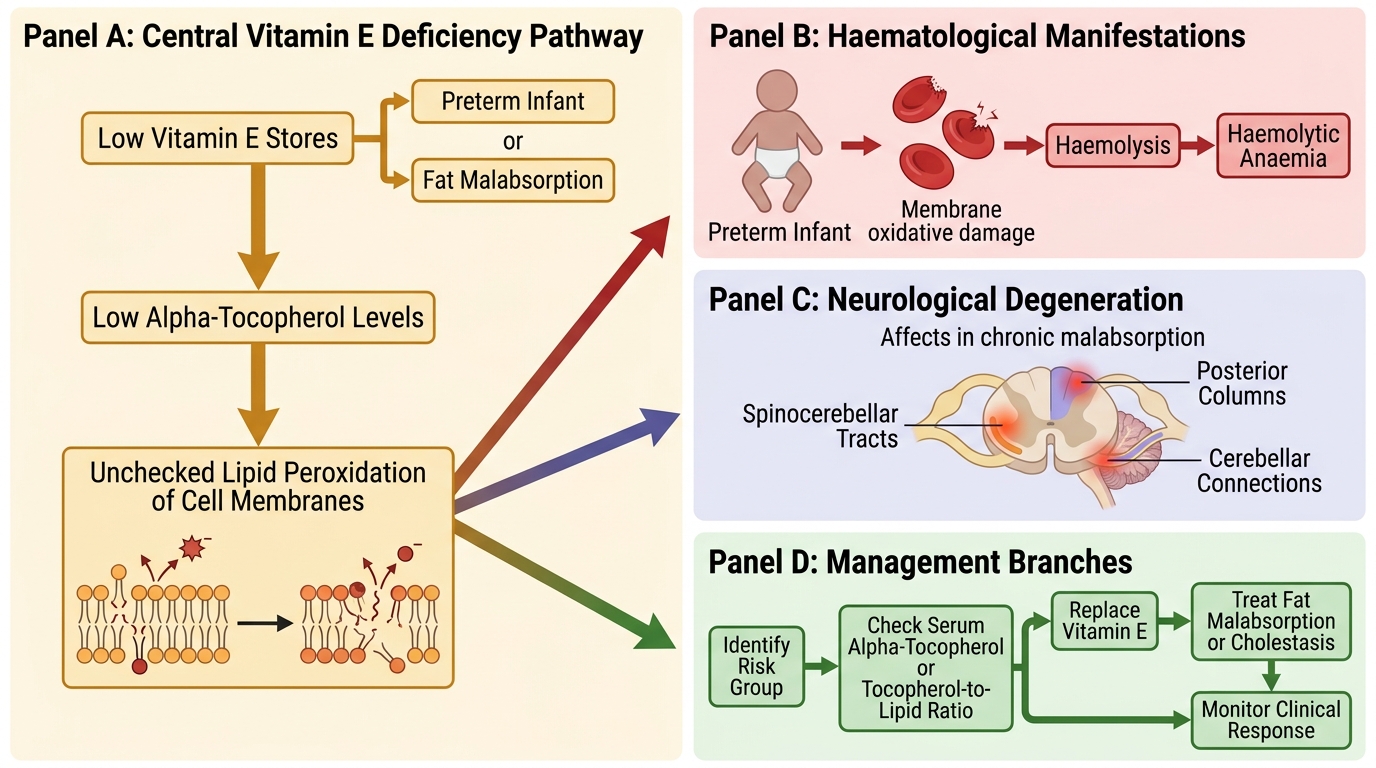
Vitamin E Deficiency: Pathway and Management