Page 1 of 20
PE16.1 | IMNCI Framework — SDL Guide
Learning Objectives
- Explain the rationale behind the Integrated Management of Neonatal and Childhood Illnesses (IMNCI) strategy in the Indian public health context
- Describe the three components of the IMNCI programme
- Outline the IMNCI case-management algorithm including the two age bands
- Explain the colour-coded triage system (pink/yellow/green) and the principle of risk stratification
- Describe the HBNC and HBPNC visit schedules and the role of community health workers
- Discuss the evidence for IMNCI's impact on neonatal and under-5 mortality in India
INSTRUCTIONS
India bears one of the world's heaviest burdens of neonatal and under-5 mortality, and a large proportion of these deaths occur at home or in peripheral health facilities where a systematic, integrated approach to sick-child assessment can be life-saving. The IMNCI strategy equips every frontline health worker — from MBBS physicians to ASHAs — with a standardised algorithm that prevents the common trap of treating only the presenting complaint while missing co-existing, equally dangerous conditions. As a final-year student about to enter practice in community and district hospital settings, mastering the IMNCI framework is not optional: it is the operational backbone of child survival in India.
References
- Ghai Essential Pediatrics, 9th edition, Ch 5 (Child Survival) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 22 (Global Child Health) (textbook)
- MoHFW India — IMNCI Training Modules (Revised), 2003 and subsequent updates (guideline)
- WHO — IMCI Chart Booklet, 2014 (guideline)
- MoHFW India — HBNC Programme Guidelines (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 10 pm at a rural sub-centre in Rajasthan. A 28-year-old mother arrives carrying her seven-month-old son. The child is hot, not feeding well, and has had loose stools for two days. The nearest paediatric unit is 45 km away. You are the duty medical officer — a fresh MBBS graduate. Do you send the child immediately? Wait and observe? Treat at the facility? The correct answer depends on a rapid, systematic appraisal of this child using the IMNCI assess-classify-treat algorithm. Without that framework, a child with severe dehydration and impending shock may be sent home with ORS, while an anxious mother with a mildly ill child may trigger an unnecessary night transfer. IMNCI gives you the decision logic to act correctly in exactly this situation.
WHY THIS MATTERS
India accounted for approximately 24% of global neonatal deaths and a significant share of under-5 deaths as recently as 2019. A majority of these deaths occur in the neonatal period and in children under two years, and are caused by a small set of preventable and treatable conditions — pneumonia, diarrhoea, malaria, malnutrition, and neonatal infections. The IMNCI strategy directly addresses this mortality burden by standardising the way sick children are assessed and managed at every level of the health system, from the ASHA's home visit to the primary health centre. For any physician practising in India — especially in community medicine, paediatrics, or general practice — IMNCI is a non-negotiable competency that is tested in NMC exit examinations and applied daily in district hospitals and PHCs.
RECALL
Before engaging with IMNCI, activate the following prior knowledge:
- Developmental milestones: social smile ~6–8 weeks; neck control ~3 months; sits without support ~6–8 months; stands with support ~9–12 months — because IMNCI flags developmental delay as a risk factor.
- Breastfeeding physiology (from PY): colostrum composition and the let-down reflex; IMNCI counselling reinforces exclusive breastfeeding as the primary preventive intervention for newborns.
- National Immunization Schedule (NIS): BCG + OPV-0 + Hep-B at birth; pentavalent/OPV/IPV/rotavirus at 6/10/14 weeks; MR at 9–12 months — IMNCI integrates immunisation checking into every sick-child visit.
- Basic pathophysiology of dehydration: from PY — the clinical signs that correlate with mild, moderate, and severe dehydration map directly onto IMNCI's no-dehydration / some-dehydration / severe-dehydration classification.
Introduction: What Is IMNCI and Why Does It Matter?
IMNCI — Integrated Management of Neonatal and Childhood Illnesses — is a clinical and public-health strategy developed jointly by the World Health Organization (WHO) and UNICEF in the 1990s and adapted for India by the Ministry of Health and Family Welfare (MoHFW) as IMNCI, adding the explicit 'N' for neonatal to emphasise the critical first 28 days of life. The strategy addresses children from birth to five years of age, covering the full window in which preventable childhood mortality is concentrated.
Before IMNCI, illness management in peripheral Indian facilities was often single-disease oriented — a child with fever was treated for malaria or tested for typhoid; a child with cough was given antibiotics empirically. This siloed approach meant that a child presenting with cough who also had severe dehydration, undernutrition, and an incomplete immunisation history might receive only a cough syrup and be discharged — all three co-existing life-threatening problems unaddressed. IMNCI was designed precisely to solve this fragmentation: it asks the health worker to assess the child for ALL major conditions simultaneously using a standardised checklist, classify each finding using a colour-coded triage, and treat (or refer) based on the most severe classification found.
For the Indian MBBS graduate, IMNCI competency is operationally critical: it is embedded in MoHFW training, tested in national-level exit examinations, and is the mandated framework for sick-child management in PHCs, community health centres, and district hospitals under the National Health Mission.
Global and Indian Burden of Neonatal and Under-5 Mortality
The global under-5 mortality rate (U5MR) fell from 93 per 1,000 live births in 1990 to approximately 37 per 1,000 live births in 2020 — a remarkable achievement, but one that masks persisting geographic inequality. India's U5MR declined from around 126 per 1,000 live births in 1990 to approximately 32 per 1,000 live births in 2020, tracking the Sustainable Development Goal (SDG) target of ≤25 per 1,000 live births by 2030, though still above that target. Neonatal mortality — deaths in the first 28 days of life — accounts for nearly 45% of all under-5 deaths globally, and India contributes the largest absolute number of neonatal deaths of any single country.
The causes of this mortality are highly concentrated: pneumonia, diarrhoeal diseases (with dehydration), neonatal sepsis, birth asphyxia, prematurity, and severe acute malnutrition account for the vast majority of preventable deaths. Crucially, most of these deaths occur in the home or at peripheral facilities where no specialist paediatrician is available. This epidemiological reality is the direct justification for IMNCI: the intervention must be deliverable by a non-specialist — a general duty medical officer, a nurse, or a trained community health worker — at the point of first contact.
- Neonatal Mortality Rate (NMR): India ~20 per 1,000 live births (SRS 2020) — SDG target ≤12.
- Infant Mortality Rate (IMR): India ~28 per 1,000 live births (SRS 2020).
- Under-5 Mortality Rate (U5MR): India ~32 per 1,000 live births (SRS 2020).
- Leading causes in neonates: prematurity, sepsis/infections, birth asphyxia.
- Leading causes age 1 month–5 years: pneumonia, diarrhoea, malnutrition, vaccine-preventable diseases.
IMPORTANT CONTEXTUAL NOTE: The IMNCI approach specifically targets the high-burden age band (neonates to 5-year-olds) and the high-burden conditions where standardised assessment can reduce the delay in appropriate referral and treatment.
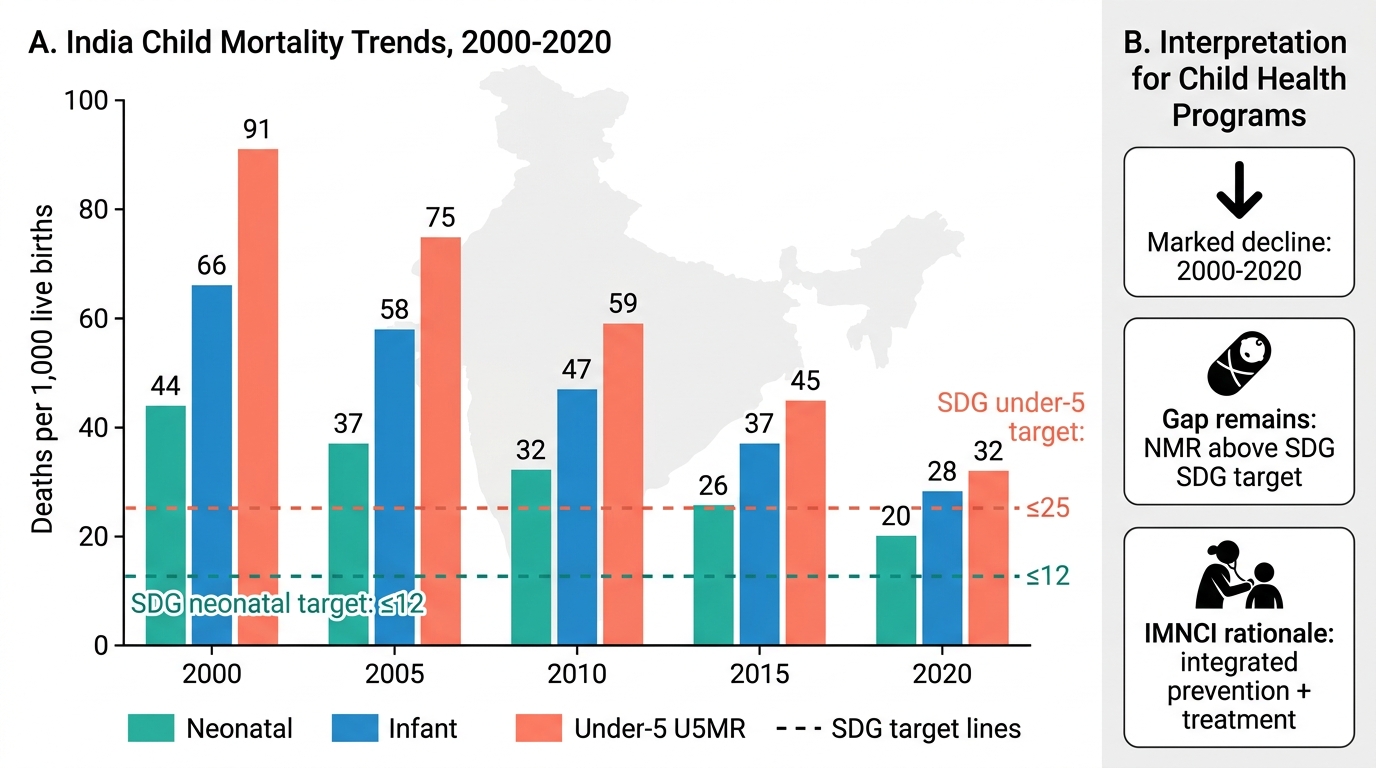
India Child Mortality Trends and SDG Targets
Why Integrated Management? Rationale and Origins of IMNCI
The conceptual foundation of IMNCI rests on four key insights from child-survival research conducted in the 1980s and 1990s, which collectively revealed why disease-specific vertical programmes, though each individually effective, could not alone reduce overall child mortality to the desired level.
First, overlapping morbidity is the rule, not the exception: a field study in Bangladesh found that over 60% of children attending health facilities had more than one illness at presentation. A child assessed only for the presenting complaint of fever would miss co-existing pneumonia, dehydration, or severe malnutrition — all of which independently increase case fatality. Second, the single-disease clinical algorithm (e.g., a malaria diagnostic pathway or a diarrhoea-ORS pathway) trained health workers to look for only one condition, creating systematic blind spots. Third, the untrained eye under-detects severity: studies in primary-care settings showed that health workers without structured assessment tools missed danger signs such as inability to feed, sternal indrawing, and impaired consciousness in a large proportion of seriously ill children. Fourth, and critically, preventive and curative care were siloed: a child presenting to a health worker with fever had their immunisation status and nutritional status unassessed — opportunities for vaccination, nutrition counselling, and micronutrient supplementation were consistently lost.
The WHO and UNICEF responded in the early 1990s with the IMCI strategy (Integrated Management of Childhood Illness), validated through the WHO Multi-Country Evaluation of IMCI (MCE/IMCI) study in five countries — Bangladesh, Brazil, Peru, Tanzania, and Uganda — published in The Lancet in 2001. The MCE demonstrated that IMCI significantly reduced the risk of child death in the communities where it was fully implemented, particularly through improvements in the quality of case management at facility level. India adapted the strategy as IMNCI, extending the algorithm explicitly into the neonatal period (first 28 days), recognising that India's neonatal mortality was proportionately higher than the global average and that the original IMCI strategy's focus on 2 months and older was leaving the most vulnerable period uncovered.
IMNCI in India is thus both a case-management tool for health workers and a quality-improvement framework for peripheral health systems.