Page 2 of 20
PE16.1 | IMNCI Framework — SDL Guide (Part 2)
Components of the IMNCI Strategy
The IMNCI strategy is built on three interlocking components, each addressing a different level of the health system. No single component works in isolation — child survival improvements documented in the MCE occurred only in sites where all three were functioning simultaneously.
Component 1: Improvement in the case-management skills of health workers is the clinical core. Health workers — doctors, nurses, ANMs, and paramedics — are trained to assess, classify, and treat children using the IMNCI chart booklet, which codifies danger-sign recognition, illness classification using colour-coded triage, standardised treatment protocols, and counselling of caregivers. Training addresses both the young infant (birth to <2 months) and the older child (2 months to 5 years) using separate algorithm charts for each age band. Pre-service and in-service training are both mandated.
Component 2: Strengthening the health system focuses on ensuring that the conditions for quality case management exist — adequate drug supply (ORS, zinc, oral amoxicillin, first-line antipyretics), functioning referral pathways, cold-chain maintenance for immunisation, and supervisory systems. Without reliable drug supply and a functioning referral system, even well-trained workers cannot implement IMNCI recommendations.
Component 3: Improving family and community practices addresses the demand side of child health — caregiver knowledge of danger signs, timely care-seeking behaviour, appropriate home management of mild illness (fluid replacement, continued breastfeeding), compliance with immunisation schedules, and nutrition practices. In India, this component is largely delivered by ASHAs (Accredited Social Health Activists) and Anganwadi Workers (AWWs) through home visits, village health and nutrition days, and community counselling.
| Component | Level | Key mechanism |
|---|---|---|
| Case-management skills | Facility (PHC, CHC, DH) | IMNCI training for health workers |
| Health system strengthening | Facility + district | Drug supply, referral, supervision |
| Family and community practices | Community | ASHA/AWW counselling, HBNC visits |
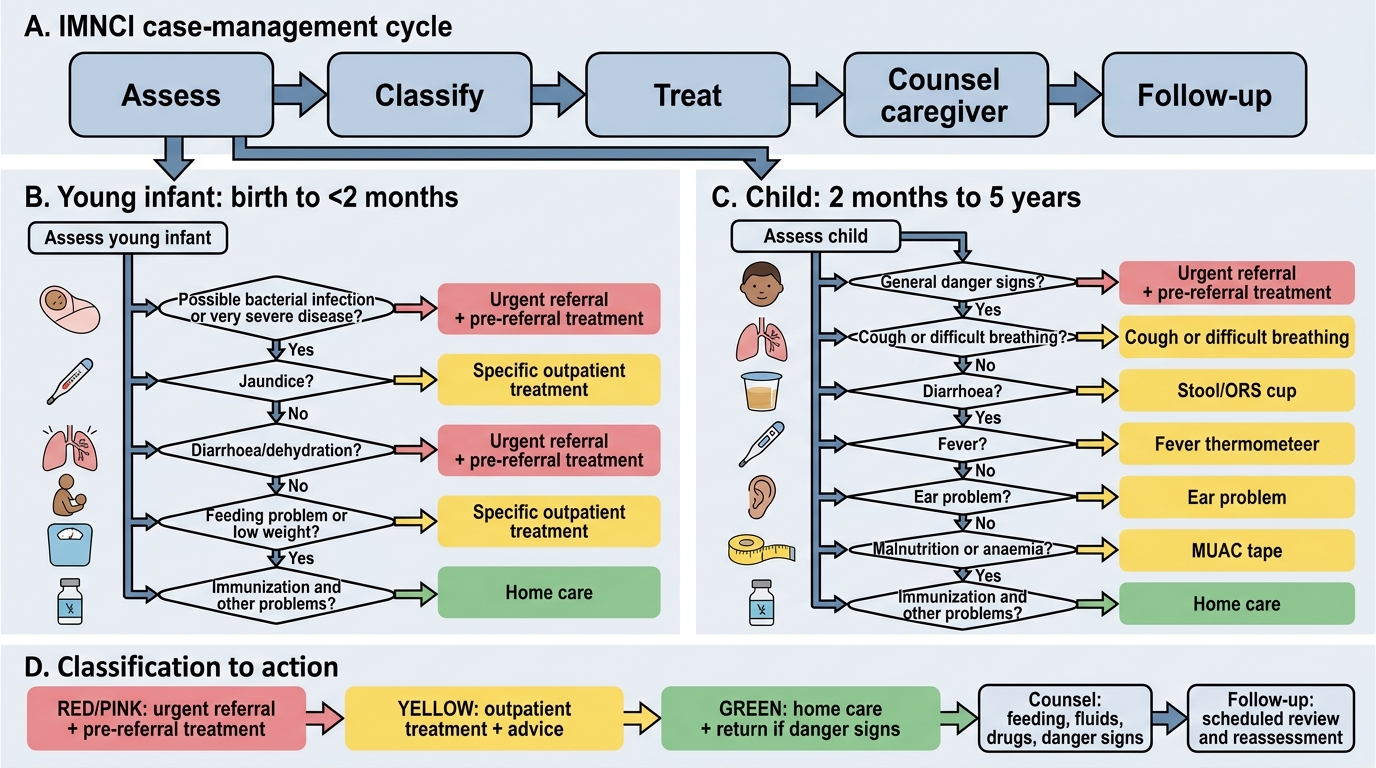
IMNCI Case-Management Algorithm: Assess-Classify-Treat
The clinical heart of IMNCI is the assess-classify-treat-counsel-follow-up algorithm, which forces a systematic, head-to-toe appraisal of the sick child rather than a symptom-focused consultation. The algorithm is organised into two age-specific chart booklets because the danger signs, clinical patterns, and management differ significantly between neonates/young infants and older children.
For the young infant (birth to <2 months), the algorithm checks for: bacterial infection (fast breathing ≥60/min, severe chest indrawing, umbilical redness/discharge, skin pustules, hypothermia, jaundice, feeding problems), low birth weight, diarrhoea, and immunisation/vitamin-K status. The focus is on recognising sepsis and pneumonia early — two conditions that can deteriorate from mild to fatal within hours at this age.
For the child 2 months to 5 years, the algorithm sequentially evaluates: general danger signs (inability to drink/breastfeed, vomiting everything, convulsions, lethargy/unconscious) → main presenting symptoms (cough/breathing, diarrhoea, fever, ear problems) → nutritional status (weight-for-age, MUAC, bilateral pedal oedema) → immunisation status → any other problems. Each category is classified using the colour-coded triage system.
The algorithm is deliberately structured so that general danger signs are elicited first — if any danger sign is present, the child is immediately classified as 'pink' (urgent referral) regardless of the severity of the presenting complaint. This prevents the common error of classifying a child as 'yellow' for a moderate illness while missing the danger sign that indicates a life-threatening condition.
Key danger signs — 2 months to 5 years (memorise these exactly):
• Unable to drink or breastfeed
• Vomits everything
• Convulsions (current or history)
• Lethargic or unconscious
The respiratory rate cut-offs for fast breathing (a proxy for pneumonia) are age-specific and are among the most commonly tested IMNCI thresholds:
• <2 months: ≥60 breaths/minute
• 2–11 months: ≥50 breaths/minute
• 12–59 months: ≥40 breaths/minute
| Feature assessed | Age <2 months | Age 2 months–5 years |
|---|---|---|
| Fast breathing threshold | ≥60/min | ≥50/min (2-11 mo), ≥40/min (12-59 mo) |
| Danger sign for feeding | Cannot feed at all | Cannot drink/breastfeed |
| Severe chest indrawing | Yes — severe bacterial infection | Yes — severe pneumonia |
| MUAC cut-off (SAM) | N/A (MUAC unreliable <6 mo) | <11.5 cm (6-59 mo) |
IMNCI Assess-Classify-Treat Algorithm
SELF-CHECK
A 9-month-old child presents with cough and fast breathing (52 breaths/min). He is alert, drinking well, and has no chest indrawing. According to IMNCI, which colour triage category does this child fall into?
A. Pink — refer urgently because respiratory rate is elevated
B. Yellow — pneumonia, treat with oral amoxicillin at the facility/PHC level
C. Green — no pneumonia, treat with home remedies and follow-up
D. Pink — danger sign of lethargy present
Reveal Answer
Answer: B. Yellow — pneumonia, treat with oral amoxicillin at the facility/PHC level
At 9 months, fast breathing is ≥50 breaths/min. At 52/min the child meets the fast-breathing threshold, classifying as 'pneumonia'. In the absence of any general danger sign (drinking well, alert, no severe chest indrawing), this is classified YELLOW — treat with oral amoxicillin and advise return if worsening. Pink (urgent referral) requires a general danger sign OR severe chest indrawing. Green (no pneumonia) requires respiratory rate below the threshold.
Risk Stratification and Colour-Coded Triage System
The colour-coded triage system is IMNCI's mechanism for translating clinical findings into actionable management decisions. The three colours — pink, yellow, and green — correspond to increasing urgency and are chosen deliberately to be unambiguous visual cues that even a non-literate community worker can apply after training. Each colour maps to a specific action:
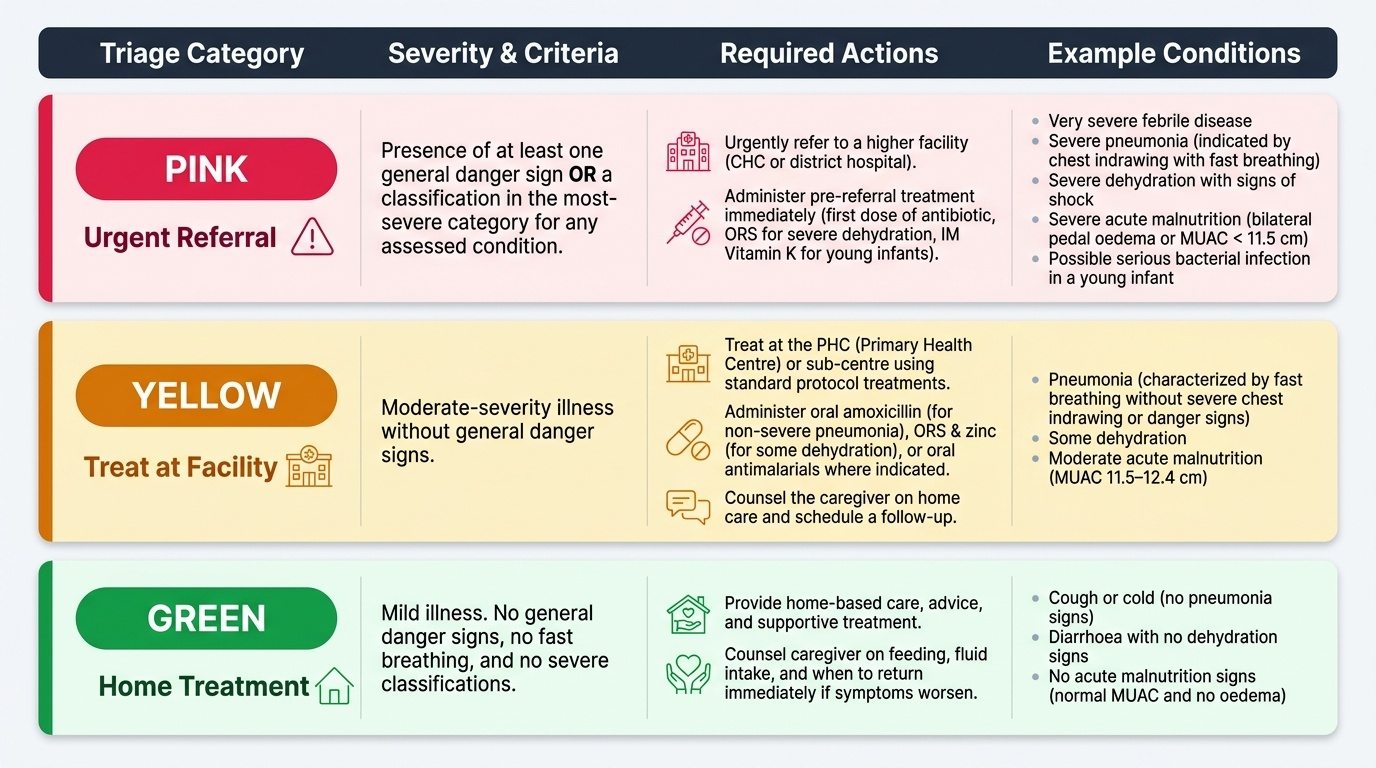
Provided image
Pink (urgent referral): The child has at least one general danger sign OR a classification in the most-severe category for any assessed condition. The appropriate action is to urgently refer to a higher facility (CHC or district hospital), after giving any pre-referral treatment (first dose of antibiotic, ORS for severe dehydration, intramuscular vitamin K for young infants). Examples: very severe febrile disease, severe pneumonia (chest indrawing with fast breathing), severe dehydration with signs of shock, severe malnutrition (bilateral pedal oedema or MUAC <11.5 cm), possible serious bacterial infection in a young infant.
Yellow (treat at facility): The child has a moderate-severity illness without general danger signs. The appropriate action is to treat at the PHC or sub-centre, using standard protocol treatments (oral amoxicillin for non-severe pneumonia, ORS and zinc for some-dehydration diarrhoea, oral antimalarials where indicated), and to counsel the caregiver on follow-up. Examples: pneumonia (fast breathing without severe chest indrawing or danger sign), some dehydration, moderate acute malnutrition (MUAC 11.5–12.4 cm).
Green (home treatment): The child has mild illness without fast breathing, without danger signs, and without significant dehydration or malnutrition. The appropriate action is to treat at home with soothing remedies (for ARI), continue normal feeding, and give specific counselling on when to return. The health worker also uses this visit to check and update immunisation, screen for malnutrition, and counsel on breastfeeding.
The clinical power of this system lies in its override rule: if ANY pink-classification condition is found during the assessment, the final action is pink regardless of what the other conditions show. A child classified as yellow for moderate malnutrition who is subsequently found to have a general danger sign is reclassified as pink — the most severe finding drives the action.
CLINICAL PEARL
The IMNCI override rule saves lives: In a busy PHC, a health worker may assess a child with moderate diarrhoea (yellow) and initially plan oral rehydration. However, if during the general danger-sign check the child is found to be lethargic, the triage immediately escalates to pink — urgent referral with IV fluid pre-referral treatment. Trainees most often miss lethargic or unconscious in a child who is physically still; always actively test responsiveness (call the child's name, touch gently) before classifying. Never assume a quiet child is simply 'resting'. The IMNCI algorithm protects against this cognitive trap by mandating the danger-sign check before any other classification.
SELF-CHECK
A 6-week-old neonate is brought to a sub-centre with fast breathing (64/min), fever, and refusal to feed. The ASHA assessed the baby at home and found axillary temperature of 38.8°C. According to IMNCI young-infant guidelines, what is the most appropriate action?
A. Green — reassure mother and advise paracetamol; review in 2 days
B. Yellow — give oral amoxicillin at the sub-centre and review in 3 days
C. Pink — refer urgently after giving first dose of intramuscular antibiotic
D. Yellow — admit for intravenous fluids and monitor respiratory rate
Reveal Answer
Answer: C. Pink — refer urgently after giving first dose of intramuscular antibiotic
This neonate has fast breathing (≥60/min in <2 months = fast breathing threshold), fever (≥37.5°C axillary), and refusal to feed — this combination classifies as 'possible serious bacterial infection' in the young-infant algorithm. Young infants with possible serious bacterial infection are classified PINK: refer urgently. Pre-referral treatment includes a first dose of intramuscular antibiotic (gentamicin + ampicillin per IMNCI protocol or as per current NHM guidelines) before transfer. Oral amoxicillin alone is inadequate; intravenous admission at a sub-centre is not feasible.