Page 1 of 19
PA30.{1,4} | Benign Breast Disease & Gynecomastia — SDL Guide
Learning Objectives
- Describe the normal microscopic structure of the breast and the hormonal influences that govern it across life stages
- Classify benign breast diseases and explain the etiology and pathogenesis of inflammatory/reactive lesions (acute mastitis, periductal mastitis, fat necrosis)
- Distinguish non-proliferative from proliferative fibrocystic change and quantify carcinoma risk associated with each category
- Describe the gross and microscopic features, hormonal dependence, and clinical behavior of fibroadenoma and intraductal papilloma
- Explain the concept of triple assessment and identify which benign lesions carry increased cancer risk
- Enumerate the causes of gynecomastia, explain the estrogen/androgen imbalance that drives it, and describe its morphology
INSTRUCTIONS
Breast lumps are among the commonest referrals in surgical outpatient clinics. The ability to distinguish a benign from a potentially malignant lesion — and to explain this distinction to a frightened patient — rests on a precise understanding of underlying pathology. This SDL anchors breast pathology in normal structure and hormonal biology, then systematically builds through inflammation, fibrocystic change, benign tumors, and gynecomastia. By the end, you will be able to apply the triple-assessment framework and counsel a patient appropriately.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 23 — The Breast (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 27-year-old woman presents with a well-defined, rubbery, mobile lump in the upper outer quadrant of her left breast. She is terrified — her aunt died of breast cancer. Ultrasound shows a smooth oval hypoechoic mass. Fine-needle aspiration yields sheets of uniform epithelial cells. The pathologist reports: fibroadenoma. She is reassured and discharged. A 45-year-old woman in the same clinic has a dense, lumpy, tender breast with multiple small cysts confirmed on ultrasound. Biopsy shows apocrine metaplasia and focal epithelial hyperplasia with atypia. She is told her risk of future breast cancer is 4–5 times the baseline. Same organ, same complaint — radically different implications. Understanding why requires knowing the pathology.
WHY THIS MATTERS
Benign breast disease accounts for the majority of breast clinic referrals. As a future clinician you will: (1) be the first to examine a breast lump and decide urgency, (2) explain biopsy results to patients, (3) identify which benign diagnoses warrant long-term surveillance. For your examinations, benign breast pathology is a perennial short and long question in Pathology and Surgery papers. Gynecomastia, while a male breast condition, is examined almost every year in the context of endocrine, hepatic, and drug-induced disease.
RECALL
Before we begin, activate your prior knowledge:
- From Anatomy/Histology: the breast is a modified apocrine sweat gland. It is composed of 15–20 lobes, each drained by a lactiferous duct that opens at the nipple. Each lobe subdivides into lobules, each lobule containing a terminal duct lobular unit (TDLU) — the functional and pathological core of most breast disease.
- From Physiology: estrogen drives ductal proliferation; progesterone drives lobular/acinar development. After menopause, both hormone levels fall and breast parenchyma involutes, replaced by fat.
- From Biochemistry: aromatase converts androgens (testosterone, androstenedione) to estrogens (estradiol, estrone). This peripheral conversion is clinically important in gynecomastia, obesity, and liver disease.
- From Pharmacology: recall at least three drug classes that can elevate prolactin or alter the estrogen/androgen ratio — you will need this for gynecomastia.
Normal Breast Structure and Hormonal Influences
The breast is not a static organ — its architecture changes continuously under hormonal control.
Microscopic layers of the TDLU:
• Luminal (inner) epithelial cells — produce milk, express estrogen receptors (ER) and progesterone receptors (PR)
• Myoepithelial (outer) cells — contractile, ER-negative, sit on the basement membrane; their presence confirms a benign lesion (carcinoma destroys this layer)
• Basement membrane — when breached by malignant cells, invasion begins
Stroma types:
• Intralobular stroma — loose, hormone-responsive, surrounds the TDLU
• Interlobular stroma — dense fibrous tissue between lobes; less hormone-responsive
Hormonal cycle:
| Phase | Hormone | Breast effect |
|---|---|---|
| Follicular | Estrogen rises | Ductal proliferation, increased stromal fluid |
| Luteal | Progesterone rises | Lobular acinar budding, edema |
| Menses | Both fall | Apoptosis, involution |
| Pregnancy | Both high + prolactin | Full lobular development, lactation |
| Menopause | Both fall | Lobular atrophy, fatty replacement |
Why this matters: Most benign breast conditions (fibrocystic change, fibroadenoma, gynecomastia) are exaggerations of normal hormonal responses. Recognising the normal architecture helps you identify what has gone wrong.
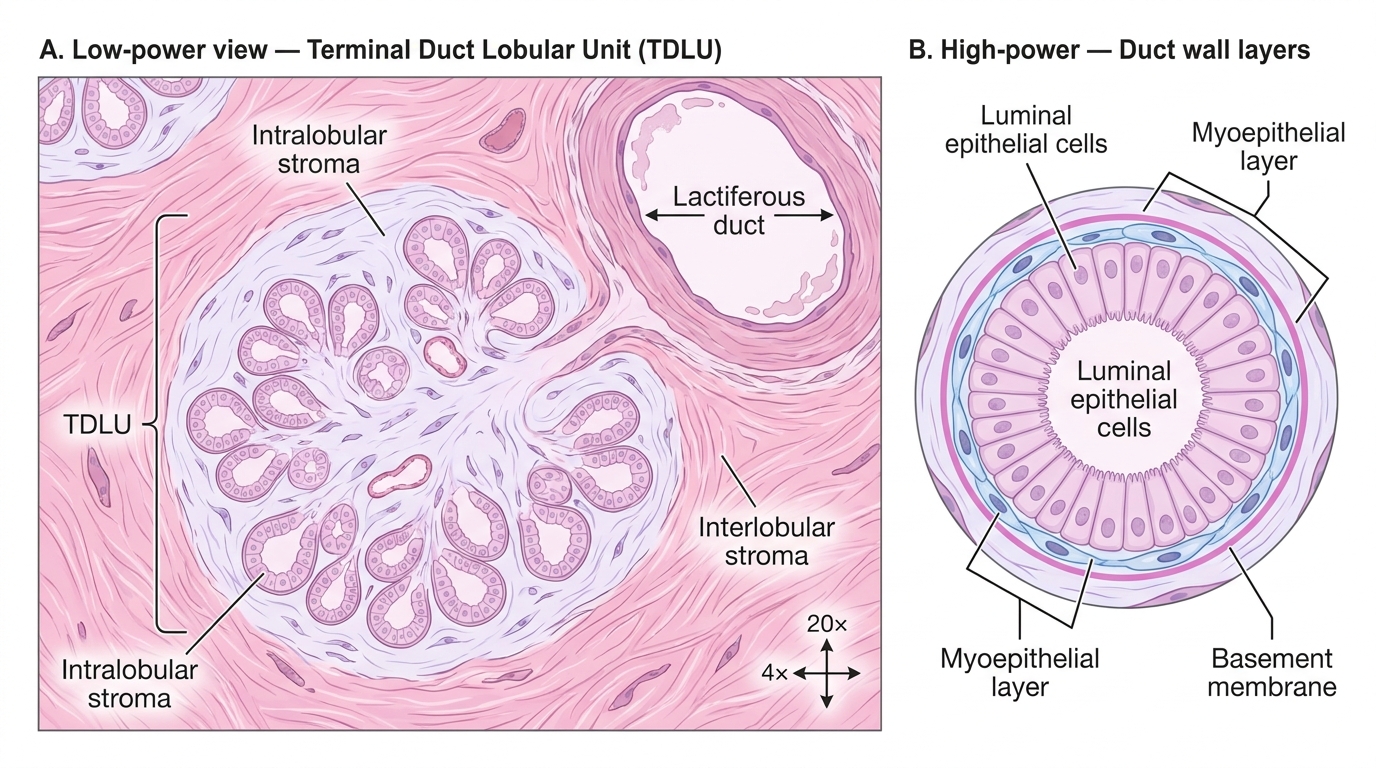
Normal Breast Histology — Terminal Duct Lobular Unit (TDLU)
Inflammatory Conditions — Acute Mastitis and Periductal Mastitis
Acute (lactational) mastitis is the commonest breast infection.
Etiology: Predominantly Staphylococcus aureus (90%), occasionally Streptococcus. During lactation, cracked nipples allow bacterial entry; milk stasis promotes growth.
Pathogenesis: Bacteria ascend the lactiferous ducts → neutrophil infiltration → tissue necrosis → abscess formation. The abscess classically localises to one segment (unicentric) but can be multifocal.
Morphology: Grossly — tender erythematous quadrant, fluctuant if abscessed. Microscopically — interstitial and intraductal neutrophil infiltration, duct dilatation, fat necrosis if severe.
Clinical note: Treat with antibiotics; if fluctuant, incise and drain. Lactation need not cease.
Periductal (plasma cell) mastitis affects non-lactating women, often perimenopausally.
Etiology: Lipid material from desquamated duct epithelium leaks into periductal stroma → chemical irritant → intense inflammatory response. Squamous metaplasia of duct epithelium is an early precipitating event.
Pathogenesis: Duct obstruction by squamous debris → duct ectasia → rupture → periductal inflammation dominated by plasma cells (hence the name).
Morphology: Green/black nipple discharge; subareolar indurated plaque that can simulate carcinoma; nipple retraction (scar tissue). Microscopically — dilated ducts filled with secretions, periductal fibrosis, lymphocytes, plasma cells, and giant cells.
Clinico-pathological trap: Nipple retraction + subareolar mass = always exclude carcinoma. Triple assessment is mandatory.
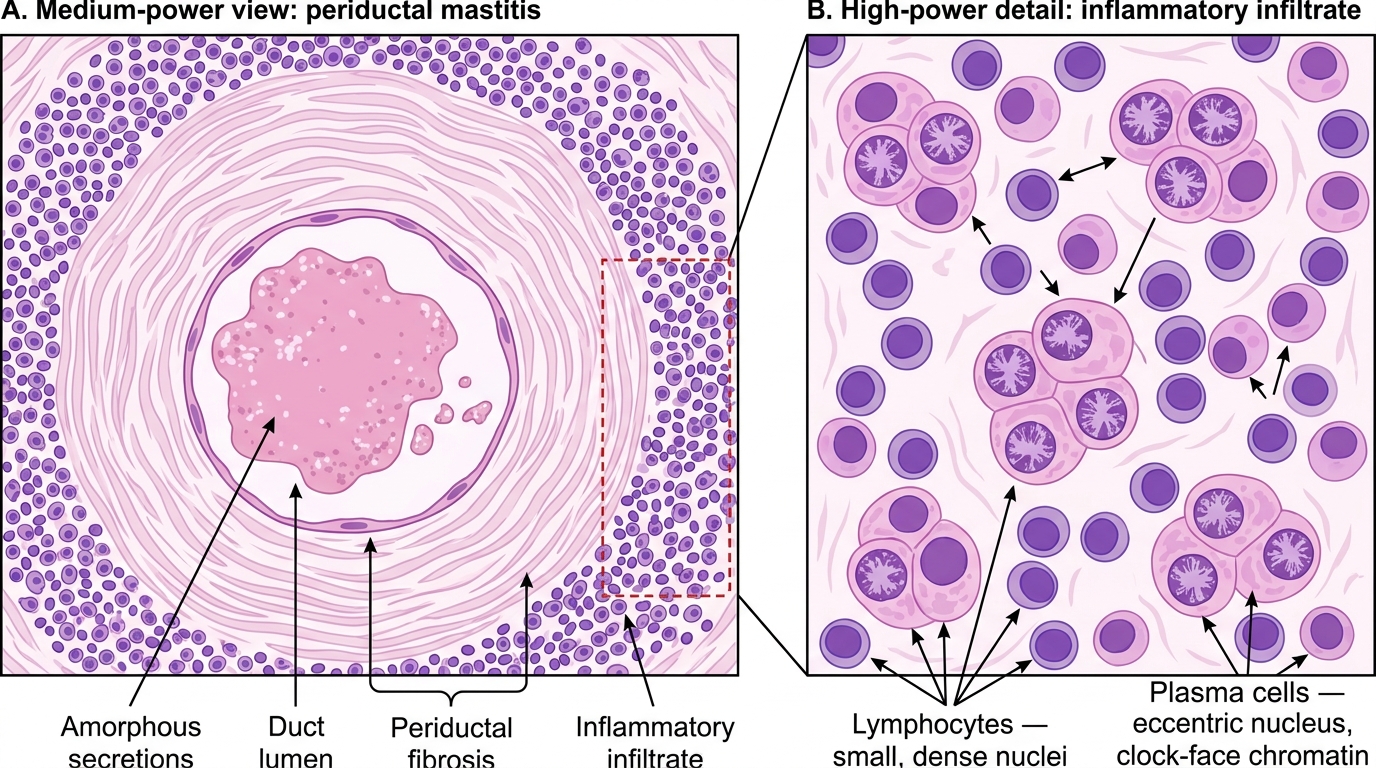
Histology of Periductal Mastitis (Medium Power with High-Power Inset)
Fat Necrosis
Fat necrosis is a reactive condition that closely mimics carcinoma clinically and radiologically — making it a classic examination and clinical trap.
Etiology: Trauma (most common, including surgical trauma/biopsy sites), radiation, vasculitis. A history of injury is obtained in only 50% of cases — the rest have subclinical microtrauma.
Pathogenesis: Adipocyte disruption → release of fatty acids and triglycerides → saponification (calcium soap formation) → inflammatory response → fibrosis.
Morphology sequence:
1. Early: haemorrhagic focus with necrotic adipocytes, neutrophil infiltration
2. Intermediate: foamy (lipid-laden) macrophages (lipophages) engulf debris; giant cells; haemosiderin
3. Late: fibrous scar; dystrophic calcification (appears as spiculated calcification on mammogram, indistinguishable from DCIS)
Clinical simulation of carcinoma: Hard, irregular, ill-defined mass; skin tethering (scar); calcification on imaging. Biopsy is essential.
Microscopic hallmark: Anucleate ghost adipocytes with eosinophilic granular cytoplasm, surrounded by lipophages and fibrosis.
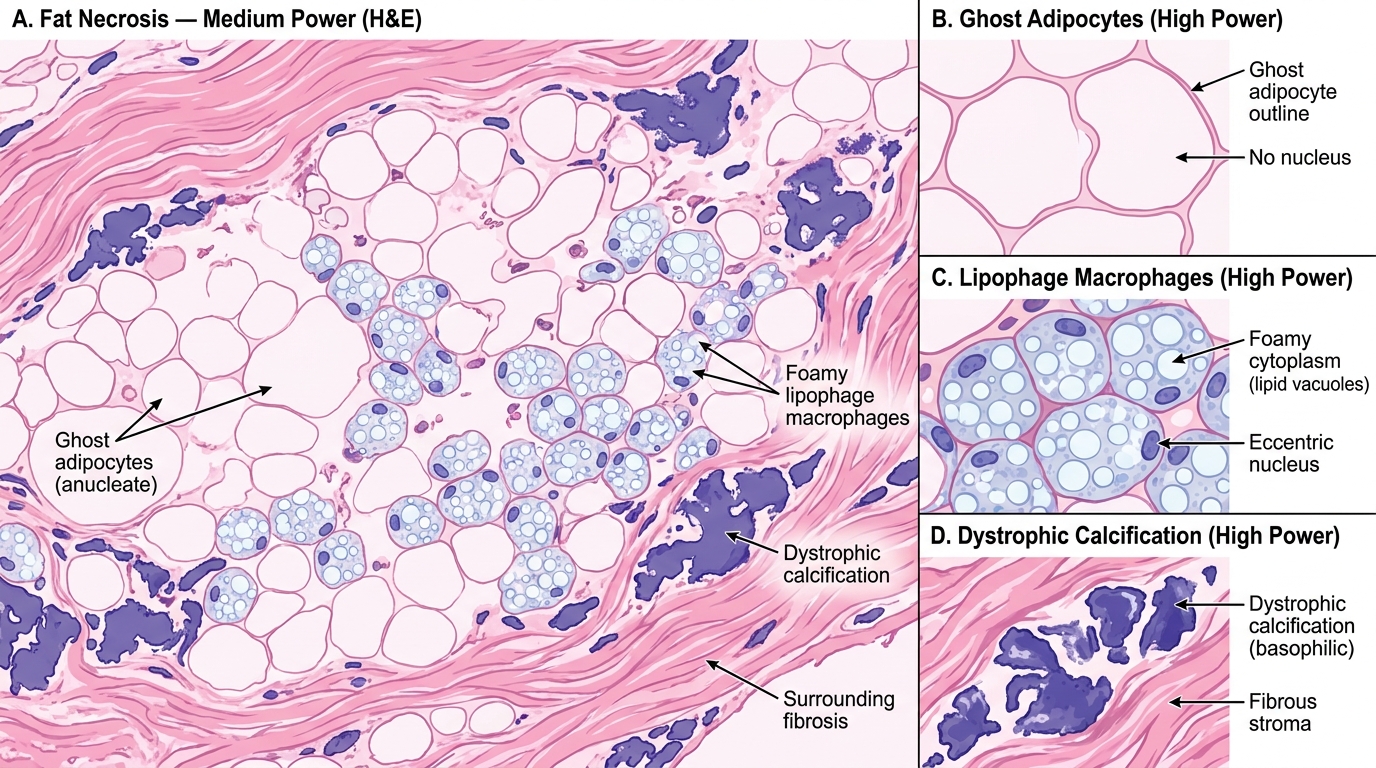
Fat Necrosis — Histological Features (H&E, Medium and High Power)
CLINICAL PEARL
The 'mimicker triad' of benign lesions that simulate carcinoma on imaging:
1. Fat necrosis — spiculated calcification, skin tethering
2. Periductal mastitis — subareolar mass, nipple retraction
3. Radial scar (complex sclerosing lesion) — stellate opacity on mammogram, central fibroelastosis
All three can only be reliably distinguished from carcinoma by histology. Knowing this protects both patient and doctor: never reassure a patient with a 'clinically benign' appearance without completing the triple assessment.